
Abstract
Objective To describe psoriatic arthritis (PsA) flares and their effect on patient-reported outcomes (PROs).
Methods Cross-sectional surveys of rheumatologists/dermatologists and their patients with PsA were conducted in France, Germany, Italy, Spain, the United Kingdom, and the United States, capturing data on physician-reported patient flare status, demographics, PsA severity, and clinical outcomes. Patient-completed surveys captured data on PROs: 5-level EuroQol 5-dimension, Work Productivity and Activity Impairment questionnaire, Health Assessment Questionnaire–Disability Index, and 12-item Psoriatic Arthritis Impact of Disease questionnaire. Patients were compared by flare status using parametric and nonparametric tests. Multivariate regression was used to identify flare associations. Multivariate logistic regression adjusted for patient demographics and physician specialty assessed the effect of flare status.
Results Among 2238 patients (586 from the US, 1652 from Europe) managed by 572 physicians, physician-reported flare was present for 168 patients (7.5%), and self-reported flare was present for 95 patients (10% of available data). Mean (SD) flare count over 12 months was 2.2 (4.9), lasting on average 16.4 (16.2) days. Flare status was linked to worse PROs. Patients who had not flared in the last 12 months or had never flared had a higher quality of life, lower overall work impairment, and a lower degree of disability compared with patients who were currently experiencing a flare (all; P < 0.01).
Conclusion Actively experiencing a flare adversely affected QOL, disability, and work productivity. PsA flares should be routinely assessed and managed in clinical care.
- Health Assessment Questionnaire
- psoriatic arthritis
- quality of life
Psoriatic arthritis (PsA) is an immune-mediated rheumatologic disease that is distinct from rheumatoid arthritis and associated with psoriasis (PsO). PsA is recognized as a severe progressive disease that can result in joint remodeling and damage leading to disability, and reduced quality of life (QOL) and work productivity.1-3 The overall effect of PsA is broad, covering all aspects of patients’ lives, including activities and participation, physical and emotional aspects, and domains such as fatigue, coping, or sleep disturbance.4
PsA is a long-term condition with variable disease activity and acute worsening conceptualized as flares, which can affect the skin, joints, or both, and periods of remission.5 Remission or low disease activity is the treatment goal, since sustained low disease activity has been shown to be effective in reducing the radiographic progression of PsA.6 In current clinical practice, while a flare may be represented as a measure of swollen joint count (SJC) or tender joint count (TJC), the psychosocial effects of the disease, such as social withdrawal, psychological symptoms, fatigue, and loss of function, are also important factors to consider in patients’ disease management.7 These features can result in a significant loss of function and social interaction, which affects the patients’ everyday life more than a painful or swollen joint or an area of skin lesions alone.5 High levels of disease activity are associated with work disability; however, limited data exist with respect to flaring and work impairment.8
The objectives were to describe the frequency, duration, and type of flares experienced by patients with PsA, and to assess the effect of flares on patients’ QOL and work productivity as well as factors associated with flares.
METHODS
Study design and participants. Data were drawn from the Adelphi PsA Disease Specific Programme, a cross-sectional survey of physicians (dermatologists and rheumatologists) and their adult patients with PsA, conducted between June and August 2018 in France, Germany, Italy, Spain, the United Kingdom, and the United States. A detailed description of the methods of data collection has been previously published and validated.9
To take part in the survey, physicians had to be involved in patients’ treatment decisions for a minimum of 5 patients with PsA per calendar month. Physicians were required to provide data for the next 3 to 6 consecutive patients with PsA who visited for routine care. There were no restrictions according to treatments or clinical features such as disease activity, disease severity, or demographics. To be eligible, patients had to have a physician-confirmed diagnosis of PsA and provide their informed consent.
Definition of flares. Physicians reported patients’ flare status, categorizing them as either “currently in flare,” “not currently flaring, but flared in last 12 months,” “not flared in last 12 months,” or “never flared.” For the purposes of this analysis, “not flared within the last 12 months” and “never flared” were grouped together. Physicians provided information on the number and typical length of patients’ flares (days) in the last 12 months, which component of the patient’s PsA (skin, joints, or both) was currently flaring, and whether they categorized the flare as mild, moderate, or severe.
Patients reported their own flare status by selecting “Yes, I am currently experiencing a flare,” “Yes, but I am not currently experiencing a flare,” or “No, I do not flare,” in answer to the question “Do you ever experience ‘flares’ (temporary worsening) of your PsA?” They also reported which component of their PsA (skin, joints, or both) was currently flaring, and their subjective assessment of whether the flare was mild, moderate, or severe.
Other data collected. Physicians recorded disease duration and symptom duration of PsA, as well as disease status (improving, stable, or deteriorating) and severity (mild, moderate, or severe), which was determined by their own subjective rating based on patient medical records and their consultation. Physicians also reported the results of any physical examinations conducted, which could include TJC and SJC (out of 68 and 66 joints, respectively), body surface area (BSA) affected by PsO, and satisfaction with treatment outcome.
In addition, patients provided the following patient-reported outcomes (PROs): the 5-level EuroQol 5-dimension (EQ-5D-5L), converted into a single utility value, using a mapping approach from the EQ-5D-5L to EQ-5D-3L, ranging from 0 to 1, with lower scores indicating a worse outcome; the EQ-5D-5L visual analog scale (VAS), ranging from 0 to 100, with lower scores indicating a worse outcome10; Work Productivity and Activity Impairment (WPAI) questionnaire, ranging from 0 to 100, with higher scores indicating a worse outcome across all domains11; Health Assessment Questionnaire–Disability Index (HAQ-DI), ranging from 0 to 3, with higher scores indicating a worse outcome12; and the Psoriatic Arthritis Impact of Disease 12-item questionnaire (PsAID-12) ranging from 0 to 10, with higher scores indicating a worse outcome.13 Pain was measured using an unvalidated 10-point VAS scale, with higher scores indicating greater pain; treatment satisfaction was measured using a Likert-type 5-point scale, with possible answers for both physicians and patients being “very satisfied,” “satisfied,” “neither satisfied nor dissatisfied,” “dissatisfied,” and “very dissatisfied.”
Data analysis. Descriptive statistics were performed. Patients were compared by physician-reported flare status and by patient-reported flare status, using parametric or nonparametric tests as appropriate. To assess physician-patient agreement in identifying current flares and flare severity, physician- and patient-reported flare status were compared using the  statistic. Agreement was assessed for physician and patient perceptions if the patient was currently in flare or not. The
statistic. Agreement was assessed for physician and patient perceptions if the patient was currently in flare or not. The  statistic was interpreted as follows: a value of < 0.20 was considered slight agreement, 0.21 to 0.40 fair agreement, 0.41 to 0.60 moderate agreement, 0.61 to 0.80 substantial agreement, and 0.81 to 1.00 excellent agreement.14,15 Multivariate regression analysis was used to identify demographic and clinical factors associated with a higher risk of flaring. Logistic regression models were used to study the effect of flaring status on each of the PROs. Marginal means were used to predict the effect of flare status on PRO scores, keeping all other variables constant in the model. Models accounted for intragroup correlation across physicians and were adjusted for sex, age, time since diagnosis, employment status, BMI, and number of joints and percentage of BSA affected.
statistic was interpreted as follows: a value of < 0.20 was considered slight agreement, 0.21 to 0.40 fair agreement, 0.41 to 0.60 moderate agreement, 0.61 to 0.80 substantial agreement, and 0.81 to 1.00 excellent agreement.14,15 Multivariate regression analysis was used to identify demographic and clinical factors associated with a higher risk of flaring. Logistic regression models were used to study the effect of flaring status on each of the PROs. Marginal means were used to predict the effect of flare status on PRO scores, keeping all other variables constant in the model. Models accounted for intragroup correlation across physicians and were adjusted for sex, age, time since diagnosis, employment status, BMI, and number of joints and percentage of BSA affected.
P < 0.05 was considered statistically significant. All analyses used Stata Statistical Software (Release 15; StataCorp).16
Ethical considerations. The Adelphi PsA IV Disease Specific Programme complied with all relevant market research guidelines and legal obligations according to the European Pharmaceutical Marketing Research Association.17 No identifiable protected health information was extracted during the course of the study. Data were collected in such a way that patients and physicians could not be identified directly; all data were aggregated and deidentified before receipt. Both physicians and patients provided informed consent.
This research obtained ethics approval from the Western institutional review board (study number 1183030) in the US, and Freiberg ethics committee in Europe (study number 02018/1077). Each survey was performed in full accordance with relevant legislation at the time of data collection, including the US Health Insurance Portability and Accountability Act 199618 and Health Information Technology for Economic and Clinical Health Act legislation.19
RESULTS
Patient demographic, clinical, and treatment characteristics. Data were collected from 382 rheumatologists and 190 dermatologists for a total of 2270 patients with PsA (1675 in Europe and 595 in the US). Patients were 53.8% male, with a mean age (SD) of 48.7 (13.2) years. Physician-subjective disease severity assessment reported 75% of patients with mild PsA, 22.4% with moderate PsA, and 2.6% with severe PsA (Table 1). Patients with tender joints, swollen joints, and psoriatic skin lesions accounted for 47%, 24.4%, and 48% of patients, respectively, at the time of data collection.. In a subset of patients for which data were available, the mean (SD) SJC66 score was 3.3 (6.9) and the mean TJC68 score was 4.2 (6.6) for n = 514 and n = 493, respectively (Table 2). At the time of data collection, 54.9% of patients were prescribed a biologic disease-modifying antirheumatic drug (bDMARD), and 11% a targeted synthetic DMARD (Table 3). Physician-reported flare status was available for 2238 patients, and patient-reported flare status was available for 947 patients, with demographic characteristics similar in these subpopulations.
PsA patient demographic and clinical characteristics according to physician-reported patient flare status.
Unadjusted analyses showing patient PsA symptoms according to physician-reported patient flare status.
Unadjusted analyses showing patient current treatment for PsA according to physician-reported patient flare status.
Physician-reported flare status. Physician-reported flare status was available for 2238 of patients. Of these, physicians reported that 168 (7.5%) patients were currently flaring, 492 (22%) flared in the last 12 months, and 1578 (70.5%) had not flared in the last 12 months or never flared. The mean (SD) number of flares in the last 12 months was 2.2 (4.9), lasting an average of 16.4 (16.2) days. A total of 45.8% of patients experienced joint flare only; 48.8% experienced concomitant joint and skin flare and 5.4% experienced an isolated skin flare. A total of 18.3%, 64%, and 17.7% of patients were classified by their physician as experiencing a mild, moderate, and severe flare, respectively.
Demographic and disease characteristics of patients stratified by their flare status are shown in Table 1. We did not observe significant differences in demographics between the groups, except patients who were currently in flare were less frequently in full-time employment (P < 0.001). Of the 7.5% of patients that physicians reported as currently in flare, 19% had severe PsA, 60.1% had moderate PsA, and 20.8% had mild PsA.
In the unadjusted analyses, the mean percentage of BSA affected by PsO was significantly greater in patients with current flares (10.3 [SD 12.0]) than in those who were not currently flaring but had in the last 12 months (6.5 [7.6]) and those who had never flared (5.0 [7.7]). Tender joints, swollen joints, dactylitis, enthesitis, tendonitis, inflammatory back pain, and sacroiliitis were also found to be more commonly present in patients who were reported by physicians to be currently flaring compared to those who were not currently flaring but had flared in the last 12 months and those who had never flared (Table 2).
Patients with current flares were less commonly prescribed bDMARDs (42.9%) compared to those who were not currently flaring but had flared in the last 12 months (58.3%) and those who had never flared (55.1%; Table 3).
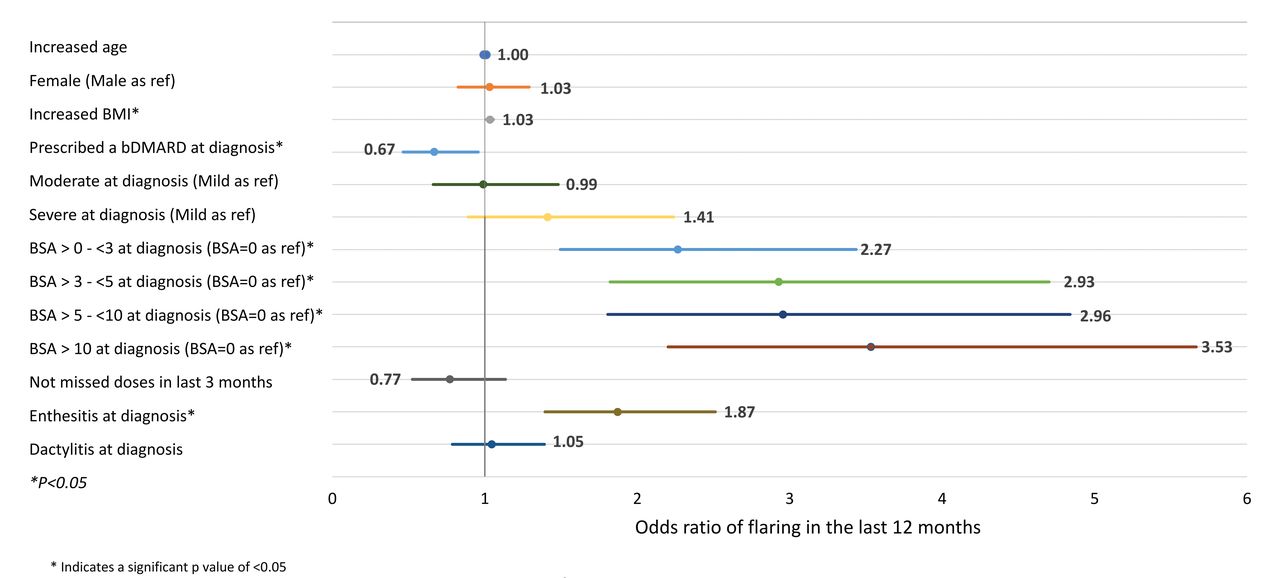
In regression analyses to assess associations of patient characteristics and status with a flare in the last 12 months, we found that a lack of bDMARD prescription at diagnosis (odds ratio [OR] 0.67), enthesitis at diagnosis (OR 1.87), and any skin involvement at diagnosis (OR 2.27-3.53 by extent of skin involvement) were associated with flaring currently or flaring within the last 12 months, with a proportionally higher risk of flare with greater levels of BSA involvement (Figure 1). Unadjusted analyses showing the association between physician-reported flaring status and PRO measures are shown in Supplementary Table S1 (available with the online version of this article).
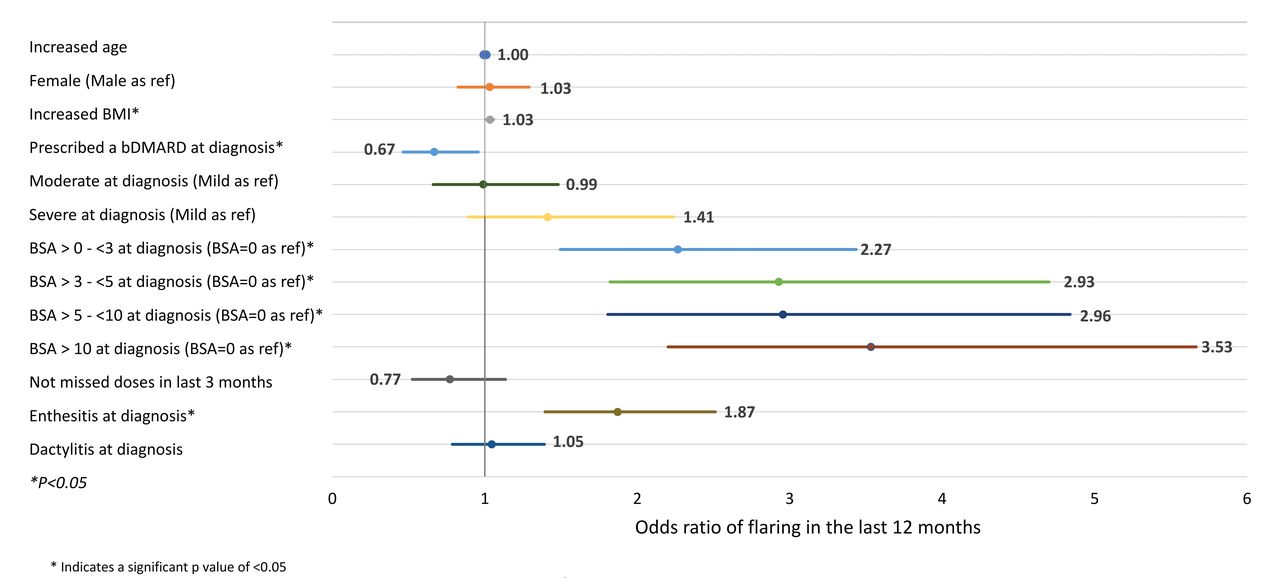
Multivariate regression assessing predictors of flaring in past 12 months (physician-reported flare status). bDMARD: biologic disease-modifying antirheumatic drug; BSA: body surface area; ref: reference.
Patient-reported flare status. Of the 947 patients with PsA who reported their flare status, 95 (10%) reported they were currently flaring, 376 (39.7%) had experienced flare but not currently, and 476 (50.3%) had never flared. Patients currently experiencing a flare had a higher mean age, a higher BMI, and were less likely to be working full time than patients who reported they had flared previously but were not currently flaring and those who had never flared (P < 0.05; Supplementary Table S2, available with the online version of this article).
Among patients who were currently flaring, 7.6% reported that their flare was mild, 60.9% reported a moderate flare, and 31.5% reported a severe flare. The types of flares patients experienced varied, with a total of 38.8% experiencing isolated joint flare, 52.9% experiencing concomitant joint and skin flare, and 8.2% experiencing an isolated skin flare.
Of the 10% of patients currently in flare, 40% had mild disease, 50.5% had moderate disease, and 9.5% had severe disease (Supplementary Table S2, available with the online version of this article). Characteristics of flares were found to be more common among patients who were currently flaring. In particular, the mean percentage of BSA affected by PsO was significantly greater in patients with current flares than in those in the other 2 patient groups. Active tender or swollen joints, dactylitis, enthesitis, tendonitis, and axial symptoms were also more frequent in patients currently flaring (all analyses; P < 0.05; Supplementary Table S3).
Of patients with current flares, 50.5% were prescribed a bDMARD, as compared with 54.8% of patients who had previously flared but were not currently flaring and 43.3% of patients who had never flared were receiving a bDMARD (P = 0.004). Patients in current flare also were prescribed more nonsteroidal antiinflammatory drugs (34.7%), analgesics (20.0%), oral steroids (12.6%), and conventional synthetic DMARDs (54.7%) than patients in the other 2 patient groups (P < 0.05; Supplementary Table S4, available with the online version of this article).
Physician and patient alignment over flare status. Agreement between physicians and patients over current flare status (currently in flare vs not currently in flare) was observed in 93.4% of matched physician-patient pairs ( 0.59, 95% CI 0.49-0.68, P < 0.001).
0.59, 95% CI 0.49-0.68, P < 0.001).
Effect of physician-reported flare on QOL, functioning, and work impairment. Table 4 and Figure 2 show adjusted analyses of predicted PRO scores by patient flare status. Patients who had not flared in the last 12 months or had never flared were predicted to have an EQ-5D-5L utility score of 0.85 (Figure 2), which is predicted to be 0.24 points higher than patients in current flare (P < 0.01; Table 4). The average adjusted overall work impairment score was 18.0 in patients who had not flared in the last 12 months or had never flared (Figure 2), compared with an average score 27.5 points higher among patients who were currently flaring (P < 0.01; Table 4). HAQ-DI score was predicted to be 0.35 in those who had not flared in the last 12 months or had never flared (Figure 2), 0.57 points lower than patients who were currently flaring (P < 0.01; Table 4). The PsAID-12 score in patients who were currently flaring was 5.7 (Figure 2) and was predicted to be 3.1 points higher in those who were currently flaring (indicating greater effect of disease) compared to patients who had not flared in the last 12 months or had never flared (P < 0.01; Table 4).
Multivariate logistic regression analyses showing the impact of physician-reported patient flare status on PRO scores.

{kind=link}
{kind=link}
Marginal means models showing predicted PRO scores according to physician-reported patient flare status. Models adjusted for gender, age, time since diagnosis, employment status, BMI, and number of joints and percentage BSA affected. BSA: body surface area; EQ-5D: EuroQol 5-Dimension; HAQ-DI: Health Assessment Questionnaire–Disability Index; MCID: minimum clinically important difference; PRO: patient-reported outcome; PsAID12: 12-item Psoriatic Arthritis Impact of Disease questionnaire; VAS: visual analog scale; WPAI: Work Productivity and Activity Impairment questionnaire.
In unadjusted analyses, 85% of patients without flares in the last 12 months or who had never flared were satisfied or very satisfied with their treatment compared with patients with current flares (28.9% satisfied or very satisfied; Table 5). Of physicians whose patients had been without flares in the last 12 months or who had never flared, 89.1% were satisfied or very satisfied with treatment compared to physicians whose patients were currently flaring (22% satisfied or very satisfied). Adjusted and descriptive analyses showing the association between patient-reported flaring status and QoL, functioning, and work impairment are shown in Supplementary Tables S5 and S6 (available with the online version of this article).
Descriptive analyses of patient- and physician-reported satisfaction with treatment according to physician-reported patient flare status.
DISCUSSION
This study shows that flares are frequent in PsA, with 29.5% of patients experiencing a flare in the past 12 months, according to physicians. Flare status was found to have a significant effect on clinical outcomes and PROs, with patients who had not flared in the last 12 months or had never flared having a higher QOL, lower overall work impairment, and a lower degree of disability compared with patients who were currently flaring.
Although it is challenging to consider flare when evaluating disease status in PsA, in part because of the absence of a clear definition of flare,5 it could be broadly considered as a period of worsening in disease activity. As our study demonstrated, this worsening has a significant effect on patients. For example, QOL, work productivity, effect, and functionality were all affected to the greatest degree in patients who were currently flaring. A general population normative value for the EQ-5D-5L index is a score of 0.88 on a 0 to 1 scale (with a higher scoring representing better QOL), with a minimum clinically important difference (MCID) of 0.07.20 Patients in our study who were currently flaring had an average EQ-5D utility value of 0.57, suggesting a much-reduced QOL at the time of data collection. This pattern was also observed in the HAQ-DI, with a population normative value of 0.25 on a scale of 0 to 3 (lower scoring representing less impaired functionality), and an MCID of 0.22,21 in comparison to a much worse score of 1.10 among the patients included in this study who were currently flaring. Similarly, patients currently flaring or who had flared in the last 12 months reported higher work productivity impairment compared to patients who had not flared ever or in the last 12 months; other studies have reported similar findings, with patients in flare being less likely to be in full-time work22 and experiencing greater work productivity loss.23 Previous studies corroborate that flare in PsA imposes a considerable QOL burden to patients.24 Although patients with current flare had worse clinical outcomes than patients not in flare, they were less likely to be prescribed a bDMARD even after adjustment for PsA disease duration. This may be a result of this study not capturing follow-up data over time. However, an association between lower use of bDMARD and flare is suggested. We found a high level of agreement between physicians and patients in terms of identifying if a flare was currently occurring; however, there was less agreement on the severity of the flare, with patients more commonly reporting moderate or severe flares. This may have been because physicians and patients did not agree on the symptoms that constituted a worse flare. For example, a study investigating physician-patient agreement on flare indicators reported that although physicians and patients agreed on almost all domains as important symptoms of flare, fatigue was reported as an important symptom by more patients than physicians and skin and participation were rated as more important by physicians than patients.25
Our study also showed that physicians and noncurrently flaring patients reported similar degrees of satisfaction with current treatment, but that patients who were currently flaring reported a higher degree of dissatisfaction than physicians. It can be concluded that further studies of patients’ expectations and of the prognostic value of different disease states/definitions of long-term outcomes are needed to inform optimal treatment strategies.
Ultimately, this study contributes to the growing evidence on factors that are important to patients with PsA, which will hopefully ensure that appropriate measures are used for the assessment of PsA in clinical practice. Physicians examining patients with PsA need to be aware of the heterogeneous presentation of flaring in PsA and response to treatment. This suggests that the evaluation of PsA disease activity and impact through patient self-reporting is important for directing physicians’ decisions on disease management.26 The results of this study signal the importance of assessing disease domains and the effect of flare on disease burden.
This study has several limitations. First, it was noninterventional, with physicians completing forms on consecutive patients with PsA. It is acknowledged that patients who were visiting physicians more often were more likely to have been included in the study. Selection bias was possible as the physicians surveyed were a convenience sample and may have not been representative of the overall population of physicians treating patients with PsA. Some measures used in this study were not validated, such as the flare status questions presented to physicians and patients. Also, patients were encouraged, but not required, to complete their questionnaires, which led to missing data and fluctuating sample sizes across PROs. Nevertheless, we involved a high number of physicians, working in different settings across different geographical regions, and a mixture of private/public practices, thereby ensuring that the sample was likely to be representative of the overall population of patients with PsA. Another limitation is that it was difficult to collect data on concomitant conditions such as fibromyalgia, anxiety, and depression; indeed, we provided a list of comorbidities, but the prevalence observed in the present study for fibromyalgia (2.1%) is much lower than what has been reported in other studies.27,28 It is possible that the psychological distress of fibromyalgia may modify perceptions of flares; we cannot confirm this hypothesis in the present study, though no significant differences in concomitant conditions were observed for patients with and without flares.
Our study found that flares in PsA were frequent and led to patients experiencing significantly negative effects on their QOL, disability, and work productivity. Further studies focusing on the effectiveness of interventions to prevent and manage flaring in PsA are needed.
Footnotes
The analysis described here using data from the Adelphi PsA IV Disease Specific Programme was funded by Janssen.
AMO has received research grants to Johns Hopkins University from AbbVie, Amgen, Celgene, Horizon, Janssen, Eli Lilly, Novartis, and Pfizer; and consulting fees from BMS, Janssen, Eli Lilly, Novartis, Pfizer, and UCB. WT has received research grants from AbbVie, Celgene, Janssen, GSK, and Eli Lilly; and consulting fees from AbbVie, Amgen, Celgene, Janssen, Eli Lilly, MSD, Novartis, Pfizer, GSK, and UCB. SG is engaged in the research or services as a private consultant and not in their capacity as a Johns Hopkins faculty member. NB and EAH are employees of Adelphi Real World. SP and SDC are employees of Janssen. LG has received research grants from Amgen, Galapagos, Janssen, Eli Lilly, Pfizer, Sandoz, and Sanofi; and consulting fees from AbbVie, Amgen, BMS, Biogen, Celgene, Gilead, Janssen, Eli Lilly, Novartis, Pfizer, Samsung Bioepis, Sanofi-Aventis, and UCB.
- Accepted for publication July 26, 2022.
- Copyright © 2023 by the Journal of Rheumatology
This is an Open Access article, which permits use, distribution, and reproduction, without modification, provided the original article is correctly cited and is not used for commercial purposes.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.