
Abstract
Chronic disabling conditions, such as immune-mediated inflammatory diseases (IMID), adversely affect patients in terms of physical suffering and pain, impaired function, and diminished quality of life. These persistent relapsing diseases have a significant influence on individual employment status and work-related productivity. In addition to the significant burden on patients and their families, IMID represent a sizable burden to society due to high healthcare and non-healthcare related costs. Non-healthcare related, or indirect, costs — primarily associated with decreased work productivity, disability payments, and early retirements — are typically greater contributors than direct healthcare costs to the total costs associated with IMID. This article discusses the socioeconomic impact of several IMID, including rheumatoid arthritis, inflammatory bowel disease, ankylosing spondylitis, and psoriasis.
- COST OF ILLNESS
- INFLAMMATORY BOWEL DISEASE
- RHEUMATOID ARTHRITIS
- ANKYLOSING SPONDYLITIS
In the past few years, an abundance of studies have investigated the socioeconomic burden of various immune-mediated inflammatory diseases (IMID)1,2,3,4,5,6. The longterm outcomes of available therapies, including tumor necrosis factor-α (TNF-α) inhibitors, have also been presented7,8,9,10,11,12. Direct (i.e., healthcare) costs associated with some IMID, as pointed out by these studies, have traditionally been dominated by inpatient care, mostly surgery2,3. With the advent of TNF-α inhibitors, which are both more effective in delaying or preventing the need for surgery and hospitalization and more costly than conventional pharmacotherapies, the majority of direct costs are shifting toward drug treatments2,3. Costs incurred by individuals and society outside those related to the healthcare system are referred to as indirect costs (unless otherwise indicated, monetary values given in this review are expressed in Canadian dollars). Nonprescription medications, transport to and from medical appointments, and household support are examples of the extra costs incurred by individuals. Societal costs involve factors such as worker absences, reduced productivity due to disability, and early retirement. Most IMID affect people in their prime working years, with considerable effect on employment behavior. Indeed, the total costs associated with IMID are dominated by work disability. Due to their chronic and disabling nature, IMID greatly affect patients’ ability to perform work-related tasks, which can translate into substantial employer costs.
A wealth of recent literature describes the negative effects of IMID in the workplace and documents the substantial consequence of these conditions on employers2,3,4,5,13,14,15,16. Researchers consistently found that employees with IMID were more likely to be absent from work, used sick days, required disability, and retired early compared to healthy controls. Further, even when at work, the individuals with IMID are generally less productive than average employees because of frequent breaks and slower working pace due to pain and reduced mobility. This loss of productivity, also referred to as presenteeism, causes another significant but poorly studied burden to employers.
INFLAMMATORY BOWEL DISEASE (IBD) AND ITS INFLUENCE ON EMPLOYMENT STATUS AND WORK-RELATED PRODUCTIVITY IN CANADA AND THE USA
Although most patients with IBD have had the disease for most of their adult life, those with milder forms may experience long periods of fairly normal health interrupted with occasional relapses. This may allow them to hold full-time jobs, with some absences for sick leave or medical checkups. Individuals with more severe disease, however, may have no choice but to cut their working hours, change their type of employment, or eventually stop working altogether.
According to the Crohn’s and Colitis Foundation of Canada (CCFC), almost 201,000 individuals in Canada were diagnosed with IBD in 20082. Conservatively estimated costs associated with these cases were in the range of $1.8 billion/year, or over $9000/year per individual with IBD. Indirect costs were over $1 billion/year (Figure 1). Further, it is estimated that 43% of employees with IBD require time off work due to the disease, averaging 7.2 days per employee with IBD per year. This translates into a cost of $138 million per year (costs are in US dollars or Canadian dollars where appropriate) in short-term work losses for 120,500 actively employed Canadians with IBD in 2008 (Table 1). In regard to longterm work loss, it is estimated that individuals with IBD have a reduction of 3%–13% in employment rate. Longobardi, et al15 applied a labor force participation model to US national health survey data to determine the effect of IBD on employment. Almost one-third (31.5%) of individuals who had experienced IBD symptoms in the past year reported being out of the workforce. This percentage was significantly greater than the 18.5% rate reported by people with IBD but without symptoms, or the 14.8% reported by the non-IBD group. This indicates that during disease flares individuals with IBD were more than twice as likely to be out of the labor force as those without IBD. Investigators also pointed to the presence of IBD symptoms as a key indicator of the reduced ability of these patients to work.

Indirect costs associated with inflammatory bowel disease in Canada by type of cost. Indirect costs were estimated at $1.064 billion in Canada in 2008 ($595 million for Crohn’s disease and $469 million for ulcerative colitis). Adapted with permission from Crohn’s and Colitis Foundation of Canada. The burden of inflammatory disease in Canada; 20082.
Short-term work losses due to inflammatory bowel disease (IBD) in Canada in 2008. Reproduced with permission from the Crohn’s and Colitis Foundation of Canada. The burden of inflammatory bowel disease (IBD) in Canada; 20082.
SOCIOECONOMIC BURDEN OF RHEUMATOID ARTHRITIS (RA)
As a chronic and debilitating disease that affects about 2% of adults in North America, RA poses a significant burden to patients, their caregivers, employers, and the government17,18. Work disability often arises early in the course of the disease. According to several prospective studies, 20%–35% of individuals had to stop working within 2–3 years after disease onset19,20,21. After 5–10 years, the reported work disability rates are approximately 40%13,20.
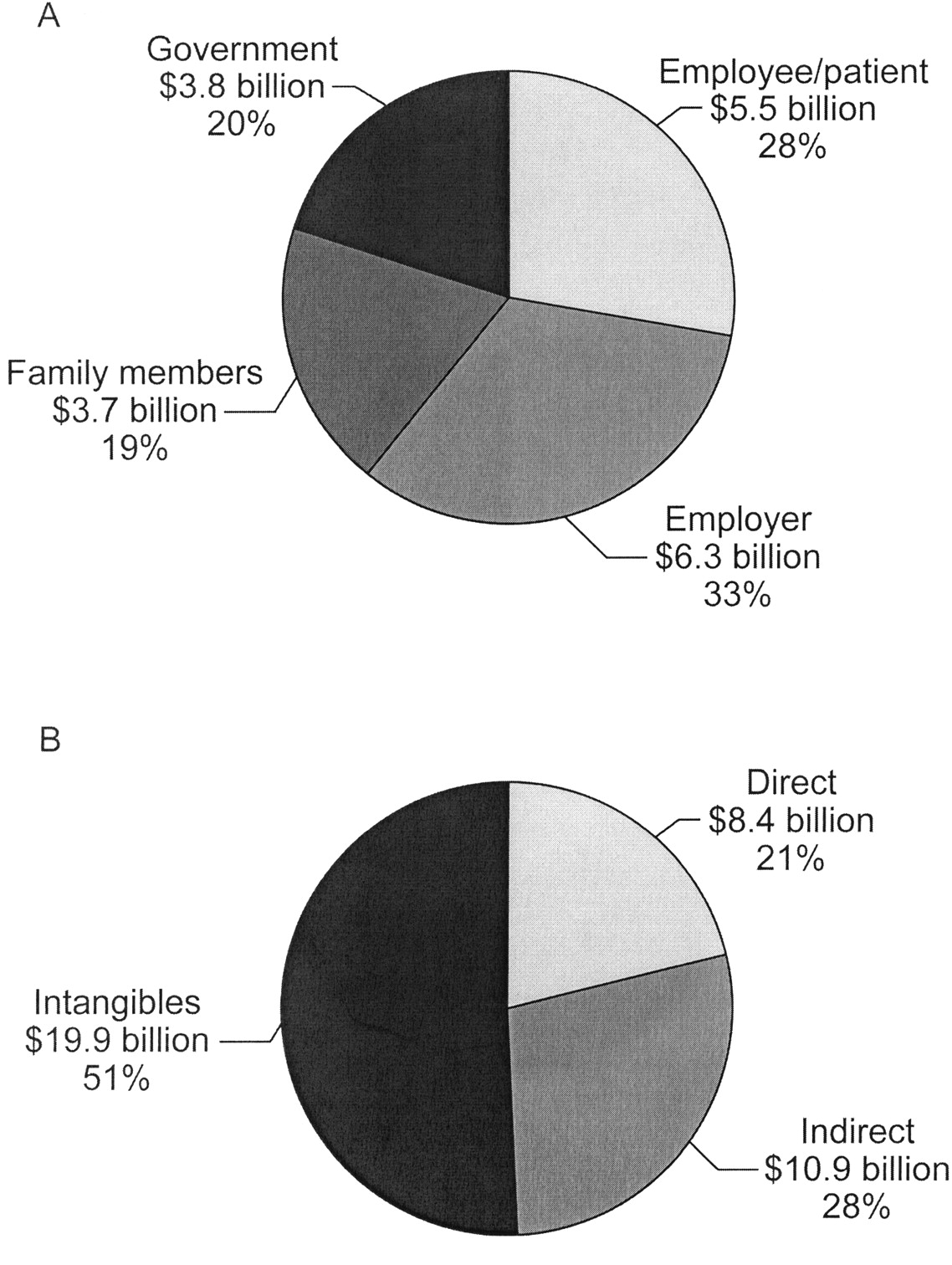
From an employer’s standpoint, the effects of RA include employer-paid direct healthcare costs — drug costs, work loss costs (i.e., disability, absenteeism), productivity loss (i.e., presenteeism), and adaptation costs to help individuals with RA remain in the workforce (i.e., special keyboards, tools, etc.) — as well as cost of replacing workers with RA required to leave the workplace5,22,23. Using administrative claims databases covering privately insured patients as well as Medicare and Medicaid beneficiaries, Birnbaum, et al5 estimated the excess payer and beneficiary-paid costs of RA in the USA annually to total $19.3 billion; 33% of the total cost was paid by employers, 28% by patients, 20% by government, and 19% by family members (Figure 2A). Addition of intangible costs such as quality of life (QOL) and premature mortality to the equation increased the total RA costs to $39.2 billion per year (Figure 2B)5.
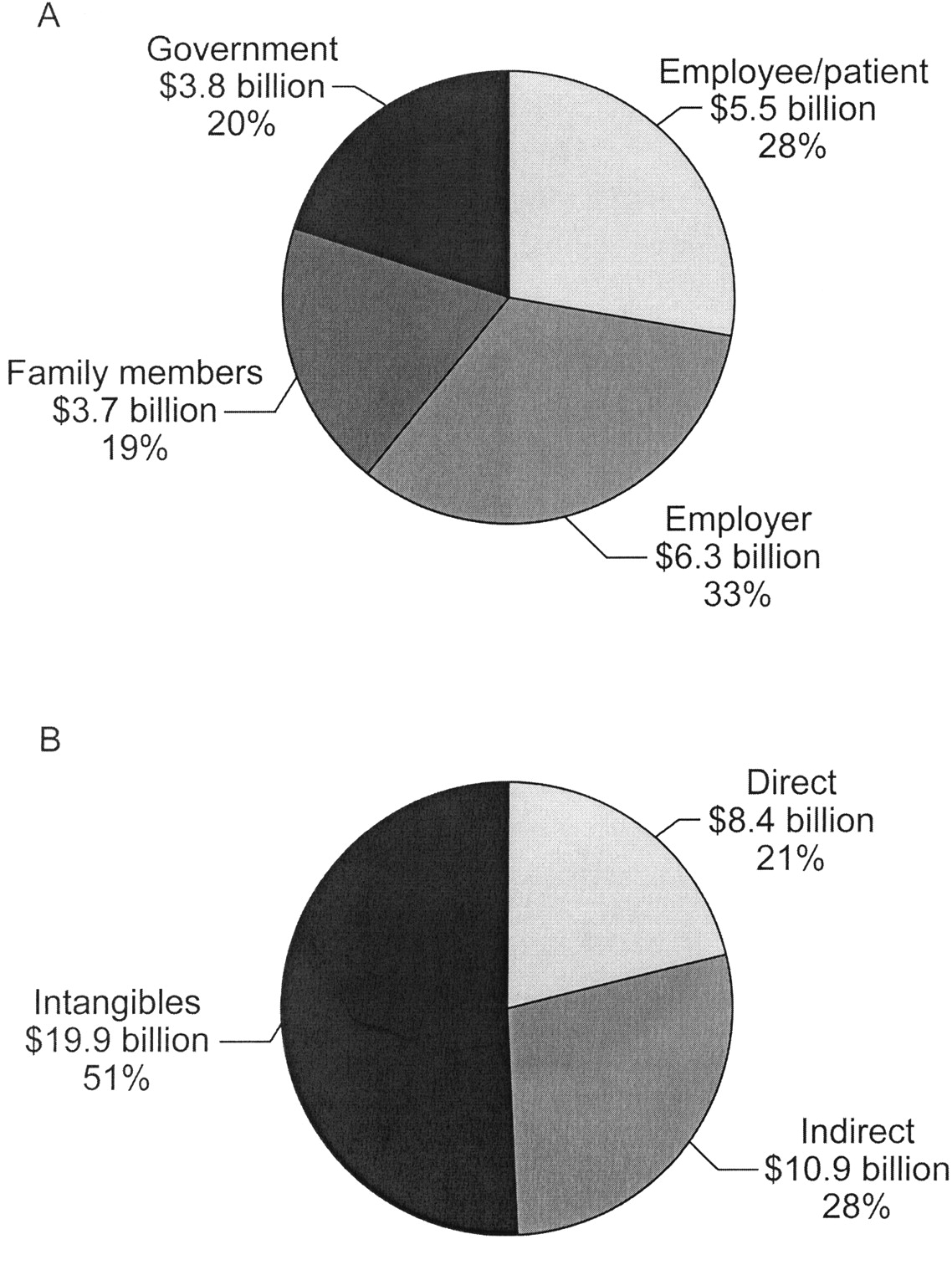
Costs associated with rheumatoid arthritis in the USA. A. Total annual societal costs by stakeholder (excluding intangible costs). Total: $19.3 billion. B. Total annual societal costs by direct, indirect, and intangible costs. Total: $39.2 billion. Reproduced with permission from Birnbaum H, et al. Curr Med Res Opin 2010;26:77–90. Copyright© 2010 Informa UK Ltd.
Kobelt, et al3 developed a model that determined the effect of function [measured with the Health Assessment Questionnaire (HAQ)], and disease activity [assessed on a global visual analog scale (VAS)] on costs and QOL in RA. The model took into consideration 5 functional states according to HAQ scores (< 0.6, 0.6 < 1.1, 1.1 < 1.6, 1.6 < 2.1, and ≥ 2.1). Each state was further subdivided according to VAS (< 40 and > 40 out of a maximum score of 100). The total costs significantly correlated with HAQ (Figure 3), except the costs associated with short- to medium-term work absence, which was correlated with VAS. Kobelt, et al24 also compared costs and consequences of RA in Sweden and the UK, and found indirect costs to be much higher in Sweden. The differences were predominantly due to the fact that far fewer patients remained in the workforce in Sweden compared to the UK.

Mean annual cost of rheumatoid arthritis in the United Kingdom in association with Health Assessment Questionnaire (HAQ) scores3.
Maetzel, et al6 compared the socioeconomic burden of 3 common disabling conditions — RA, osteoarthritis (OA), and hypertension — in Ontario, Canada. Study participants were recruited by 52 rheumatologists and 72 family physicians and were interviewed at baseline and at 3 months. Approximate estimated annual costs for RA (n = 253), mixed OA and hypertension (n = 191), OA (n = 140), and hypertension (n = 142) were $9300, $4900, $5700, and $3900, respectively. Thus, the study confirmed that the economic costs incurred by RA significantly exceed those related to OA, hypertension, and even to combined OA and hypertension. Further, indirect costs related to RA were up to 5 times higher than indirect costs associated with the other 2 conditions. Productive time spent doing housework and/or work-related duties was also lower among patients with RA compared to those with OA and hypertension. The presence of comorbidities had a strong association with disease costs. Similarly, Joyce, et al25 found total healthcare costs in patients with RA and comorbid depression and/or cardiovascular disease were significantly higher than those in patients with RA alone.
WORK STATUS AND WORK PRODUCTIVITY IN PATIENTS WITH ANKYLOSING SPONDYLITIS (AS)
Several studies reported the influence of AS on ability to work and the associated healthcare costs26,27,28. Compared to the general population, individuals with AS have lower employment rates, experience more disability, and are absent more frequently from work29,30,31. According to a US study, 13% of patients with a median disease duration of 21 years were on permanent work disability32, whereas a study in The Netherlands indicated that 31% of patients had left the workforce within 20 years after diagnosis33. Differences seen in the employment of AS patients reported by different countries are likely due to the variations in the social security systems and economic situations28,30. Total annual indirect costs associated with AS range from $5287 in the US to $8535 in Europe1. In Canada, the mean annual cost per patient is estimated at $9008 and lost work capacity accounts for 38% of these costs34. Further, both diminishing physical function and high disease activity were associated with a significant increase in costs (Figure 4). For Bath Ankylosing Spondylitis Functional Index (BASFI) scores < 5, the estimated cost increase per unit-increase was around $1000 and for BASFI scores > 7, the cost increase per unit-increase was over $5000.

Mean annual costs for patients with ankylosing spondylitis (AS) with different levels of Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Bath Ankylosing Spondylitis Functional Index (BASFI). Costs for different severity levels of AS are presented for hypothetical patients with a defined combination of BASFI and BASDAI (2,2; 5,5; 8,8). BASDAI and BASFI are both scored out of 10. Reproduced with permission from Kobelt G, et al. J Rheumatol 2006;33:289–95. Copyright© 2006, The Journal of Rheumatology Publishing Company Limited.
WORK LIMITATION AND PRODUCTIVITY LOSS IN PATIENTS WITH PSORIASIS
In 2004, the estimated indirect cost of psoriasis in the US due to lost productivity was reported in the range of $114 million per year35. Lost workdays, restricted activity days, and caregiver lost workdays accounted for $51 million, $32 million, and $22 million of this total, respectively. According to Schmitt and Ford16, the indirect costs associated with psoriasis are in fact much higher and considerably outweigh the direct costs of the disease. Among 201 individuals with psoriasis who answered the Work Limitation Questionnaire (WLQ), 16.3% were unemployed, 34% had missed at least 1 day of work, and 10% had missed ≥ 3 days of work within the past 4 weeks as a result of their psoriasis. The investigators calculated the total cost of health-related work productivity loss in patients with psoriasis to be about $16.6 billion, taking into consideration both absenteeism and presenteeism.
THE EFFECT OF ANTI-TNF-α THERAPY ON WORK PRODUCTIVITY
Over the past decade, a number of biologic therapies have been approved for the treatment of various IMID, including RA, AS, IBD, and psoriasis. In RA, biologics have been shown to be more effective than conventional disease-modifying antirheumatic drugs in controlling symptoms of the disease, improving disability, and slowing radiographic progression. It has also been suggested that early suppression of disease activity may be essential for maintenance of work capacity in patients with recent onset of RA36. Although the effects of anti-TNF agents on work outcomes have been evaluated in several studies, the effects of these agents on longterm work prospects in patients with RA remain unknown37. Yelin, et al7 demonstrated significant improvement in hours of work per week over a 12-month period in patients treated with etanercept compared to those not receiving the drug. After adjustment for demographics, overall health status, duration of RA, RA status, occupation, and industry, those treated with etanercept worked 7.4 more hours per week. More recently, Wolfe, et al8 identified 1986 employed patients receiving anti-TNF therapy and 1900 patients who were also employed but who were anti-TNF-naive. Work disability was assessed by patients self-reporting (SR disability) and by US Social Security disability reports (SS disability). In unadjusted analyses, patients treated with anti-TNF agents had an increased risk of both SR and SS disability. However, as the anti-TNF group included more sick patients with worse disease activity scores compared to those in the non-anti-TNF group, after adjustment for disease-related covariates, anti-TNF therapy was associated only with SR disability. Therefore, the investigators could not discern a positive effect of anti-TNF therapy on the risk of work disability.
In several studies, treatment of RA with adalimumab was associated with sustained ability to work38, reduction in job loss39, and improvement in work participation40; however, not all of the productivity-related results from these studies achieved statistical significance. A randomized, controlled trial by Smolen, et al41 found no significant difference in any indicator between patients with early RA treated with methotrexate (MTX) or MTX in combination with infliximab, but they observed significantly fewer lost workdays among patients in the combination therapy group. Two Scandinavian studies also produced conflicting results. Laas, et al42 found no substantial decrease in work disability costs 1 year after infliximab treatment. However, using data from the Stockholm anti-TNF-α followup registry, Augustsson, et al43 provided evidence that biologic therapy increases workplace participation in a group of patients typically expected to experience progressive deterioration and reduced ability to work. The investigators estimated an improvement of 4.2 hours/week during the first year followed by an added improvement of 0.5 hour/week annually thereafter.
Observational, population-based studies in IBD evaluating the influence of anti-TNF therapy on productivity and associated indirect costs are scarce. The ACCENT I and II trials included the differences in resource use in patients treated with infliximab as secondary endpoints44,45. In both studies, treatment with infliximab led to a significant reduction in the number of hospitalizations and surgeries 1 year after initiation of infliximab. This was especially pronounced in patients with fistulizing disease. In contrast to these randomized clinical trials, a population-based study using the University of Manitoba Inflammatory Bowel Disease Epidemiology Database found treatment with infliximab was associated with increases in IBD-related physician visits, hospitalizations, and surgeries compared to treatment with azathioprine9. It should be noted that infliximab patients were significantly younger at diagnosis and first treatment, had a longer disease duration at first diagnosis, and underwent more resective surgery before and after diagnosis. The importance of this study is that, contrary to well controlled trials, it included and assessed all comers during a longer timeframe (3 years after initiation of infliximab), which might be more relevant to real-world clinical practice. These results indicate the importance of longer time horizons; they also serve as a reminder that direct as well as indirect costs are needed for a complete cost-effectiveness analysis.
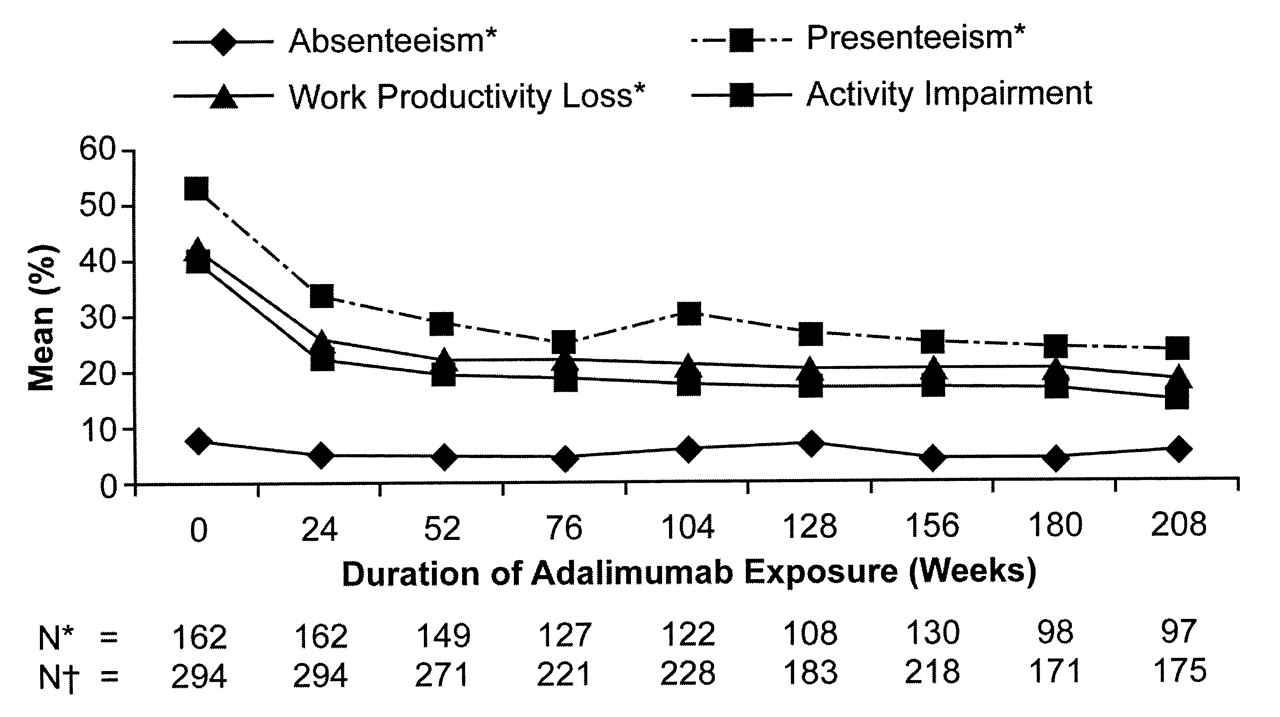
In patients with AS, longterm anti-TNF-α therapy was associated with sustained improvement in the Work Productivity and Activity Impairment-Specific Health Problem Questionnaire (Figure 5)46. In the Evaluation of Infliximab for Psoriasis in a [Remicade] Efficacy and Safety Study (EXPRESS II), infliximab-treated patients demonstrated a statistically significant productivity increase on a 10-cm productivity VAS: 2.7 cm from baseline compared with a mean decrease of 0.1 cm achieved with placebo (p < 0.001) through 10 weeks and sustained at Week 2447. Similarly, in a study of 1230 patients with psoriasis treated with 45 mg or 90 mg of ustekinumab, the self-administered WLQ and VAS showed work productivity improved and sick days reduced48. At Week 12, the productivity VAS scores improved by 72.6% and 71.4% in the 45 mg and 90 mg ustekinumab groups, respectively, but were unchanged in the placebo group (p < 0.001). Only 2.0% of each ustekinumab group missed days from work compared to 8.3% taking placebo (p < 0.001). In the WLQ domains, there was greater improvement in time management with usteki numab 45 mg/90 mg versus placebo (6.6/9.1 vs −0.7), mental-interpersonal (7.8/7.5 vs −1.1), and output demands (6.8/7.0 vs −1.1) (p < 0.001) at Week 12, which were maintained through Week 24.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Longterm effects of adalimumab on work-related outcomes in patients with ankylosing spondylitis. *Only employed patients were considered for the first 3 items of the WPAI-SHP (absenteeism, presenteeism, and work productivity loss). †All patients, including unemployed patients, were considered for the fourth item of the WPAI-SHP (activity impairment). WPAI-SHP: Work Productivity and Activity Impairment-Specific Health Problem Questionnaire. Reproduced with permission from Maksymowych WP, et al. J Rheumatol 2010;37:385–92. Copyright© 2010, The Journal of Rheumatology Publishing Company Limited.
CONCLUSION
Socioeconomic outcomes, including work productivity, are an important piece of the puzzle when conducting economic evaluations. Evidence with regard to their scope and magnitude should be included in economic assessments, along with direct costs and health outcomes. Adverse effects of IMID in regard to socioeconomic burden and work productivity have been well documented and quantified. The emergence of biologic therapies, anti-TNF-α agents in particular, have revolutionized treatment of these disabling diseases and made long-lasting remission highly achievable. From the presented evidence it is apparent that productivity-related outcomes increasingly are being assessed in clinical trials. However, it is still uncertain whether and to what extent anti-TNF agents affect work-related productivity and the associated indirect costs.
Footnotes
-
Supported by an unrestricted grant from Abbott Canada. Dr. Jacobs has received a research grant for Economics of Uveitis from Abbott; Dr. Bissonnette received research grants or honoraria from Abbott, Amgen, Astellas, Merck, Pfizer, and Schering; Dr. Guenther has acted as consultant for Abbott Laboratories, Amgen Canada, Galderma Canada, LEO Pharma, Janssen, Schering-Plough Canada, and Wyeth; and received investigator-initiated study support from Astellas Pharma Canada; and contract research support from Abbott Laboratories, Amgen Canada, Astellas Pharma Canada, Celgene Corporation, Centocor Ortho Biotech, EMD Serono Canada, Galderma Canada, Isotechnika, Janssen-Ortho, LEO Pharma, Novartis Pharmaceuticals Canada, Pfizer, Schering-Plough Canada, and Stiefel Laboratories.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.