
Abstract
Clinical trials evaluating therapies for the management of rheumatoid arthritis (RA) typically report disease activity using measures such as the American College of Rheumatology response criteria and Disease Activity Scores. Additional outcomes, such as feeling well and feeling less fatigue, appear to be more important to patients than traditional disease activity outcomes such as joint tenderness and stiffness. As a result, patient-driven outcomes are increasingly used in clinical trials of RA, and have been shown to provide useful information. It is proposed that factors such as Health Assessment Questionnaire scores, fatigue, sleep, and physical and mental function become part of a patient’s core set of outcomes when assessing patients with RA.
- RHEUMATOID ARTHRITIS
- PATIENT-DRIVEN OUTCOMES
- FATIGUE
Despite significant improvements in therapy in recent years, quality of life (QOL) for patients with rheumatoid arthritis (RA) is still well below that of the general population. QOL includes not only quality of function, but QOL in all its facets. RA, particularly when poorly controlled, disrupts the quality of a person’s life by adversely affecting their ability to maintain their “normal” life and identity. “Feeling well” is described by patients as an important aspect of QOL. Constantly feeling ill or being in pain takes its toll on a person’s natural resilience and motivation. Patients with RA not only have to live with the pain and decreased physical functioning associated with joint damage, fatigue, and disturbed sleep, but also often have to come to terms with issues such as economically altered (often greatly reduced) lifestyles and a lack of control over their lives, activity participation, and healthcare. Not surprisingly, this influences the patient’s emotional well-being and QOL. Some patients may face additional QOL challenges, such as social isolation and/or discrimination, especially if they have noticeable joint damage. Patient-driven outcomes are increasingly being used to assess the efficacy of RA therapies in clinical trials.
PATIENT-DRIVEN OUTCOMES IN CLINICAL TRIALS
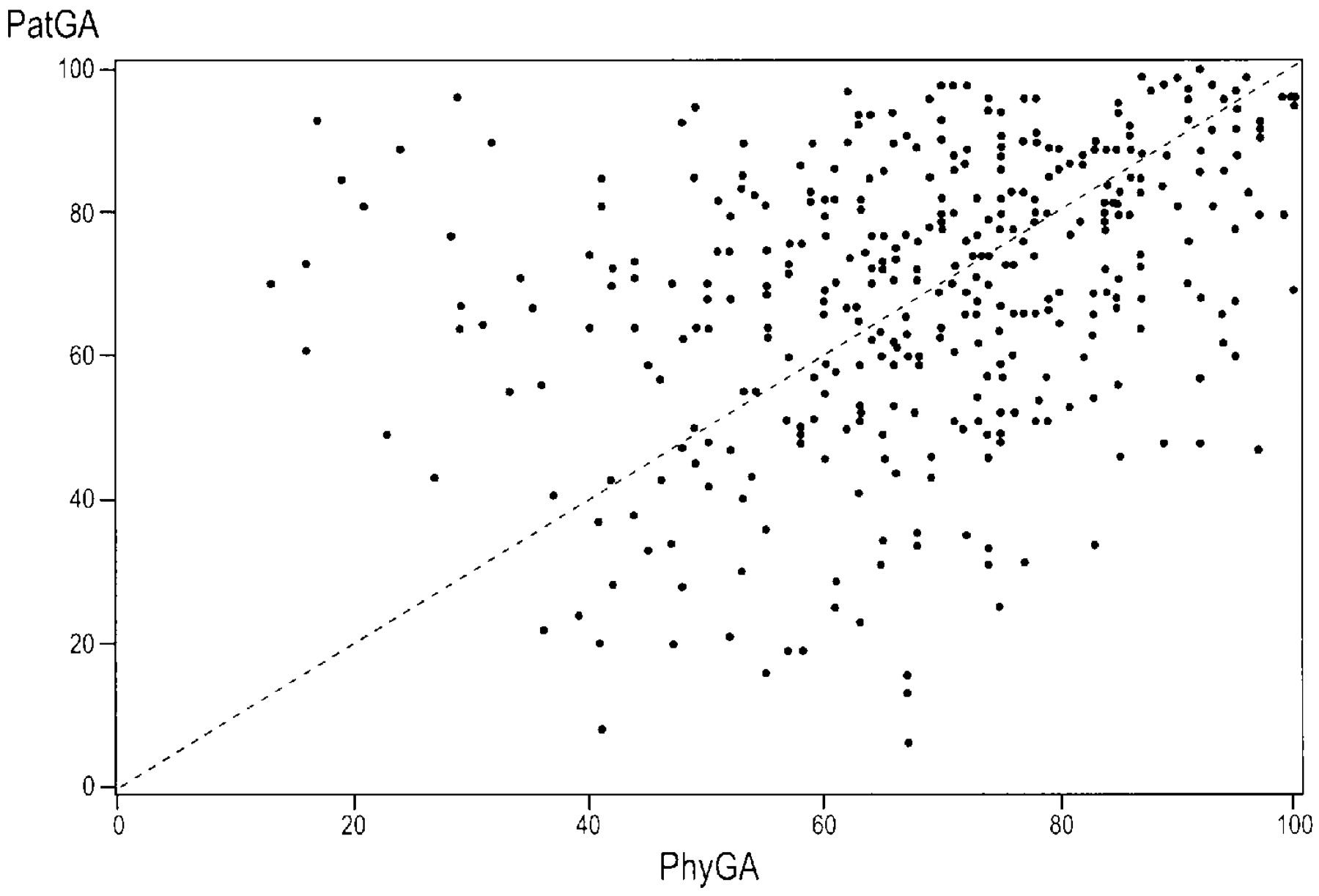
The Abatacept Trial in Treatment on Anti-TNF Inadequate Responders (ATTAIN)1 assessed the efficacy and safety of the selective costimulator modulator abatacept in patients with active RA who had an inadequate response to anti-tumor necrosis factor (TNF) therapy and were receiving background therapy with a disease modifying antirheumatic drug (DMARD). In addition to typical measures such as a 20% improvement in American College of Rheumatology RA criteria (ACR20)2, responses to the Health Assessment Questionnaire (HAQ), and C-reactive protein (CRP) levels, clinical efficacy was measured by both the patient and the physician global assessments of disease activity. When results from the patient and physician global assessments are visualized on a scatterplot (Figure 1) or a Bland-Altman plot, not surprisingly, the data do not demonstrate uniform agreement, suggesting that physician and patient assessments of outcomes are not always well correlated (unpublished data). What factors contribute to this discrepancy? Looking at the absolute standardized coefficients of outcomes in the ATTAIN trial1, it was evident that tender joint count, swollen joint count, and CRP had greater contributions to the physician global assessment than to the patient global assessment. Variables with a greater contribution to the patient global assessment included pain, HAQ scores, fatigue, sleep, and physical and mental components of the Medical Outcome Study Short-Form General Health Survey (SF-36). To confirm these findings, it would be worthwhile to replicate these results with clinical data, as opposed to clinical trial data, using traditional as well as newer patient core outcomes. Disease duration, and the relation between tender joints and pain, should also be examined to determine the effects of these variables on patient-reported outcomes.

Scatterplot of physician (PhyGA) vs patient global assessment (PatGA) scores in the Abatacept Trial in Treatment on Anti-TNF Inadequate Responders (ATTAIN)1.
Patient-driven outcomes have also been used to assess the efficacy of other biologics in the treatment of RA. In a study of rituximab, patients with severe RA who were refractory to anti-TNF therapy experienced significant improvements in patient-reported pain, fatigue, functional disability, health-related QOL, and disease activity3. In the multicenter, open-label, single-arm OMEGA (Outcome Measures Generated by Anakinra) trial, HAQ scores were assessed and found to be significantly improved among patients given anakinra in addition to their existing DMARD treatment4. Fatigue has also been used as an outcome measure in 3 randomized, placebo-controlled trials of adalimumab, where treatment with the anti-TNF agent in combination with methotrexate or standard therapy was shown to significantly reduce fatigue in patients with moderate to severe RA5.
A systematic review of the literature was recently conducted to assess the frequency of use of various patient-reported outcomes used in clinical trials of RA6. Of 109 clinical reports, 50 were randomized, controlled trials (RCT) and 59 nonrandomized studies (NRS). Patient-reported outcomes in the 109 trials included function, patient overall assessment, morning stiffness, QOL, utility, fatigue, self-reported painful joint count, psychological status, coping, productivity losses, well-being, sleep disturbance, and leisure. These outcomes were then ranked according to the frequency of their use in clinical trials. Overall, “function” was the most common patient-reported outcome, used in 90% of RCT and 78% of NRS (Table 1). Of interest, only 4% of RCT used fatigue as an outcome measure, while 22% of NRS used this outcome measure, making it the fifth most commonly used outcome, ahead of QOL and utility, among NRS.
Domains and tools used to assess patient-related outcomes in randomized clinical trials (RCT) and other clinical reports of rheumatoid arthritis6. Reprinted from Ann Rheum Dis 2009;68:183–90, with permission.
Which of these domains are most important to patients? A series of focus groups conducted in the United Kingdom7 generated a list of 23 outcomes that patients deemed important in relation to the treatment of their RA (Table 2). To assess the relative importance of these outcomes and validate their generalizability to a wider RA population, a questionnaire was distributed to 3 rheumatology centers in the United Kingdom8. Patients were asked to rank each outcome according to its importance. The most frequently selected outcomes were independence, pain, and mobility (Figure 2). Through factor analysis, 6 distinct groupings were identified: general well-being (11.9% explained variance), day-to-day functioning (10.6%), emotional and psychological well-being (10.6%), social role and confidence (10%), physical symptoms (9.5%), and medication issues (7.9%). When the top 10 outcomes were grouped according to these 6 categories, general well-being, day-to-day functioning, and physical symptoms were revealed as having the greatest importance for patients. These results suggest that pain and function domains reflect disease activity and patient priorities, supporting their use as core outcome measures. Additional outcomes, such as feeling well and feeling less fatigue, appear to be more important to patients than traditional disease activity outcomes, such as joint swelling and stiffness.
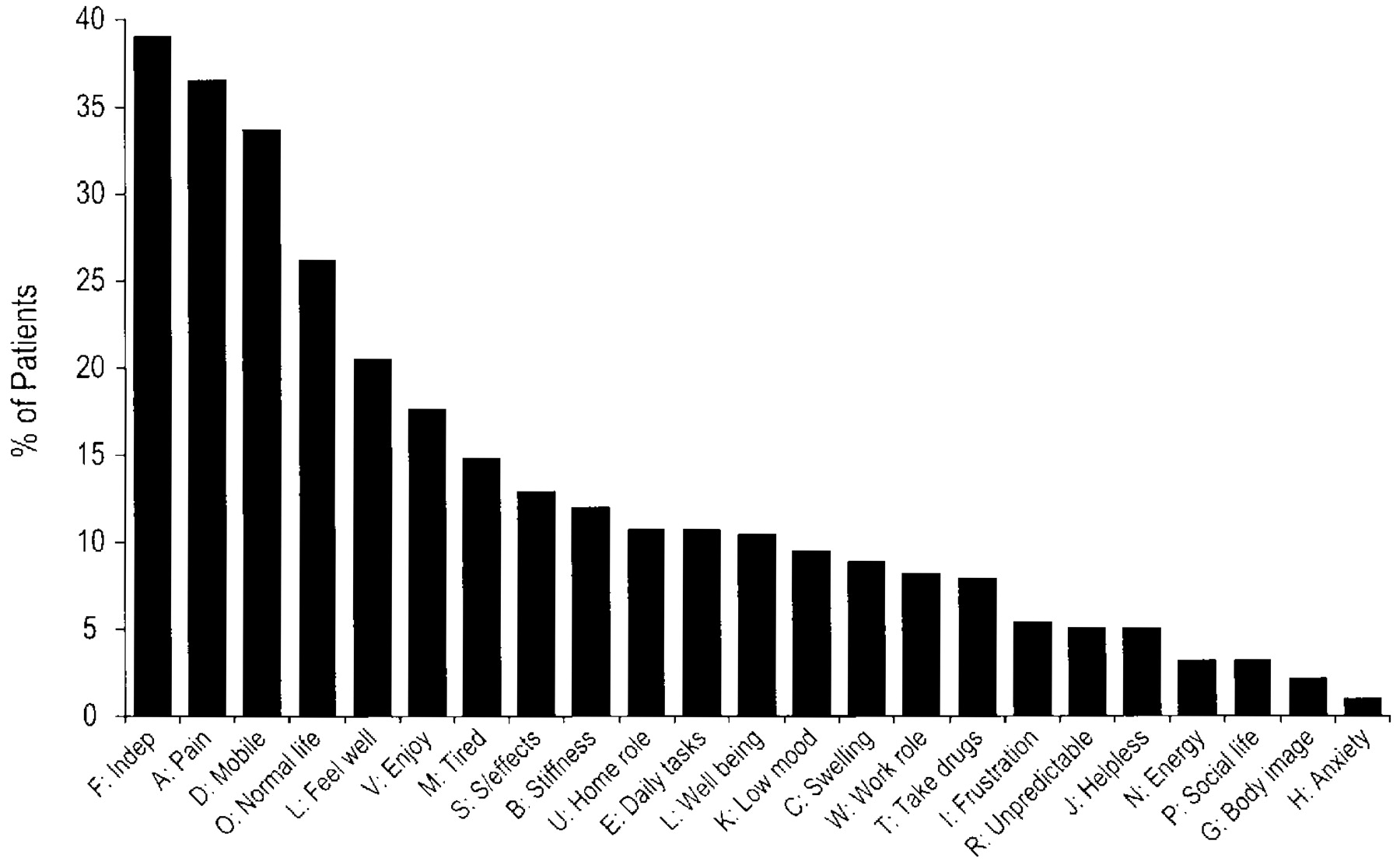
Proportion of patients who selected each outcome as their 3 most important, in a survey of 323 patients from 3 rheumatology centers in the United Kingdom8. Reprinted from Musculoskeletal Care 2005;3:131–142, with permission.
Outcomes identified as important by patients with rheumatoid arthritis in a series of focus groups7.
Numerous clinical studies have identified fatigue as an important patient-related outcome in RA9–14. However, lengthy questionnaires designed to assess levels of fatigue are not always practical for clinical care. Wolfe13 compared answers to a single-item visual analog scale (VAS) with answers to 3 longer fatigue questionnaires completed by 7,760 participants in a longitudinal outcome study of RA. With respect to clinical variables and sensitivity to change, the single-item VAS performed as well as, or better than, longer scales such as the Multi-dimensional Assessment of Fatigue (MAF)15, the vitality scale from the SF-36, and the Brief Fatigue Inventory16. The VAS fatigue scale is considered therefore suitable for routine use in clinical care. Its minimal clinically important difference (MCID) is 10 on the 100 mm VAS17.
Sleep has also been shown to be an important patient-reported outcome in clinical trials18–20. In studies of abatacept, sleep was assessed using the Medical Outcomes Study Sleep measure21, resulting in an MCID of 6 for the subscale sleep problems index II17. Anecdotal evidence suggests that sleep disturbance is among the most important aspects of sleep.
Work productivity has also been used as a patient-reported outcome in clinical trials of RA. However, a limitation of this measure is its applicability only to patients who are employed. An alternative activity measure has been developed for recent clinical trials, which assesses how many days a patient is limited in terms of being able to do what they would have liked to do. The Activity Participation Questionnaire (ApaQ) consists of 2 items: During the past 30 days, how many days did your RA keep you from doing your usual activities?, and, How often were you able to perform your usual activities completely? The benefit of such a tool is its applicability to everyone in terms of what they considered to be their usual activities, from the most sedentary patient to the most active. This activity measure has been validated22. Patients treated with abatacept in the Abatacept in Inadequate Responders to MTX trial (AIM)23 were able to participate in daily activities on 24.7 days per month after one year of treatment, representing an increase of 8.3 days from baseline, compared to an increase of 4.4 days in the placebo group (p < 0.001). Similarly, improvements were experienced in the Abatacept Trial in Treatment of Anti-TNF INadequate responders trial (ATTAIN)24 with a gain of 7.4 days, respectively (1.4 days for placebo), resulting in 20.1 days of activity participation per month after 6 months of treatment.
Patient-reported measures are being integrated into clinical trials in several ways. The European Rheumatoid Arthritis Impact of Disease (RAID) group assessed numerous different measures of patient-reported outcomes25, and came up with 7 domains deemed to be most important to patients: pain, function, fatigue, emotional well-being, sleep, coping/helplessness, and physical well-being. This score may be of value in clinical trials as a new composite index to identify information that is relevant for patients. The joint European League Against Rheumatism/ACR task force has recommended that clinical trials of RA report on fatigue as a measure of disease activity26. The task force is also currently redefining their criteria for remission in patients with RA, and fatigue is currently under consideration as an outcome. OMERACT is also looking at including patient-reported outcomes in their consideration of outcome measures in patients with RA9,10.
WHAT PROPORTION OF PATIENTS ATTAIN QOL OUTCOMES?
In the systematic review by Kalyoncu, et al, the most commonly used instrument was the SF-36 – a generic QOL instrument that can be applied to a wide range of patients (e.g., cardiac, diabetic, and arthritic patients)6. The 8 domains of the SF-36 are physical, role limitation due to physical problems, bodily pain, general health, vitality, social functioning, role limitation due to emotional problems, and mental health. These 8 domains are then combined into 2 component scores – the physical component score and the mental component score – which are assessed on a scale of 0 to 100, where 100 indicates a better QOL. An improvement of 3 or more units is considered to be clinically meaningful. In both the ATTAIN24 and AIM23 trials, patients treated with abatacept experienced clinically meaningful and statistically significant improvements in all 8 subscales of the SF-36, as well as the physical and mental component scores. The greatest improvement in health-related QOL was observed in bodily pain. However, compared to “norm values” based on the US population, one finds that few of the patients in the RA population achieve the norm values. It is probably unreasonable to use the normal population as a comparator when looking to measure improvements in QOL among the RA population. In order to determine the true proportion of patients with RA who regain their QOL, further research is needed to establish this benchmark.
The performance of the SF-36 in 7 randomized, double-blind trials of various therapies for RA was recently assessed by Tugwell, et al27. Mean standardized response rates were calculated for the various patient-reported outcomes in the 7 trials. For the physical component of the SF-36, a small to moderate effect size was revealed for rituximab, a moderate effect size for abatacept and celecoxib, and variable effect sizes for infliximab. As expected, the mental component of the SF-36 was less responsive to change, with only the rituximab and abatacept trials showing a significant effect size. The authors concluded that the SF-36 correlated well with HAQ results, as well as physician and patient global assessments.
WHAT IS THE ACCEPTABLE SYMPTOMATIC STATE?
The Patient Acceptable Symptomatic State (PASS) is the highest level of symptoms beyond which patients consider themselves well. The goal is to determine the PASS using patient-driven outcomes when assessing patients with RA29. Differences between PASS, low disease activity state (LDAS), and MCID were reviewed by Tubach, et al29. From the patients’ perspective, it appears that LDAS and PASS are different. While LDAS addresses a symptomatic state above which a therapeutic decision should be taken, PASS addresses a relevant and desirable symptomatic state.
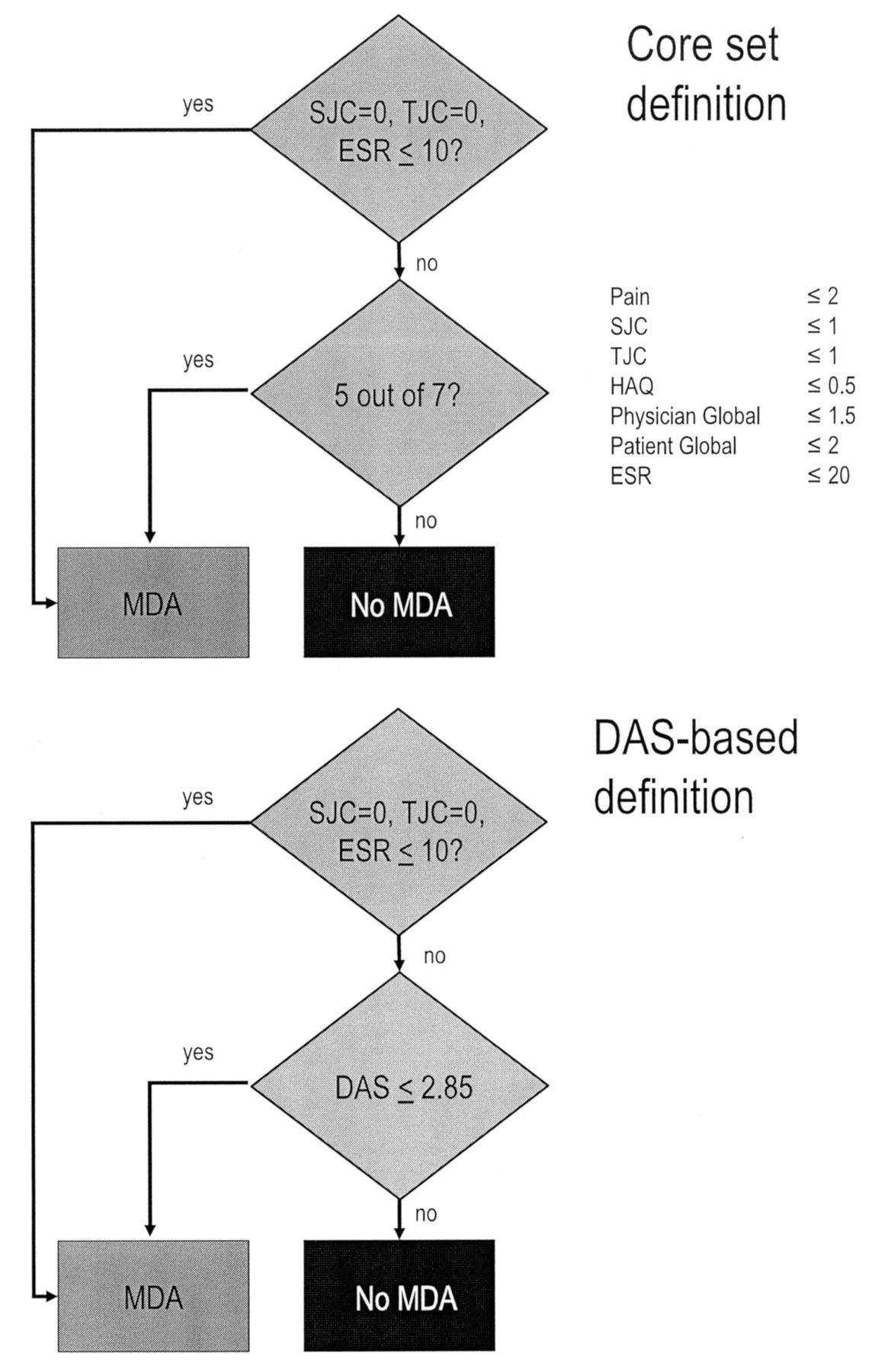
An algorithm for determining LDAS in RA has been developed based on existing algorithms. The minimal disease activity (MDA), which is based either on meeting 5 of the 7 World Health Organization(WHO)/International League of Associations for Rheumatology (ILAR) core set measures or on DAS30 (Figure 3). For a patient acceptable state outcomes can either be combined into one cutoff score, as in the DAS definition of MDA, or patients are required to satisfy cutoff values for a specified number of outcomes.
{kind=link}
{kind=link}
{kind=link}
Algorithms for determining minimal disease activity, based on core set measures (top) or Disease Activity Scores (DAS) (bottom)29. Reprinted from J Rheumatol 2005;32:2016–24, with permission.
CONCLUSIONS
Despite significant improvements in therapy for patients with RA, QOL remains below that of the general population. Pain and function domains reflect disease activity and patient priorities, supporting their use as core outcome measures. Additional outcomes, such as feeling well and feeling less fatigue, appear to be more important to patients than traditional disease activity outcomes, such as joint tenderness and stiffness. Factors such as HAQ scores, fatigue, sleep, and physical and mental function, therefore, should become part of a patient’s core set of outcomes when assessing patients with RA.
Footnotes
-
Supported by an unrestricted educational grant from Bristol-Myers Squibb Canada.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.