
We are disappointed that the American College of Rheumatology (ACR) has changed its position from no recommendation to conditional recommendation against the use of intraarticular hyaluronic acid (IAHA) injections for osteoarthritis (OA) knee pain, as stated in the 2019 ACR Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee.1 The authors of this article, including Dr. Altman (a member of the 2000, 2012, and 2019 ACR Guideline Committees on OA Treatment who was physically absent during the decision process to alter the 2019 IAHA recommendation), believe this updated guideline is based on a paucity of and, perhaps, biased interpretation of the evidence. The 2019 ACR guideline mirrors that of the 2013 American Academy of Orthopedic Surgeons (AAOS),2 which was retained in the recent AAOS 2021 guideline update (https://www.aaos.org/OAK3CPG). However, both differ from other global organizations and are incongruous with the majority of published literature, which indicates that IAHA injections for OA knee pain are safe and at least as effective as the standard-of-care (SOC) medication including oral nonsteroidal antiinflammatory drugs (NSAIDs).3 Because the recent ACR guidelines have the potential to influence US clinical decision making and insurance policy, potentially limiting patient access to a safe and beneficial treatment, the ACR should reconsider the IAHA update in the 2019 guideline based on the evidence presented here.
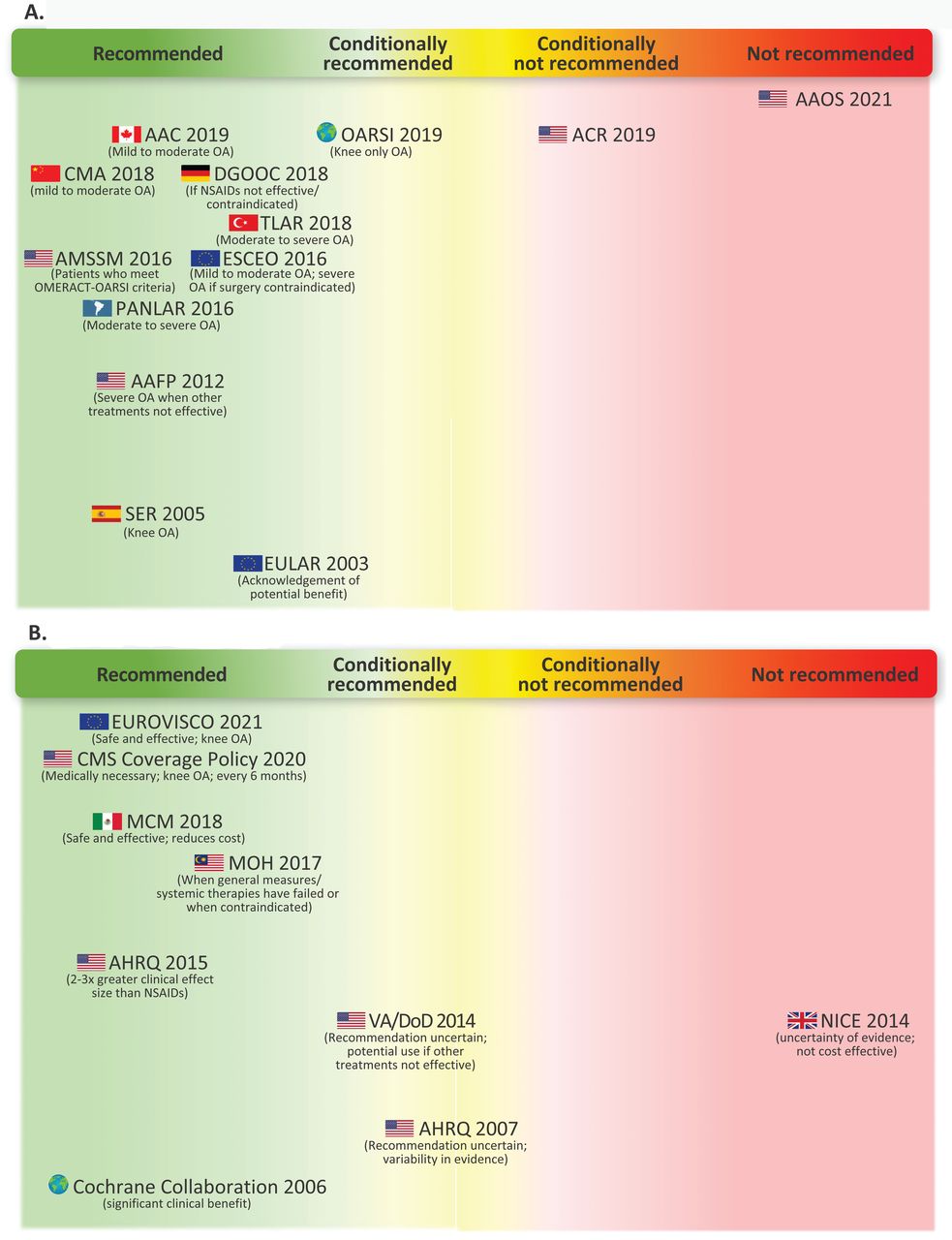
We identified 13 professional organizations and 8 global agencies focusing on musculoskeletal disease that published guidelines for IAHA (Supplementary References, available with the online version of this article). Of these, 86% (19/22) were either neutral or in favor of IAHA treatment for OA knee pain; only the ACR, the AAOS, and the National Institute for Health and Care Excellence had recommendations against IAHA use (Figure 1 and Supplementary Figure). Notably, both the European Alliance of Associations for Rheumatology and the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis published positive recommendations for IAHA use (Figure 1A). In fact, of the 8 global agencies from which a policy could be identified, 88% (7/8) stated that IAHA treatment is warranted and/or should be covered by insurance carriers. These policy recommendations included independent assessments by the Agency for Healthcare Research and Quality (AHRQ) and the Cochrane Collaboration for evidence-based medicine (Figure 1B). A recent systematic review published in the Orthopaedic Journal of Sports Medicine aligned with our findings, noting that 81% of identified clinical practice guidelines provided favorable or neutral recommendations for the administration of IAHA for OA knee pain.4
{kind=link}
Summary of selected global clinical practice guidelines for IAHA for treating OA Knee pain. (A) Professional societies. (B) Consensus agency, metaanalysis, and healthcare policy. AAC: Arthroscopy Association of Canada; AAFP: American Academy of Family Physicians; AAOS: American Academy of Orthopaedic Surgeons; ACR: American College of Rheumatology; AHRQ: Agency for Healthcare Research and Quality; AMSSM: American Medical Society for Sports Medicine; CMA: Chinese Medical Association; CMS: Centers for Medicare and Medicaid Services; DGOOC: German Society for Orthopaedics and Trauma; ESCEO: European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases; EULAR: European Alliance of Associations for Rheumatology; EUROVISCO: European Viscosupplementation Consensus Group; MCM: Mexican Consensus Meeting; MOH: Ministry of Health Malaysia; NICE: National Institute for Health and Care Excellence ; NSAID: nonsteroidal antiinflammatory drug; OA: osteoarthritis; OARSI: Osteoarthritis Research Society International; OMERACT: Outcome Measures in Rheumatology; PANLAR: Pan American League of Associations for Rheumatology; SER: Spanish Society of Rheumatology; TLAR: Turkish League Against Rheumatism; VA/DoD: Veterans Affairs/Department of Defense.
We believe the discrepancy between the 2019 ACR guideline and international guidelines hinges on the ACR’s exclusion of pivotal IAHA literature. The ACR dismisses a 30-year global history of IAHA use by citing a single 10-year-old review by Rutjes et al as the basis for the 2019 updated recommendation.5 This review concluded that evidence of IAHA clinical benefit was restricted to studies with “high risk of bias.” The review5 focused on trials deemed by the authors to have a “low risk of bias,” many of which are not published (and therefore not auditable) and involved non-U.S. Food and Drug Administration (FDA)-approved IAHA products. The review by Rutjes et al is the only publication to report an insignificant effect size difference between IAHA and IA saline. In contrast, a metaanalysis of 12 overlapping metaanalyses,6 which included the metaanalysis by Rutjes et al,5 concluded that IAHA is an effective intervention for OA knee pain. The metaanalysis by Xing et al6 extracted the overall findings of Rutjes et al that support the use of HA but noted that the misinterpretation of effect size statistics and the inclusion of unpublished, unverified data affected the overall conclusions drawn in that study.
As a result of relying on the Rutjes et al review,5 the ACR guideline overlooks fundamental studies of IAHA including a metaanalysis by Bannuru et al,3 the only published study to rank the clinical effect sizes of commonly used pharmacologic agents for treating OA knee pain. Bannuru et al3 demonstrated that IA steroid or IAHA injections have clinical effect sizes 2 to 3 times greater than SOC oral pain medication comparators including NSAIDs. That this study4 was sponsored by the AHRQ at the request of the Centers for Medicare and Medicaid Services suggests that it is an unbiased study and should have been included in any comprehensive examination of the literature. Additionally, studies have suggested a large placebo effect for IA saline injections in clinical studies.3 It is important to consider this beneficial clinical effect when interpreting clinical trial results with IA saline as the comparator. The new ACR guideline also does not address the contrasting safety profiles of locally delivered IAHA and systemic oral analgesics for chronic pain management. IAHA has no known systemic side effects or drug interactions.7 In contrast, the adverse effects associated with NSAIDs have prompted the FDA to release a black box warning for NSAIDs for cardiovascular and gastrointestinal risks (https://www.fdanews.com/articles/73674-fda-releases-black-box-template-for-nsaid). It is therefore problematic that the new ACR guideline favors systemic NSAIDs when, for many patients, it cannot be inferred that “benefits clearly outweighed harms and burdens” (as defined in the ACR guideline).1 Further, at the present time when narcotic abuse is a national crisis, it seems imprudent to limit safe, nonnarcotic analgesic options by discouraging the use of IAHA, for example, wherein there is no potential for abuse.8 In addition, use of IAHA has recently been correlated with reduced risk of requiring total knee arthroplasty.9
Surprisingly, the ACR Committee states that its “recommendations are not intended to dictate payment or insurance decisions.”1 Clearly, the ACR underestimates the effect their recommendations will have on insurance decisions. Unfortunately, the 2013 AAOS guideline,2 which had a similar recommendation, has been cited by many insurance carriers to implement IAHA noncoverage policies and has resulted in the loss of IAHA coverage for almost 64 million patients in the past 5 to 6 years.10 The new ACR guideline will likely augment this negative trend.
Professional society guidelines have pivotal influence on clinical decision making and insurance policies and should be crafted with the utmost caution. In its most recent statement regarding IAHA, the ACR therefore contradicts its conclusion that “clinicians and patients should engage in shared decision-making that accounts for patients’ values, preferences, and comorbidities. These recommendations should not be used to limit or deny access to therapies.”1 Consequently, we strongly encourage the ACR Committee on Guidelines to reconsider all available data, to recognize and take responsibility for their statement’s potential negative effect on patient access to treatment, and to revise their recommendations to include the use of IAHA as a valuable treatment option for OA knee pain. We also ask that the ACR Committee honor its prior position focusing on the maintenance of autonomy in clinical decision making. Without a revision, the current ACR guideline will only exacerbate the current trend of limiting clinicians’ autonomy and denying patient access to efficacious and safe treatment options where limited treatment options for OA knee pain exist.
ACKNOWLEDGMENT
Publication management was provided by AOIC, LLC and funded by OrthogenRx. All listed authors meet the criteria for authorship set forth by the International Committee for Medical Journal Editors. Editorial support (assembling tables, collating author comments, copyediting, fact checking, and referencing) and graphic services were provided by AOIC, LLC and were also funded by OrthogenRx.
Footnotes
This study was funded by OrthogenRx. MJD is a former employee of and stockholder in OrthogenRx. TCA is a stockholder in OrthogenRx. The remaining authors declare no conflicts of interest relevant to this article.
- Copyright © 2022 by the Journal of Rheumatology
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.