
Axial spondyloarthritis (axSpA) and diffuse idiopathic skeletal hyperostosis (DISH) involve tendon and ligament ossification showing similarity on spinal radiographs. Differentiating axSpA from DISH facilitates proper treatment and improves inflammatory pain; however, the overlap between axSpA and DISH delays its diagnosis.
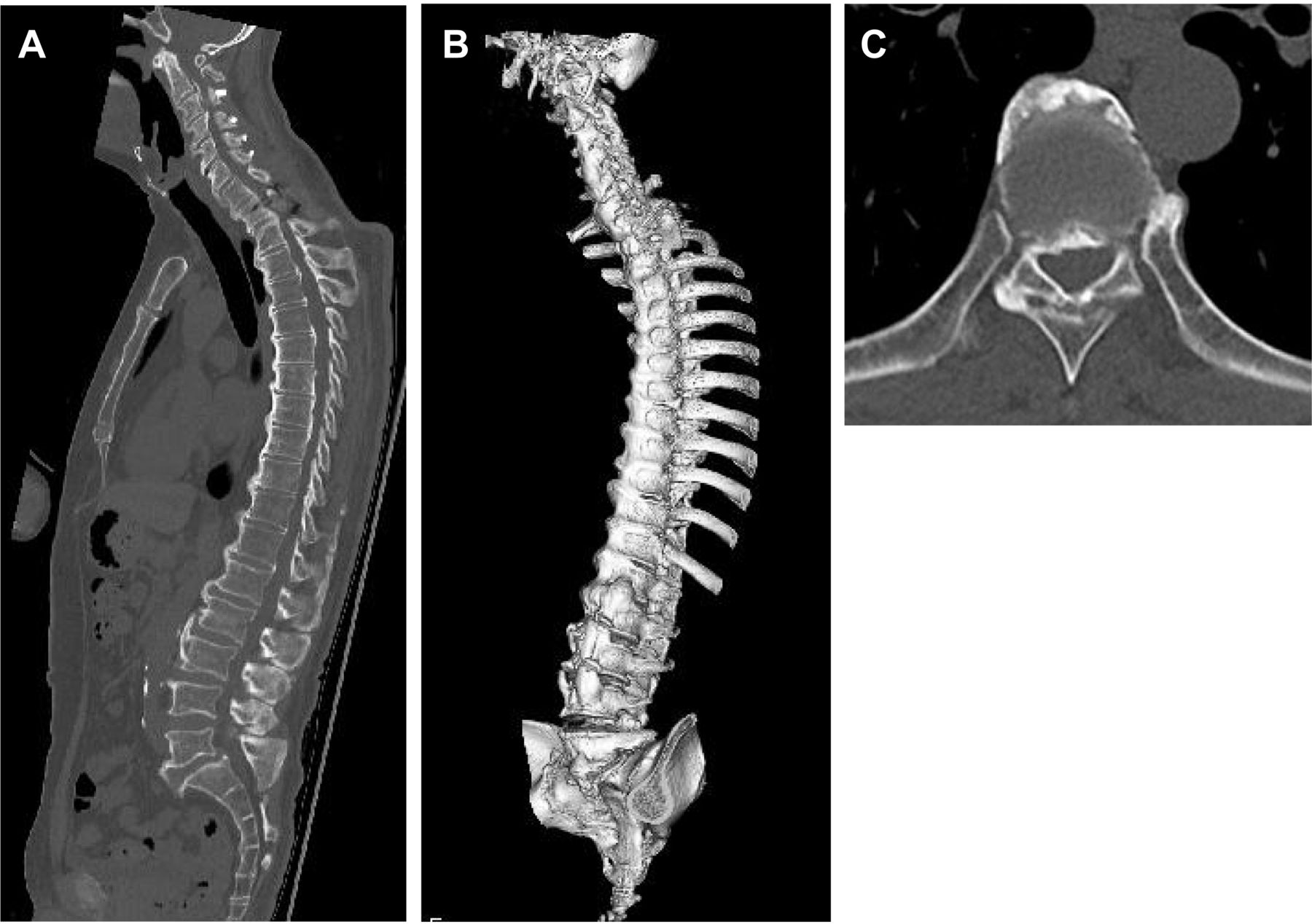
A 58-year-old man presented to our hospital with a 38-year history of back pain and stiffness. The patient had received the diagnosis of both DISH and ossification of the posterior longitudinal ligament. He had a partial response to nonsteroidal antiinflammatory drugs. On examination, the pain was consistent with the features of inflammatory back pain. He had impaired spinal mobility and tenderness around the left shoulder joint. Laboratory studies showed elevated C-reactive protein (CRP) of 2.8 mg/L and were negative for HLA-B27. Although pelvic radiographs revealed grade 2 bilateral sacroiliitis with irregular bone margin, magnetic resonance imaging (MRI) did not show any bone edema in sacroiliac joints. Whole-body MRI demonstrated abnormal signals of entheseal sites in left shoulder. While spinal computed tomography (CT) showed flowing anterior ossification and bone growth > 45° to the horizontal axis, which are typical for DISH (Figure 1A), the images with 3-D reconstruction also revealed bridging of the vertebral bodies at bilateral rim including posterolateral region (Figure 1B) and fusion of the facet joints (Figure 1C) that suggested syndesmophytes characteristic of axSpA.1,2

{kind=link}
Radiographic images of axSpA in diffuse idiopathic skeletal hyperostosis (DISH). (A) Sagittal CT image showing a flowing anterior ossification and bone growth > 45° to the horizontal axis, which are typical for DISH. (B) Spinal CT with 3-D reconstruction demonstrating bridging of the vertebral bodies at bilateral rim, especially posterolateral region. (C) Axial CT of thoracic and lumbar spine showing sclerosis and fusion of the facet joints. Panels B and C suggest the syndesmophytes seen in axial spondyloarthritis. CT: computed tomography.
These findings confirmed the coexistence of axSpA and DISH. A tumor necrosis factor inhibitor was initiated, and the patient had attenuation of the back pain and stiffness as well as diminished CRP. This case highlights the beneficial role of CT with 3-D reconstruction in differentiating axSpA from DISH.
ACKNOWLEDGMENT
We gratefully acknowledge the work of past and present members of our department.
Footnotes
The authors declare no conflicts of interest relevant to this article. The research ethics board of the authors’ institution does not require board review for a single case report when the patient’s privacy is protected. Written consent was obtained from the patient.
- Copyright © 2022 by the Journal of Rheumatology
REFERENCES
- 1.
- 2.