
Abstract
At the 2020 annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA), the International Dermatology Outcome Measures (IDEOM) Initiative Psoriasis (PsO) Working Group presented an update on its work to agree on meaningful, valid, and feasible outcome measures for PsO randomized controlled trials and longitudinal observational studies. The Treatment Satisfaction Working Group presented the development of a treatment satisfaction instrument to be utilized in PsO clinical trials. The Musculoskeletal Symptoms Working Group presented an overview of their work conducted to date to define how to best measure musculoskeletal symptoms in PsO clinical studies, and discussed next steps during an open-panel discussion, which included PsO and psoriatic arthritis experts.
- GRAPPA
- outcome measure
- psoriasis
- psoriatic arthritis
The International Dermatology Outcomes Measures (IDEOM) Initiative
Founded in 2013, the International Dermatology Outcomes Measures (IDEOM) Initiative is a nonprofit organization that aims to establish patient-centered measurements to enhance research and treatment for those with dermatologic disease,1 and to that aim, IDEOM established the Psoriasis (PsO) Working Group.2 After 4 years of continued work, the working group defined a core domain set for PsO clinical trials.3 This core domain set includes the domains of skin manifestations, investigator (IGA) and patient global assessment (PtGA), PsO, and psoriatic arthritis (PsA) symptoms, treatment satisfaction, and health-related quality of life.
To further identify appropriate outcome measures for each of the core domains, new working groups were then formed. In this report, we summarize the work that was presented at the 2020 Group for Research and Assessment of PsO and PsA (GRAPPA) annual meeting from the 2 working groups: “Treatment Satisfaction” and “Musculoskeletal (MSK) Symptoms” (previously known as “PsA Symptoms”).
Treatment Satisfaction Working Group Update by Dr. April W. Armstrong
Dr. April W. Armstrong presented an update on IDEOM and GRAPPA’s progress on the development of a treatment satisfaction instrument to be utilized in PsO randomized controlled trials (RCTs) and longitudinal observational studies (LOS). Treatment satisfaction was identified as one of 6 core domains, precipitating the need to identify the best treatment satisfaction instrument to be used in RCTs and LOS.3 The Treatment Satisfaction Working Group conducted a systematic literature review to evaluate existing treatment satisfaction tools. Eleven treatment satisfaction instruments were identified and critically appraised based on the quality of their measurement properties using the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) guidelines. The results of the systematic literature review revealed that there was no single instrument that was consistent in validity, reliability, feasibility, or responsiveness.4 Thus, IDEOM sought to develop a new treatment satisfaction instrument for PsO clinical trials.
Treatment satisfaction is defined as the degree to which the patient perceives that the treatment fulfills their health needs. Treatments have 2 key attribute categories: process attributes and outcome attributes. Process attributes refer to the location, frequency, duration, route of administration, formulation, and cost of the treatment. Outcome attributes refer to probability and magnitude of treatment benefits, time until treatment benefit, duration of treatment benefit, and the probability and reversibility of side effects due to the treatment. The decisional balance model of treatment satisfaction posits that a patient’s decision to continue or change treatments depends on the balance of factors from these 2 attribute categories.5 To encompass these important attributes, the IDEOM treatment satisfaction instrument items reflect effectiveness, convenience, and overall satisfaction with the treatment.
Dr. Armstrong also reviewed the efforts contributing to the latest draft of the IDEOM treatment satisfaction instrument. After conducting the systematic literature review as described above, the Treatment Satisfaction Working Group conducted nominal group discussions with patients who have PsO. Based on these discussions, questionnaire items were generated and categorized, with removal of duplicate items. An initial draft of the instrument was created and underwent extensive cognitive evaluation by IDEOM physicians, methodologists, and patients.
Finally, Dr. Armstrong presented the latest draft of the IDEOM treatment satisfaction instrument, which includes 7 items that are to be answered on a 5-point unipolar scale. The next step in development is the validation of the IDEOM treatment satisfaction instrument alongside an existing instrument in a larger population.
MSK Symptoms Working Group Update by Dr. Joseph F. Merola
Dr. Joseph F. Merola first provided an overview of the work conducted to date by the MSK Symptoms Working Group. “PsA symptoms” was identified in 2016 as a core domain to be measured in all PsO clinical trials.3 To define the measurement of PsA symptoms in this context, the working group conducted a Delphi consensus exercise involving 297 international stakeholders. Through this exercise, it was agreed that (1) all PsO trial participants should be screened for PsA with a validated screening tool prior to the measurement of PsA symptoms; (2) the measurement of PsA symptoms should occur in those who screen positive or have a prior rheumatologist diagnosis of PsA; and (3) the most appropriate instrument to measure PsA symptoms in PsO RCTs and LOS is the PsA Impact of Disease-9 (PsAID9), with the Routine Assessment Patient Index Data 3 (RAPID-3) representing an acceptable alternative.6,7
In an effort to further refine the applicability and validity of the PsA symptoms measurement, a new focus on the measurement of MSK symptoms has been established. A limitation of the PsA symptoms work includes the relatively low specificity of currently available PsA screening tools.8 Noninflammatory rheumatologic conditions, such as fibromyalgia and osteoarthritis, may be misclassified as PsA, for example. Ideally, all those who screen positive should be referred to a rheumatologist to confirm the diagnosis, but PsO studies are often carried out by nonrheumatologists and access to rheumatologists in this context is quite limited. Another limitation of the current PsA symptoms measures framework is that the PsAID9 and the RAPID-3 assume the presence of a diagnosis within question stems and have not been validated in the conduct of a PsO-limited study. Therefore, the content validity (i.e., the extent to which the instrument is relevant, comprehensive, and comprehensible to the study population, and the context of use) of these instruments may not be sufficient in patients with skin-limited disease.9 For example, the first question of the PsAID9 states: “Circle the number that best describes the pain you felt due to your psoriatic arthritis during the last week.”10 Patients with PsO without a formal diagnosis of PsA may be confused by the language used in this question and unable to reliably respond.
To overcome these challenges, the working group seeks to define how to measure MSK symptoms (e.g., pain, weakness, stiffness, fatigue) broadly in subjects with PsO in the context of PsO clinical studies. The identification and quantification of MSK symptoms in patients with PsO holds great potential to contribute to understanding the natural history of psoriatic disease. Indeed, as the overall prevalence of PsA in patients with PsO is 20%,11 the measurement of MSK symptoms may help to develop algorithms to predict which patients with PsO will transition into PsA, and to develop strategies to prevent its onset. We also know that up to 41% of patients not actively under the care of a rheumatologist have undiagnosed PsA,12 suggesting that many subjects’ symptoms are being missed for this reason as well. The measurement of MSK symptoms in the context of longitudinal cohort studies allows the potential effect of these therapies on MSK symptoms over time to be documented due to the availability of paired longitudinal data in clinical trials with longer-term follow-up registries.
To define how to measure MSK symptoms in subjects with PsO, the working group is currently working on 2 parallel projects: (1) exploring which MSK symptoms have been measured in previous PsO trials and registries, as well as the instruments that were used to measure them, and (2) developing an MSK Symptoms measure for PsO with input from patients with PsO and PsA.
Related to the first project, Drs. Lihi Eder, Alice Gottlieb, Philip Mease, Alexis Ogdie, Vibeke Strand, and Lourdes Perez-Chada presented their most recent work related to the measurement of MSK symptoms in PsO trials and registries.
Prodromal Presentation in PsA by Dr. Lihi Eder. Dr. Eder’s presentation aimed to: (1) provide evidence to support the existence of a prodromal phase in PsA, (2) describe the MSK symptoms that characterize this phase and their effect on healthcare utilization, and (3) review the potential role of imaging in optimizing the identification of patients who are at high risk for transitioning to PsA.
The observation that a prodromal phase does exist in PsA was triggered by dermatology reports describing how patients without prior diagnosis of PsA experienced an improvement in MSK symptoms following the initiation of biologic medications that were prescribed for their PsO. In a longitudinal study of a unique cohort of patients with PsO who were followed up prospectively over time, the presence of arthralgia in women, heel pain, fatigue, and stiffness were identified as the earlier symptoms associated with subsequent development of PsA in patients with PsO. In addition, the gradual worsening in the levels of pain, stiffness, fatigue, and physical function over time predicted the diagnosis of PsA.13
To further understand the effect of this prodromal phase of PsA, Eder and colleagues analyzed MSK-related healthcare utilization prior to the diagnosis of PsA in patients from primary care settings using electronic medical records and administrative data in Ontario, Canada.14 All cases were compared with age- and sex-matched comparators without inflammatory arthritis. The study outcomes included healthcare utilization and costs related to nonspecific MSK issues during a 5-year period prior to the index date. The study revealed that a substantial proportion of patients with PsA presented an increased number of visits to primary care physicians, MSK specialists, and emergency departments compared to matched controls. In addition, these patients evidenced a higher use of diagnostic imaging tests and procedures related to MSK symptoms. In all, this reflected that patients with PsA experienced MSK symptoms for a prolonged period prior to diagnosis of PsA and that this prodromal phase is associated with increased healthcare utilization and costs.
Diagnosing PsA is challenging due to the clinical heterogeneity of the disease, the lack of reliable objective biomarkers, and often the lack of distinct clinical findings suggestive of PsA.13 MSK ultrasound is an affordable and accessible imaging modality that, in expert hands, is more reliable than physical examination in the assessment of MSK abnormalities. Therefore, it has the potential to optimize early diagnosis of PsA at early stages of disease.15,16
In a cross-sectional study involving 203 patients with PsO who were experiencing MSK complaints and did not have a prior diagnosis of PsA, patients were classified by a rheumatologist as “Not PsA,” “Possibly PsA,” or “PsA” after a clinical assessment, which was considered the gold-standard diagnosis.17 In addition, a targeted MSK ultrasound was conducted, and patients completed questionnaires about their MSK symptoms and other patient-reported outcome measures (PROMs). Results were then compared between patients with PsA and Possibly/Not PsA. While the distribution and duration of MSK symptoms between groups was comparable, patients with PsA had worse fatigue, physical function, and quality of life scores. When comparing the performance of ultrasound vs rheumatologist diagnosis, ultrasound was shown to be very sensitive (83%), though not highly specific (52%). This finding is likely explained by the fact that ultrasound was detecting more inflammation than the rheumatologist’s clinical assessment. In fact, almost half of the patients that were found to have positive ultrasound inflammation were not classified as having PsA by the rheumatologist. Possibly, these underdetected cases consisted of patients in early phases of the disease, in whom the clinical findings were too subtle to be detected by rheumatologists.
In summary, a significant proportion of patients that will develop PsA experience a prodromal phase that is associated with higher healthcare utilization and costs. Ultrasound and other imaging modalities may optimize the identification of these patients who are at high risk of progressing from PsO to PsA.
Utility of PsAID12 in the Corrona PsO Registry by Dr. Alice B. Gottlieb. Dr. Gottlieb presented data from the Corrona PsO Registry to support the utility of the PsAID12 in a real-world PsO cohort. The Corrona PsO Registry is a prospective multicenter, observational, disease-based registry that included 5326 patients as of August 10, 2018. Of these patients, 1438 had a physician-reported diagnosis of PsA or had screened positive for PsA as measured by the PsO Epidemiology Screening Tool (PEST).18 In this study, the PsAID12 was emailed or mailed to these patients to be completed at home. In all, 439 (30.5%) of these patients completed the questionnaire, 370 were diagnosed with PsA, and 69 were PEST-positive. The scores of the PsAID12 were then correlated with PsO severity and other PROMs from the nearest available study visit (mean time elapsed between the Corrona visit and the PsAID12 was 2.2 ± 5 months). The mean age of patients was 56 ± 12 years, 54% were women, and the mean PsO duration was 20 ± 16 years. The PsAID12 presented moderately positive correlations (r = 0.32-0.62) with IGA, body surface area (BSA) affected by PsO, IGA × BSA, Psoriasis Area and Severity Index (PASI), Dermatology Life Quality Index, and Work Productivity and Impairment questionnaires, as well as the fatigue visual analog scale (VAS), skin pain VAS, itch VAS, joint pain due to PsA VAS, PtGA-VAS, and EuroQol EQ-5D domains. Moderate negative correlations were observed between PsAID12 and the 3-level EQ-5D (EQ-5D-3L) health state (VAS) and EQ-5D-3L index.
To conclude, this is the first largescale PsO registry to assess PsA symptoms using the PsAID12. This instrument may be a valid PsA symptoms outcome measure for dermatology clinical practice and real-word registries.
Assessing MSK Pain in a Phase II PsO Trial (Tyrosine Kinase 2 Inhibitor—BMS-986165) by Dr. Philip J. Mease. Deucravacitinib is a potent and highly selective oral tyrosine kinase 2 (TYK-2) inhibitor. TYK-2 is a member of the Janus kinase family that mediates cytokine signaling, especially interleukin (IL)-23, IL-12, interferon (IFN)-α, and IFN-ß.19 Dr. Mease presented a substudy, which assessed MSK pain improvement in a phase II RCT to assess the efficacy and safety of deucravacitinib in patients with moderate-to-severe plaque PsO.20,21 In this substudy, the percentage change in “pain” in patients who had MSK symptoms at baseline was evaluated as an exploratory endpoint. MSK pain was used as a possible surrogate for MSK pain response in PsA. Pain was measured on a 100-mm VAS: “How much pain have you had because of your condition over the past week?” Scores ranged from 0 (no pain) to 100 (worst pain). Of note, the question did not specifically ask about PsA pain. Demographics and baseline characteristics for the subpopulation of patients who had MSK symptoms at baseline were similar to the overall study population. Nonlinear mixed-effects exposure-response models showed that deucravacitinib (given twice/d) demonstrated dose-dependent improvements in pain VAS scores in patients with PsO who had baseline MSK symptoms. In a subanalysis, improvements in pain VAS did not correlate with improvements in skin as measured by the PASI score. Therefore, patients with PsO treated with this TYK-2 inhibitor may experience a reduction in pain from MSK manifestations independently of skin improvements. This study provided support for evaluating deucravacitinib in a dedicated PsA trial.
RAPID-3 in the Vascular Inflammation in Psoriasis Trial by Dr. Alexis Ogdie. The RAPID-3 is a patient-reported disease activity measure developed for patients with rheumatoid arthritis (RA) for use in clinical care, although it may also be useful in clinical research. After initial validation in patients with RA, its use has been extended to other rheumatologic conditions, including PsA.22,23 RAPID-3 is a simple arithmetic composite index of 3 patient self-report measures: physical function on a Health Assessment Questionnaire, pain, and patient global estimate status. Each self-report is scored from 0 to 10; raw scores range from 0 to 30.22
In the Vascular Inflammation in PsO trial, 46 patients with PsO and 16 comparators with PsA completed the RAPID-3 questionnaire. Baseline characteristics between patients with PsO and patients with PsA were similar in mean age (43.3 ± 14 vs 44.8 ± 12, respectively), mean BMI (32.5 ± 8.5 vs 30.3 ± 6.1, respectively), mean age at PsO onset (25 ± 13.5 vs 26.2 ± 12.2 yrs, respectively), PsO duration (18.2 ± 17.5 vs 17.3 ± 11 yrs, respectively), and female sex (69% vs 56%, respectively). Remarkably, mean scores for each of the individual components of the RAPID-3, as well as the total RAPID-3 score, were also very similar among the groups. It was surprising to see that patients with PsO reported higher pain scores (mean pain = 4 ± 3.2) than patients with PsA (mean pain = 3.4 ± 2.7). To understand whether this finding was driven by joint pain, RAPID-3 pain scores were compared between patients who reported joint pain and those who did not. Interestingly, patients with PsO alone who reported joint pain had similar scores in the PtGA, pain assessment, and total RAPID-3 compared to those who did not report joint pain. In addition, BSA did not seem to explain RAPID-3 scores, either, as these measures correlated poorly in a subanalysis.
In conclusion, patients with PsO have similar scores to patients with PsA on the RAPID-3, even among those without joint pain. RAPID-3 may capture pain other than joint pain, and it remains unclear how skin disease may affect the scores of PsA measures.
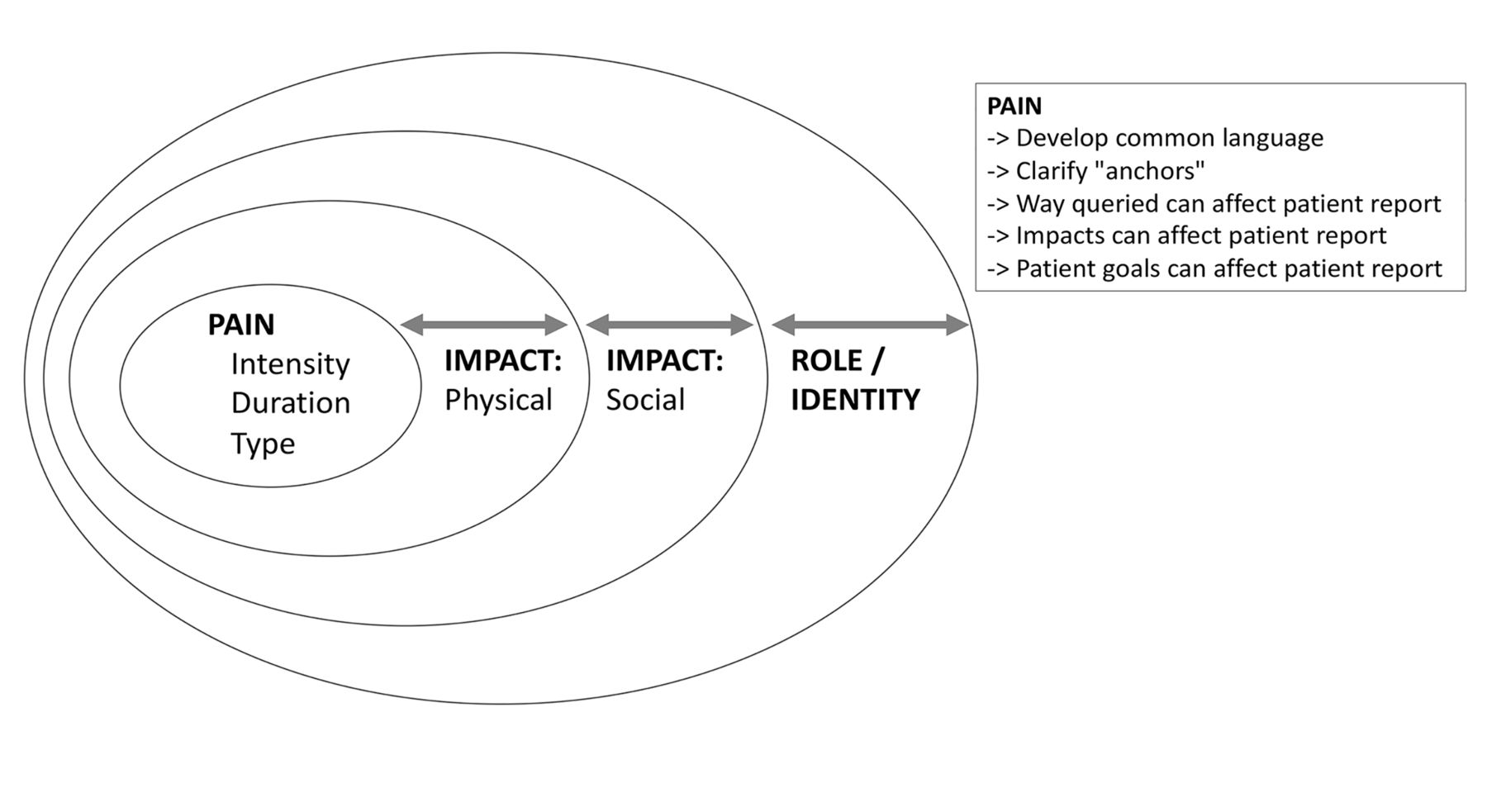
Do We Know Which Pain Outcomes are Meaningful to Patients by Dr. Vibeke Strand. Dr. Strand presented a summary of a planned presentation at a future workshop conducted by Outcome Measures in Rheumatology (OMERACT) about how to measure pain and what to measure. Traditional pain measurement scales, such as the pain VAS, pain numerical rating scale (NRS), and the pain rating scale, focus on measuring pain intensity.24 While the validity, responsiveness, and clinically meaningful changes for such pain intensity scales have been previously demonstrated,24,25,26 qualitative research has shown that patients report pain intensity using idiosyncratic methods.2 Indeed, patients consider other pain features, such as sensations, experience, duration, and impact, and they do not use intensity scales in a linear manner.27 Therefore, the working group questioned whether validated thresholds of pain improvement, such as > 30% or > 50% of pain relief, are truly meaningful to patients and whether they can actually distinguish between distinct states of pain other than “pain” vs “no pain.” In addition, the working group discussed the contribution of central sensitization to chronic pain in rheumatic conditions and how to best evaluate it. In summary, pain intensity, duration, and type are certainly important features, but pain’s impact on social, physical, and emotional well-being (role, identity) are also critical (Figure 1). Further research and discussions are warranted to agree on how to better query pain in rheumatologic conditions.

Pain taxonomy and its effect on 3 domains (physical, social, and role/identity).
Measurement of MSK Symptoms in PsO Trials Registered on ClinicalTrials.gov by Dr. Lourdes M. Perez-Chada. Dr. PerezChada presented the preliminary results of an ongoing study focused on identifying MSK symptoms measured in PsO RCTs and LOS. In this study, 2 independent reviewers searched for the study protocols of all phase III and IV PsO trials published on ClinicalTrials.gov. Next, investigators screened all identified protocols to determine primary or secondary endpoints targeting the measurement of MSK symptoms in patients with PsO. In all, 490 phase III and IV PsO RCTs were identified. Of these, only 33 trials included the measurement of MSK symptoms as a primary or secondary endpoint. Among the 33 identified protocols, the vast majority had used the Medical Outcomes Study 36-item Short Form Health survey,28 and only a few studies had used more specific MSK symptoms measures, such as a joint pain score, tender and swollen joint count, or physician global assessment of arthritis. Of note, several studies reported the use of generic pain VAS or NRS scores (i.e., not joint- or MSK-specific). In the context of a PsO study, the score from such generic measures may be difficult to interpret because patients may experience skin pain, joint pain, or both. Next steps involve extracting and analyzing study results from ClinicalTrials.gov and from full-text articles related to the study protocols published in the PubMed database.
Open-panel Discussion to Identify Next Steps
Finally, Dr. Merola and Dr. Armstrong moderated an open-panel discussion for the next steps and items for the research agenda related to the diagnosis/classification of PsA in PsO RCTs and the measurement of MSK symptoms in patients with PsO (Figure 2). In addition, Dr. Merola and Dr. Gottlieb introduced a treatment algorithm for patients with PsO for use in clinical practice based on the measurement of MSK symptoms (Figure 3). Mirroring the agreed upon approach for PsO clinical trials, patients with PsO would first be asked about a rheumatologist diagnosis of PsA and screened for PsA using a validated screening tool. Those who have a rheumatologist diagnosis of PsA or who screen positive for PsA would then receive a PsA/MSK symptoms measure, and the score of the instrument would guide treatment decisions. Specifically, the validated cutoff value for a Patient Acceptable Symptom State (PASS) has previously been published for the PsAID9 and PsAID12.10 If a patient’s PsAID score is ≤ 4 (acceptable symptom state), the patient should be continued on the same therapy. If the PsAID score is > 4 (unacceptable symptom state), then therapy modification and/or comanagement/referral to a specialist should be considered. This is particularly valuable in the hands of the nonrheumatologist, as a patient-completed questionnaire places low burden on the provider. As other MSK symptoms measures are developed and/or validated for PsO, cutoff values for a PASS state will need to be determined in order to apply the algorithm.

Discussion points raised during the open-panel discussion. IDEOM: International Dermatology Outcome Measures.

{kind=link}
{kind=link}
{kind=link}
IDEOM’s working treatment algorithm for PsO in clinical practice. * Based on validated cutoff values for patient acceptable symptoms state (PASS). IDEOM: International Dermatology Outcome Measures; PsA: psoriatic arthritis; PsO: psoriasis; PEST: Psoriasis Epidemiology Screening Tool; MSK: musculoskeletal; PsAID: Psoriatic Arthritis Impact of Disease.
Conclusion
Herein, we provided an update on IDEOM’s work presented at the GRAPPA 2020 Annual Meeting. IDEOM’s PsO Treatment Satisfaction Working Group developed a treatment satisfaction instrument, which includes 7 items that are to be answered on a 5-point unipolar scale. Next steps involve conducting a validation study to confirm its validity, reliability, responsiveness, and feasibility. Meanwhile, IDEOM’s MSK Symptoms Working Group’s efforts are centered on identifying how to best measure MSK symptoms in patients with PsO. The working group will continue working on 2 main projects: (1) to explore which MSK symptoms have been measured in previous PsO trials and registries and the instruments that were used to measure them; and (2) to develop an MSK symptoms measure for PsO. Progress of their efforts was presented at the 2020 IDEOM Annual Meeting.
Footnotes
As part of the supplement series GRAPPA 2020, this report was reviewed internally and approved by the Guest Editors for integrity, accuracy, and consistency with scientific and ethical standards.
This paper does not require institutional review board approval.
- Copyright © 2021 by The Journal of Rheumatology
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.