
Abstract
Goals of work
This study investigated physician’s attitudes toward the relative importance of chemotherapeutic and antiemetic efficacy in different clinical scenarios.
Materials and methods
Oncologists in the USA and four European countries completed an online stated-choice survey consisting of three hypothetical treatment choices for each of two patient types. Each hypothetical treatment alternative included both chemotherapy and antiemetic regimens. The two hypothetical patient types were (1) a 48-year-old woman with locoregional infiltrating ductal carcinoma of the breast and (2) a 78-year-old man with squamous cell carcinoma of the lung and multiple liver metastases. In each choice question, oncologists were asked to select the better combination of chemotherapy and antiemetic prophylaxis between two treatment alternatives.
Main results
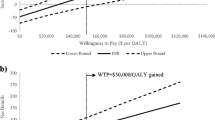
Five hundred fifty-seven oncologists completed the survey. For the adjuvant breast cancer patient, the most aggressive chemotherapy is consistently the most important treatment consideration in all countries. For the advanced lung cancer patient, the most aggressive chemotherapy, the less aggressive chemotherapy, and the most aggressive antiemetic prophylaxis are of similar importance in most countries.
Conclusions
Physicians appear more likely to prescribe a more aggressive chemotherapy regimen for a younger patient with a perceived curable tumor, regardless of the emetogenic properties of the chemotherapy. Symptom management is more of a concern and chemotherapeutic efficacy relatively less of a priority in an older patient with advanced disease for whom chemotherapy is not curative.



Similar content being viewed by others


References
American Cancer Society (2007) Global cancer facts and figures 2007. American Cancer Society, Atlanta, GA
Chew HK (2001) Adjuvant therapy for breast cancer: who should get what? West J Med 174(4):284–287, doi:10.1136/ewjm.174.4.284
Cronin DP, Harlan LC, Potosky AL, Clegg LX, Stevens JL, Mooney MM (2006) Patterns of care for adjuvant therapy in a random population-based sample of patients diagnosed with colorectal cancer. Am J Gastroenterol 101(10):2308–2318, doi:10.1111/j.1572-0241.2006.00775.x
Enger SM, Thwin SS, Buist DSM et al (2006) Breast cancer treatment among older women in integrated health care settings. J Clin Oncol 24(27):4377–4383, doi:10.1200/JCO.2006.06.3065
Grunberg SM, Osoba D, Hesketh PJ et al (2005) Evaluation of new antiemetic agents and definition of antineoplastic agent emetogenicity—an update. Support Care Cancer 13(2):80–84, doi:10.1007/s00520-004-0718-y
Hurria A, Naeim A, Elkin E et al (2007) Adjuvant treatment recommendations in older women with breast cancer: a survey of oncologists. Crit Rev Oncol Hematol 61(3):255–260, doi:10.1016/j.critrevonc.2006.09.002
Morrow GR, Hickok JT, Burish TG, Rosenthal SN (1996) Frequency and clinical implications of delayed nausea and delayed emesis. Am J Clin Oncol 19:199–203, doi:10.1097/00000421-199604000-00023
Owusu C, Lash TL, Silliman RA (2007) Effect of undertreatment on the disparity in age-related breast cancer-specific survival among older women. Breast Cancer Res Treat 102(2):227–236, doi:10.1007/s10549-006-9321-x
Ryan M, Ferrar S (2000) Using conjoint analysis to elicit preferences for health care. BMJ 320:1530–1533, doi:10.1136/bmj.320.7248.1530
Ryan M, McIntosh E, Schackley P (1998) Methodological issues in the application of conjoint analysis is health care. Health Econ 7:373–387, doi:10.1002/(SICI)1099-1050(199806)7:4<373::AID-HEC348>3.0.CO;2-J
Schleinitz MD, DePalo D, Blume J, Stein M (2006) Can differences in breast cancer utilities explain disparities in breast cancer care? J Gen Intern Med 21(12):1253–1260, doi:10.1111/j.1525-1497.2006.00609.x
Voliotis DL, Diehl V (1998) Clinical aspects and prognostic factors of nausea and vomiting after chemotherapy. In: Dicato M (ed) Medical management of cancer treatment induced emesis. Dunitz, London, UK, pp 45–54
Acknowledgements
This study was funded by GlaxoSmithKline, Inc., Collegeville, Pennsylvania. The views expressed herein do not necessarily reflect those of GlaxoSmithKline.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ettinger, D.S., Grunberg, S.M., Hauber, A.B. et al. Evaluation of the relative importance of chemotherapeutic and antiemetic efficacy in various oncologic settings. Support Care Cancer 17, 405–411 (2009). https://doi.org/10.1007/s00520-008-0501-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-008-0501-6