
Abstract
Objective. To systematically review the efficacy and safety of on-demand versus continuous use of nonsteroidal antiinflammatory drugs (NSAID) in patients with inflammatory arthritis and to assess if longterm continuous treatment with NSAID in comparison with NSAID treatment on-demand reduces radiographic progression.
Methods. A systematic literature review was performed in Medline, Embase, the Cochrane Library, and American College of Rheumatology/European League Against Rheumatism 2008–2009 meeting abstracts as part of the multinational 3e (Evidence, Expertise, Exchange) Initiative for generating practical recommendations about Pain Management by Pharmacotherapy in Inflammatory Arthritis. Articles fulfilling predefined inclusion criteria were reviewed and quality appraisal was performed.
Results. The search yielded a total of 1410 articles from Medline and Embase, 73 from Cochrane Central, and 3 meeting abstracts. After review, only one study fulfilled the defined inclusion criteria, which indicated that longterm continuous treatment with NSAID versus NSAID treatment on-demand reduced radiographic progression in patients with ankylosing spondylitis. Secondary measured endpoints were disease activity measures including pain and the frequency of observed adverse events in both groups. Relevant adverse events tended to occur more frequently in the continuous treatment group with odds ratios of 2.79 for hypertension, 1.67 for abdominal pain, 1.35 for diarrhea, 0.95 for dyspepsia, and 3.2 for depression. None of these differences were statistically significant, with the exception of depression, which could not be explained.
Conclusion. Based on a single study, there does not seem to be a statistical difference in efficacy between the on-demand versus continuous use of NSAID in the context of ankylosing spondylitis. There were no studies in patients with rheumatoid arthritis, psoriatic arthritis, or spondyloarthritis. Research is needed to study the risk-benefit ratio of continuous versus on-demand use of NSAID.
- NONSTEROIDAL ANTIINFLAMMATORY DRUGS
- CONTINUOUS
- ON-DEMAND
- INFLAMMATORY ARTHRITIS
Nonsteroidal antiinflammatory drugs (NSAID) are recommended as first-line treatment in patients with inflammatory arthritis. Relief of pain and stiffness in patients with inflammatory back pain has been well established. Recent concerns about the longterm safety of NSAID raised the possibility that on-demand use might lead to a better risk/benefit ratio as compared to continuous use. Few studies, however, have compared the efficacy and safety profile of continuous versus on-demand NSAID use in the inflammatory arthritis population. The objective of this study was to systematically review the available literature to answer this question.
MATERIALS AND METHODS
A systematic literature review (SLR) was carried out in several steps following the updated guidelines for Cochrane systematic review1. The review was part of the multinational 3e (Evidence, Expertise, Exchange) Initiative for generating practical recommendations about Pain Management by Pharmacotherapy in Inflammatory Arthritis2. In our review we addressed the question, “Is there a difference in efficacy and safety between on demand and continuous use of NSAID in inflammatory arthritis?”.
Rephrasing the question
When conducting a SLR, the first step is to translate the question into an epidemiological question following the PICO method (Patients, Intervention, Comparator, Outcome). The population was defined as patients over 18 years of age with an established diagnosis of rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis (AS), or spondyloarthritis. The intervention group consisted of the continuous use of NSAID for a period of more than 2 weeks, whatever the dose or route of administration; the control group was the on-demand use of NSAID. Defined outcomes included decrease in pain and development of any adverse event (AE) during the use of NSAID. Optimal study scenarios to be included were randomized controlled trials, pseudo-randomized controlled trials, controlled before-and-after studies, and cohort studies. Studies were excluded that compared the clinical activity of various NSAID only or addressed the side effects or safety profiles of specific NSAID.
Literature search
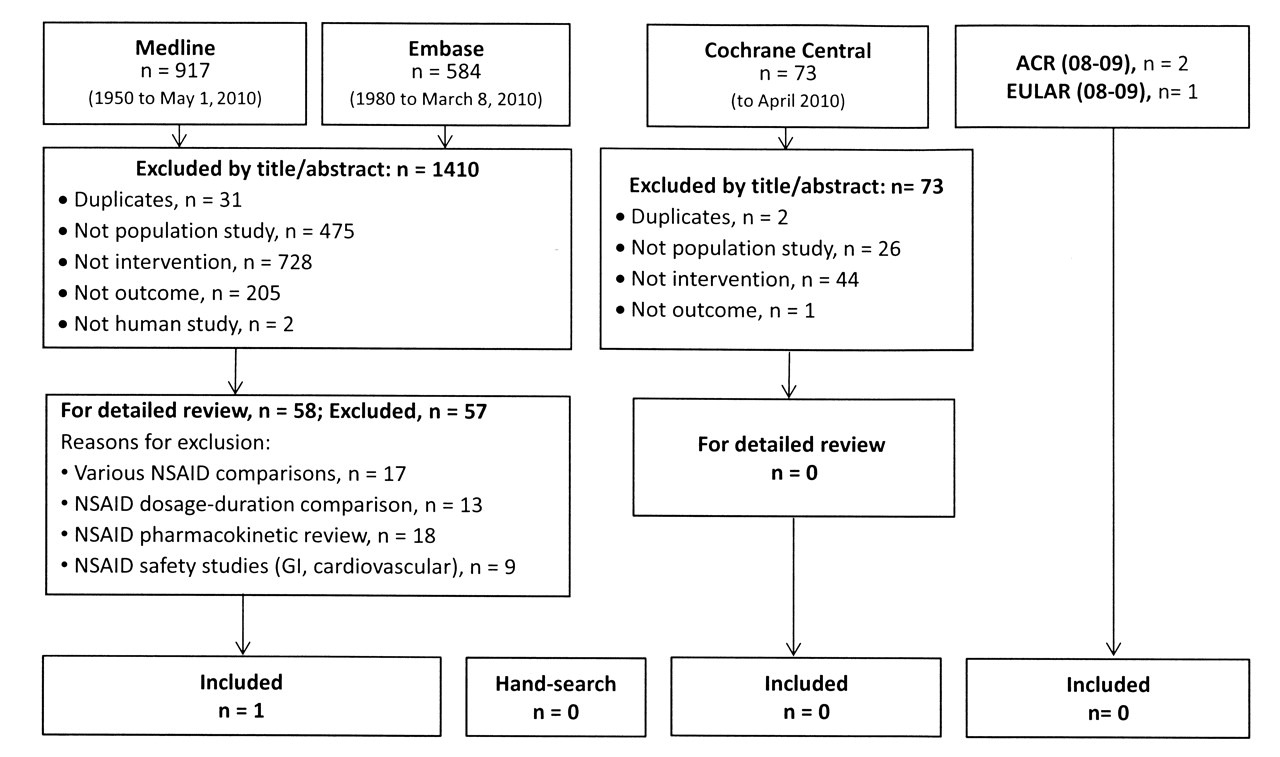
A systematic literature search was performed in Medline (1950 to the 4th week of April 2010), Embase (1980 to the 10th week of 2010), and the Cochrane Library using a comprehensive search strategy developed in collaboration with 2 experienced librarians (for details see the online Appendix available from www.3epain.com). We also searched European League Against Rheumatism (EULAR) 2008–2009 and American College of Rheumatology (ACR) 2008–2009 meeting abstracts, and examined review articles to identify additional studies by hand-searching reference lists. Figure 1 depicts the results of our literature search.
{kind=link}
Literature search from which 58 articles were selected for detailed review. One article met the inclusion criteria.
Study selection
Relevant articles were selected following a systematic procedure. Titles and abstracts of all the references were screened, excluding articles that did not address the studied topic. All selected articles were then reviewed as full articles, applying the inclusion criteria defined by the PICO method. Articles that did not fulfill all the inclusion criteria were excluded. The level of evidence of each study was assessed according to the Oxford Centre for Evidence-based Medicine3.
RESULTS
After removal of duplicates, a total of 1483 references were identified, 73 of which were from Cochrane Central. Seven meeting abstracts were also identified. After title and abstract screening, 58 articles were retrieved for full article review, of which only one study fulfilled the inclusion criteria4. No meeting abstracts or additional hand-search reports were included.
The included article was a low risk of bias randomized clinical trial published in 2005. The objective of the study was to test the hypothesis that longterm, continuous treatment with NSAID, in comparison with NSAID treatment on demand only, influences radiographic progression in patients with AS. Secondary endpoints were disease activity measures including pain and the frequency of observed AE in both groups. The study group included 215 patients, 111 of whom were randomized to the continuous-treatment group and 104 randomized to the on-demand group. Ninety-six patients in the continuous-treatment group completed the study, 68 of whom were taking celecoxib and 28 a different NSAID. Reasons for withdrawal of the 15 patients were inefficacy (n = 8), AE (n = 2), moving to another city or country (n = 2), and unknown (n = 3). In the on-demand treatment group, 86 patients completed the study, 67 of whom were taking celecoxib and 19 a different NSAID. Withdrawal reasons for the remaining 17 patients were inefficacy (n = 8), AE (n = 3), moving to another city or country (n = 2), and unknown (n = 4). Mean daily dose of celecoxib was 243 ± 59 mg in the continuous-treatment group and 201 ± 93 mg in the on-demand group, with a mean difference of 42 mg (95% CI 21—63, p = 0.0001).
Disease activity was stable over time in both groups, reflected by 4 disease activity variables: Bath Ankylosing Spondylitis Disease Activity Index, global pain [by visual analog scale (VAS)], C-reactive protein, and patient global assessment (by VAS). Results confirmed the initial general impression of somewhat higher disease activity in the on-demand group compared with the continuous-treatment group; the difference, however, was not statistically significant for any variable. Although there was no statistical difference between the 2 groups regarding disease activity, a trend towards less global pain and fewer painful days was noted in the continuous-treatment group.
Overall, 22 episodes of AE were reported by 22 patients (19.8%) in the continuous-treatment group, and 25 times in 16 patients (15.5%) in the on-demand group. Only one of these serious AE (a case of severe abdominal pain requiring hospital admission in the on-demand group) was considered related to the study medication.
The most important and frequently occurring AE were hypertension 9% versus 3% (OR 2.79, p = 0.12), abdominal pain 11% versus 6% (OR 1.67, p = 0.28), diarrhea 19% versus 13% (OR 1.35, p = 0.28), and dyspepsia 41% versus 38% (OR 0.95, p = 0.65). The only statistically significant difference in event outcomes was in occurrence of depression, with 14% in the continuous group versus 4% in the on-demand group (OR 3.2, p = 0.03). No explanation was provided to account for this statistically significant difference between the groups.
DISCUSSION
Based on this single low risk of bias study, there does not seem to be a statistical difference in efficacy between the on-demand versus continuous use of NSAID in the context of AS. Although not statistically significant, the results of the included study did confirm the impression of somewhat higher disease activity, including pain data, in the on-demand group compared to the continuous-treatment group. There was no statistical difference in the safety profile during continuous versus on-demand use of NSAID in the context of AS, with the exception of higher occurrence of depression in the continuous-use group. This statistical difference could not be explained by a pathophysiological hypothesis.
In conclusion, the question of the safety of continuous use of NSAID versus on-demand use in inflammatory arthritis could not be answered conclusively with our systematic review as only one study in AS was included. In this study, no safety issues were noted except for a higher rate of depression. However, the study was relatively small to ascertain similar safety with a high level of confidence. There were no studies in patients with rheumatoid arthritis, psoriatic arthritis, or spondyloarthritis. Future research is needed to study the risk-benefit ratio of continuous versus on-demand use of NSAID.
Acknowledgments
The authors thank all the members of the 3e scientific committees, the participants of the national meetings, and the support from Margaux Orange. A special acknowledgment is also directed to Amy Faulkner and Louise Falzon, information specialists at the University of Toronto and Cochrane Central, respectively.
REFERENCES
- 1.
- 2.
- 3.
- 4.