
Abstract
Objective Gout disproportionately affects older Pacific Islander and Black populations relative to White populations. However, the ethnic-specific determinants remain understudied within these groups, as well as within other ethnicities. We examined gout incidence and associations with behavioral factors, including diet, alcohol, and smoking, within a large multiethnic population of older adults from the Multiethnic Cohort Study, which linked prospective cohort data to Medicare gout claims between 1999–2016.
Methods Using samples of Black (n = 12,370), Native Hawaiian (n = 6459), Japanese (n = 29,830), Latino (n = 17,538), and White (n = 26,067) participants, we conducted multiple Cox regressions, producing hazard ratios (HRs) and 95% CIs.
Results Relative to White individuals, Native Hawaiians had the highest risk of gout (HR 2.21, 95% CI 2.06–2.38), followed successively by Black and Japanese participants, whereas Latino individuals had a lower risk of gout (HR 0.78, 95% CI 0.73–0.83). Alcohol use was associated with an increased risk, with significantly greater effects observed among Japanese participants drinking ≥ 3 drinks per day (HR 1.46, 95% CI 1.27–1.66), or > 5 beers per week (HR 1.29, 95% CI 1.17–1.43), compared to White individuals (Pinteraction < 0.001). Former smokers with ≥ 20 pack-years had an increased risk (HR 1.14, 95% CI 1.06–1.22). Higher dietary quality was associated with a decreased gout risk, with the largest effect observed among White participants (HRQ5vsQ1 0.84, 95% CI 0.79–0.90), whereas vitamin C was weakly associated with a decreased risk of gout only among Japanese individuals (HR 0.91, 95% CI 0.85–0.98).
Conclusion Overall, notable ethnic differences were observed in both gout risk and associations with modifiable behavioral factors. Our findings offer crucial insights that may improve precision in preventing and managing gout.
- ethnic groups
- gout
- lifestyle factors
- proportional hazards models
Gout is the most common rheumatic disease, affecting up to 6.8% of the world’s population, including 9.2 million adults in the United States.1,2 Characterized by moderate-to-severe acute pain and inflammation, periods of remission, and long-term chronic inflammation and disfigurement caused by the accumulation and deposition of monosodium uric acid crystals during hyperuricemia, gout is a debilitating condition with substantial implications for a patient’s quality of life.3 The disability-adjusted life-years of gout have increased over the past few decades, especially in the US.4 Moreover, gout presents not only a substantial societal and personal burden but also a financial one. In a systematic review of the economic burden of gout, gout-related costs range between US $172 to $6179 per capita annually, with costs considerably greater among older adults.5 Additionally, factoring in the various comorbidities associated with gout, the indirect costs likely exceed these estimates.
The burden and risk of gout differs significantly by demographic characteristics, particularly age, sex, race/ethnicity, and genetics.6 Globally, gout prevalence is higher in men compared to women, with differences becoming less pronounced in older adulthood.7 As a condition strongly associated with the aging process, incident cases of gout are expected to increase worldwide in the coming decades; coinciding with an aging population, these cases have already doubled over the past 20 years.8,9 The World Health Organization projects a rapid increase in the world’s proportion of adults aged > 60 years in the next few decades, nearly doubling by the year 2050 from the most recent estimates.10
With global cases likely to rise significantly, further investigation into the determinants of gout is necessary to the prevention, intervention, and identification of those at high risk. Understanding underlying differences in risk between populations remains a critical gap in prioritizing public health efforts targeting gout. Thus, this study aimed to examine the incidence and behavioral determinants of gout among understudied populations from a large multiethnic cohort of older adults with no history of gout.
METHODS
The Multiethnic Cohort Study. This study utilized data collected from the Multiethnic Cohort Study (MEC).11 The MEC is a large prospective study following a cohort of 215,251 men and women aged 45–75 years at the time of entry (1993–1997), from the Los Angeles area (51%) and Hawai‘i (49%). The study aimed to explore associations between lifestyle factors (primarily dietary components) and cancer and other chronic diseases within 5 racial/ethnic groups: White, Japanese American, Native Hawaiian, Black, and Latino. At baseline, all participants completed a 26-page self-administered questionnaire containing items pertaining to their demographic characteristics, medical histories, physical activity, dietary behaviors, and medication and supplement use. Recruitment and sampling methodologies have been summarized elsewhere.11 The MEC participants were linked to Centers for Medicare & Medicaid Services (CMS) fee-for-service insurance claims data from 1999 to 2016 through methodology previously reported.12 Participation was voluntary and all participants provided written informed consent. The study protocol was approved by the institutional review boards of the University of Hawai‘i (2018-00912) and the University of Southern California (HS-16-00719).
Study population. The derivation of the final analytic sample for the present study is presented in Figure 1. We included MEC participants who were linked to the CMS database, were fee-for-service Medicare enrollees, and belonged to 1 of the 5 major racial/ethnic groups in the MEC. Participants were excluded if they indicated a history of gout in the baseline questionnaire, had inconsistent dates (death prior to gout or claim date prior to Medicare enrollment), or exited the cohort for any reason prior to age 65 years. Of the 215,640 MEC participants, 92,264 participants (12,370 Black, 6459 Native Hawaiian, 29,830 Japanese, 17,538 Latino, and 26,067 White) were included in our final analytic sample. There were no significant differences between participants excluded due to covariate missingness by the outcome within the total sample or racial/ethnic subsamples.
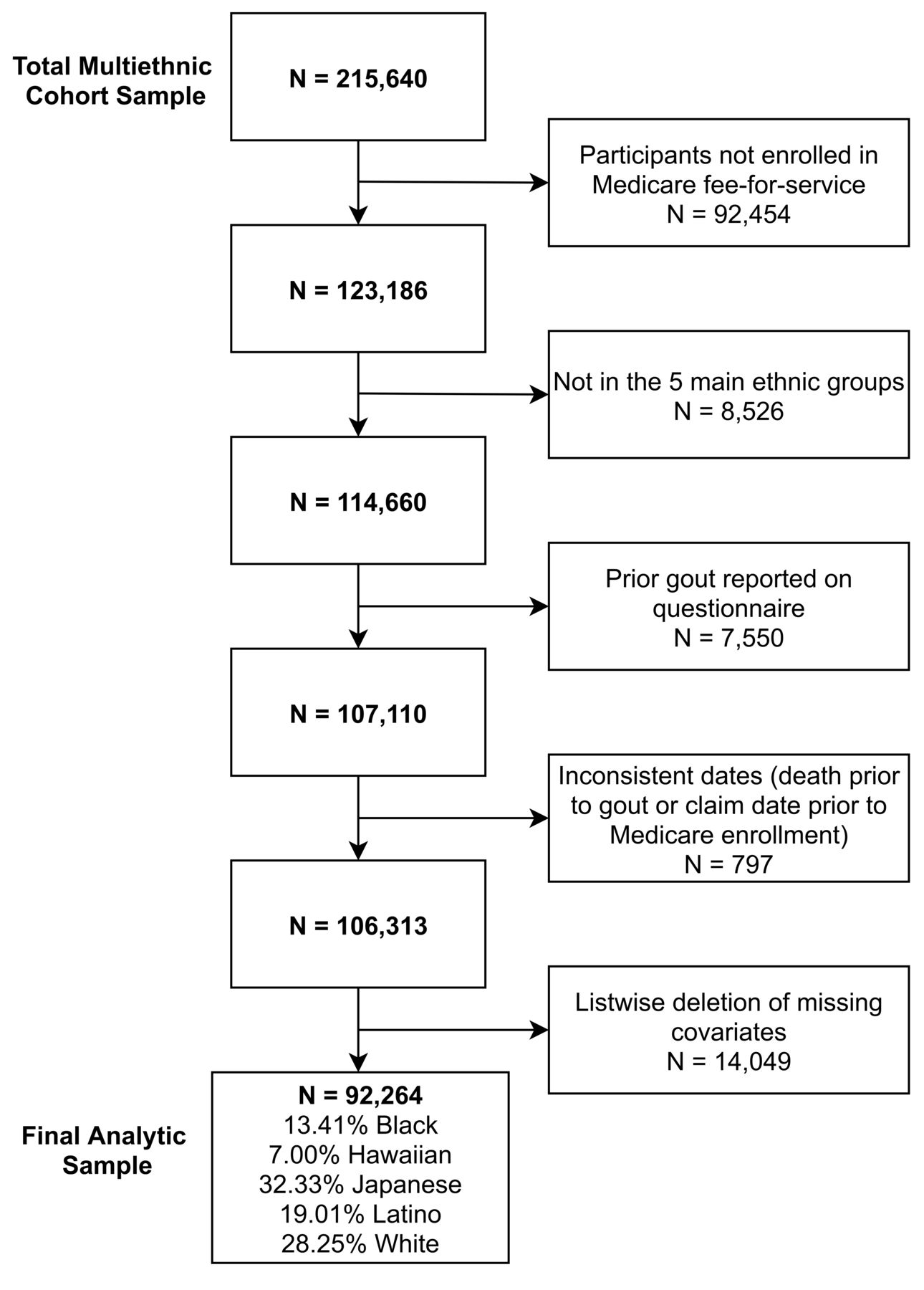
Analytic sample derivation.
Case ascertainment. We considered insurance claims for gout through Medicare to be equivalent to a gout case diagnosis by a physician. International Classification of Diseases, 9th revision (ICD-9) code 274.9 and ICD-10 code M10.9 were used to identify gout diagnoses. Follow-up began at Medicare linkage (1999) and ended upon gout diagnosis, death, or completion of the observation period (December 31, 2016). The follow-up period for participants too young (54.29%) to be enrolled in Medicare in 1999 began the year of their 65th birthday, and thus had a shorter period of observation; the average period of observation was approximately 9.56 years.
Demographics. Data for the demographic characteristics were ascertained from self-reported responses to the 1993–1996 MEC baseline questionnaire, including date of birth; sex (male or female); marital status (married, separated, divorced, widowed, or never married); birthplace of participant, mother, and father (US or other); racial/ethnic background (Black, Native Hawaiian, Japanese, Mexican/Other Hispanic, White, or other); and years of school completed (high school or less, vocational school or some college, and graduated college or graduate/professional school). Self-reported race/ethnicity, sex, marital status, and education level were considered as potential confounders because previous studies have reported associations between these variables and many of the lifestyle measures of interest in this study—smoking status,13,14 vitamin supplementation,15 diet,16 and alcohol use17,18—as well as gout.19,20,21 Generation in the US was derived from the self-reported birthplace of the participant and those of the participant’s parents. First-generation participants included those born outside the US who had since immigrated to the study location. Second-generation participants were defined as individuals born in the US, with at least 1 parent born in another country; greater than second generation was defined as the participant and both parents being born in the US. Generation in the US was considered a possible confounder due to prior associations detected between immigration, lifestyle factors, and gout.21,22,23
Behavioral factors. Modifiable lifestyle exposures were determined by self-report from the MEC 1993–1996 baseline questionnaire and were selected on the basis of previous associations detected between each factor and gout or uric acid. These modifiable lifestyle factors included cigarette smoking,24 vitamin C supplementation,25 alcohol use,26 and dietary behaviors.27 Respondents reported their current smoking status (current, past, or never smoker), total number of years spent smoking, and average number of cigarettes per day. Pack-years (< 10, 10–19, or ≥ 20) were calculated by multiplying the number of 20-cigarette packs smoked per day by the number of years smoked for current and past smokers. Vitamin C supplementation (yes or no) was ascertained by asking respondents whether they had taken a vitamin C supplement by itself in the past year at least once a week.
Diet and alcohol use were ascertained using a validated28 food frequency questionnaire with over 180 items pertaining to dietary intake of specific foods and beverages, including wine, beer, and hard liquor, over the past year. We calculated the total number of standard alcoholic drinks per day from the total mean grams per day of ethyl alcohol consumed for each participant, with 14 grams corresponding to 1 standard drink. For each type of alcoholic drink, we converted the daily grams (of total beer, total wine, and total hard liquor) to fluid ounces per week, assuming a density of approximately 1.0 grams/cm3 (1 beer ≈ 12 fl oz, 1 wine ≈ 5 fl oz, and 1 hard liquor ≈ 1.5 fl oz). The average number of standard drinks for each alcoholic beverage was examined in 3 categories (< 1/week, 1–5/week, or > 5/week). Dietary quality was assessed by the Dietary Approaches to Stop Hypertension (DASH) diet29 adherence score quintiles, utilizing 8 components pioneered by Fung et al,30 yielding a sum component score ranging from 8 to 40 for each participant.31 We chose to use the validated DASH score because preliminary crude analyses revealed that DASH was the only dietary index available in the MEC31 that was associated with gout.
Other covariates. BMI and histories of other health conditions were also collected at baseline. BMI (kg/m2) was calculated from self-reported weight and height, whereas history of cardiovascular disease (CVD; hypertension, strokes, and heart attacks), diabetes, and kidney stones, were directly assessed through items on the baseline questionnaire. BMI and histories of CVD, diabetes, and kidney stones were included in our analyses because of their previously observed associations with demographic factors, behavioral exposures, and gout risk.8,32,33
Statistical analyses. Descriptive statistics were calculated to summarize baseline sample characteristics for the total sample and racial/ethnic sub-samples. We plotted the Kaplan-Meier cumulative hazards by ethnicity. Total sample and race/ethnicity-stratified Cox proportional hazard models of gout, with age as the time metric, were used to estimate hazard ratios (HRs) and 95% CIs. Multivariable models adjusted for race/ethnicity; sex; age; education level; generation in the US; marital status; BMI; and history of CVD, diabetes, and kidney stones. All modifiable factors were included in the multivariable models. All models were adjusted for total number of alcoholic drinks per day, except for those ascertaining effects of specific alcohol types. We examined adherence to the proportional hazards assumption with scaled Schoenfeld residuals (Supplementary Material, available from the authors on request). Sex was adjusted as a stratum variable in all models; race/ethnicity was included as stratum variables for the total sample model. We tested for interaction between each modifiable factor and race/ethnicity using a likelihood ratio test; significant overall interactions were investigated using interaction models with White participants as a reference group (Supplementary Material). All analyses were conducted using R version 4.0.5 with integrated development environment RStudio version 1.4.1106 (RStudio Team).
RESULTS
Baseline characteristics. Table 1 presents the baseline sample characteristics for the 92,264 MEC participants by ethnic group: Black, Native Hawaiian, Japanese, Latino, and White. In the total sample and across racial ethnic groups, there was a higher proportion of females to males, and most participants were married. Education level was highest among White and Japanese participants. The proportion of immigrants to the US was highest among Latino participants, whereas most Japanese participants were children of immigrants. BMI was highest among Native Hawaiian, and lowest among Japanese participants. Black participants had the highest proportion of CVD and the lowest proportion of kidney stones, whereas White participants had the lowest proportion of CVD and the highest proportion of kidney stones. Latino participants had the highest proportion of diabetes. Black and Native Hawaiian participants had the highest proportion of current smokers, with most Native Hawaiian current smokers reporting ≥ 20 pack-years. White participants reported the highest levels of vitamin C supplementation, total alcoholic drinks per day, standard wine glasses per week, standard hard liquor drinks per week, and DASH diet adherence. Consuming > 5 standard beers per week was most common among Native Hawaiian participants.
Baseline demographic characteristics of the multiethnic cohort linked to Medicare fee-for-service records by ethnicity.
Race/ethnicity-specific risk. Figure 2 presents the Kaplan-Meier cumulative hazards of gout over age at Medicare claim by race/ethnicity. A total of 9648 participants (10.46%) had a gout Medicare claim over the period of observation. Native Hawaiian participants had the highest risk of gout, with over twice the risk relative to White participants (HR 2.21, 95% CI 2.06–2.38). Black and Japanese participants had a risk of gout similar to that of White participants up until approximately age 80 years, when their relative risk increased. Overall, Black participants had a 34% (HR 1.34, 95% CI 1.26–1.43), and Japanese participants a 14% (HR 1.14, 95% CI 1.08–1.20) higher risk compared to White individuals. Latino participants had the lowest risk of gout claims compared to all other ethnic groups, with a 23% lower risk relative to White participants (HR 0.78, 95% CI 0.73–0.83).

{kind=link}
{kind=link}
Kaplan-Meier cumulative hazards over age by ethnic group.
Modifiable factors. The Supplementary Material (available from the authors on request) summarizes the crude analysis, and Table 2 summarizes the multivariable analysis, HR (95% CI) for modifiable behaviors on gout incidence for each ethnic subsample, as well as the P value of the overall likelihood ratio test for effect heterogeneity by ethnicity (Supplementary Material for crude and multivariable pairwise interaction significance). Effects of modifiable behaviors for the total sample, adjusting for ethnicity as a stratum variable in the multivariable model, are also reported. Overall, the effects of the modifiable factors attenuated in the multivariable models.
Multivariable ethnic-specific model for modifiable lifestyle factors.
Among past smokers, ≥ 20 pack-years corresponded to a 14% (HR 1.14, 95% CI 1.06–1.22) greater risk of gout compared to never smokers. Among current smokers, 10–19 pack-years were associated with a 12% (HR 1.12, 95% CI 1.01–1.23) greater risk relative to never smokers. We detected significant heterogeneity for the effect (Pinteraction = 0.02) of smoking by ethnicity. Among past smoker vs never smokers, the effect ≥ 20 pack-years was significantly lower (Pinteraction = 0.02) among Latino (HR 1.00, 95% CI 0.77–1.29) compared to White (HR 1.19, 95% CI 1.06–1.34) participants. Similarly, the effect of 10–19 pack-years for past smokers was weaker compared to that of White individuals (Pinteraction = 0.03) among Native Hawaiian (HR 0.89, 95% CI 0.73–1.08) past smokers.
Higher total alcohol intake was associated with an elevated risk of gout, with 1–2 drinks per day corresponding to 11% (HR 1.11, 95% CI 1.05–1.18), and ≥ 3 drinks per day corresponding to 38% (HR 1.38, 95% CI 1.28–1.49) increased risk of gout compared to never drinkers. In the model assessing specific alcohol types, ≥ 5 standard drinks per week of beer (HR 1.15, 95% CI 1.08–1.22), wine (HR 1.12, 95% CI 1.02–1.22), or hard liquor (HR 1.20, 95% CI 1.11–1.30) were associated with an elevated risk of gout, relative to none of each type. Alcohol intake was a risk factor for gout in all ethnic groups. However, we observed significant effect modification by ethnicity for total alcohol (Pinteraction < 0.001) and beer consumption (Pinteraction < 0.001), but not for wine or hard liquor. Compared to White participants (HR1–2vs0 1.11, 95% CI 1.01–1.22; HR≥3vs0 1.43, 95% CI 1.26–1.61), the effect of 1–2 drinks per day was significantly greater (HR 1.18, 95% CI 1.07–1.30) among Japanese participants (Pinteraction = 0.01), whereas the effect of ≥ 3 drinks per day was significantly lower (HR 1.21, 95% CI 0.96–1.51) among Latino participants (Pinteraction = 0.01). Similarly, the effect of 1–5 beers per week (HR 1.16, 95% CI 1.03–1.31) and > 5 beers per week (HR 1.29, 95% CI 1.17–1.43) among Japanese participants was significantly higher (Pinteraction < 0.001 and Pinteraction = 0.003, respectively) compared to White participants (HR1–5vs0 0.96, 95% CI 0.84–1.09; HR>5vs0 1.16, 95% CI 1.03–1.32), whereas the effect of > 5 beers per week was significantly lower (HR 0.86, 95% CI 0.71–1.04) among Latino participants (Pinteraction < 0.001).
In the total sample, vitamin C supplementation was weakly associated with a lower risk of incident gout (HR 0.96, 95% CI 0.92–1.00). Significant effect modification was observed by race/ethnicity (Pinteraction = 0.02). Specifically, the effect of vitamin C supplementation was significantly (Pinteraction = 0.03) greater among Japanese (HR 0.91, 95% CI 0.85–0.98) compared to White participants (HR 1.03, 95% CI 0.94–1.12). Last, the highest quintile of the total DASH scores was significantly associated with a decreased risk of gout incidence (HRQ5vsQ1 0.84, 95% CI 0.79–0.90) relative to the lowest quintile; the observed protective effect of higher DASH adherence did not significantly differ by race/ethnicity.
DISCUSSION
We observed evidence of ethnic disparities and effect modification by ethnicity for gout incidence among older adults with no prior history of gout. Native Hawaiians had the highest risk of gout, with over twice the risk observed relative to White participants. Examination of modifiable lifestyle behaviors on incident gout revealed a higher risk associated with smoking, total alcohol use, and consumption of beer, wine, and hard liquor, as well as a lower risk associated with vitamin C use and adherence to the DASH diet. We observed significant differences in the effect of certain lifestyle factors on gout risk by race/ethnicity. Compared to White participants, the risk-elevating association between smoking, total alcohol intake, and beer consumption was lower among Latino participants, while total alcohol intake and beer consumption was associated with a greater risk among Japanese participants. Finally, the observed protective effect of vitamin C supplementation was greater among Japanese compared to White participants.
Our findings are consistent with the literature of gout incidence and prevalence observed among Pacific Peoples, primarily in New Zealand.34 For instance, a systematic review found a proportion of gout cases among New Zealand Māori approximately 3 times higher than that in New Zealand Europeans.35 Prior literature on the disparity between Black and White populations in gout incidence is consistent with our findings. An investigation of racial differences within the Atherosclerosis Risk in Communities study36 in 2014 reported that Black participants had a disproportionately higher sex-specific incidence of gout compared to White participants. Another finding consistent with prior literature is the notably low incidence of gout among Latino participants; data examining the number of patients with a gout diagnosis across 3 national ambulatory surveys found that Hispanic/Latino individuals were less likely to have a visit with gout compared to Non-Hispanic/Latino individuals.37 Incident gout among the Japanese participants was unexpectedly high given the markedly low prevalence reported from Japan.38 This finding may be attributed to acculturation with Western lifestyles,39 and/or the larger proportion of the Japanese population of Okinawan descent within the Hawai‘i-born population, which is a culturally and ethnically distinct group.40,41 However, with increasing evidence of gout heritability,42 recent findings suggest individuals of Asian descent may have an elevated frequency of gout risk–associated alleles compared to Europeans, potentially adding to the effects attributed to lifestyle acculturation.43
Behavioral factors had similar relationships with gout reported in prior literature utilizing less diverse populations, with a higher gout risk attributed to alcohol use and smoking,44 and protective effects from vitamin C supplementation25 and DASH diet.27 Alcohol use is thought to contribute to both the overproduction and underexcretion of urate, leading to hyperuricemia and gout.9 Beer, a particularly purine-rich alcoholic beverage, may increase uric acid production through the catabolism of common purines, such as guanosine, whereas alcohol use in general may downregulate excretion of uric acid by producing lactic acid, which competitively inhibits urate secretion.45 Our results further suggest that these pathways may be modified by ethnicity, with stronger effects of beer and total alcohol among Japanese, and weaker effects among Latino individuals, relative to White participants. These differences may suggest that there is a potential interaction between population genetic structure and alcohol use, or that the effects of population genetics are mediated by alcohol use. Alternatively, differences in the observed effect may be driven by differences in the presence or absence of confounding factors between groups. While our results suggest a higher risk among former smokers with ≥ 20 pack-years, particularly for White and Black participants, a metaanalysis examining the effects of smoking status reported conflicting results from several large studies, suggesting that smoking may not be causally related to gout.24 Thus, the lack of consistency observed in the smoking analyses may be more reflective of differential survival probability in heavy smokers or other risk factors that cluster with smoking, rather than a causal association. Moreover, with limited literature on the relationship between smoking and gout, the mechanism behind these associations remains elusive. While there are conflicting results from observational studies on the effect of vitamin C supplementation, a recent metaanalysis found a significant uric acid–lowering effect across 16 randomized controlled trials.25 Vitamin C may increase uric acid excretion by competitively inhibiting reabsorption and increasing glomerular filtration rates.46 We observed a weak protective effect of vitamin C supplementation, with the effect significantly greater among Japanese relative to White participants. A potential explanation for this difference may be differences in intake source. Japanese MEC participants had the lowest dietary intake of vitamin C relative to the other ethnic groups.11 Thus, Japanese participants may benefit more from supplemental vitamin C because other groups account for the effect of vitamin C in their diet. Finally, prior findings on dietary factors associated with gout largely reflect the components of the DASH diet, such as high levels of fruits, vegetables, and low-fat dairy products, as well as low levels of red meat, sweetened beverages, and sodium.1,27 Similar to alcohol consumption, different food groups may contribute to both overproduction and underexcretion of uric acid. For instance, consuming fructose leads to the depletion of adenosine triphosphate and increases uric acid levels; moreover, fructose may convert to lactic acid, which then competes with uric acid for excretion.47 Similar associations offer support for the observed protective effect from adherence to the DASH diet.27
Our study is not without limitations. First, all baseline factors were self-reported, and may have led to exposure misclassification, particularly for behaviors influenced by social desirability. However, these measures were collected well before gout diagnosis (average of 21 yrs prior) and are unlikely to be differentially misreported. Second, access to care is known to differ by race/ethnicity,48 and this difference may have contributed to delays in gout diagnosis, affecting the time-to-event analyses. That is, we were unable to differentiate Medicare gout claim and the disease onset, affecting our ability to accurately define the temporal relationship between exposure and outcome. Third, we were unable to include Medicare participants enrolled in health maintenance organization (HMO) programs because these programs do not provide individual claims data. Thus, our study was limited to Medicare recipients enrolled in a fee-for-service plan only, possibly affecting the generalizability of our findings. Moreover, because our study was limited to Medicare-eligible participants (ie, age ≥ 65 yrs) with no history of gout, our results may be generalizable only to individuals at risk of becoming an incident case in older adulthood. Because Pacific Islanders are known to have an earlier onset of gout relative to other ethnic groups,34 the observed incidence of gout among Native Hawaiians is likely underestimated relative to the general population. Finally, clinical gout may mimic the symptoms of rheumatoid arthritis, which is more common in women than men, possibly resulting in underdiagnosis among women.49
Our study offers crucial insights into the ethnic differences in the risk of gout and the ethnic-specific effects of modifiable factors. These findings may improve precision in identifying individuals at risk and preventing disease progression, thereby reducing the overall burden attributed to gout. Recent trends suggest an increasingly ethnically diverse older population, particularly in the US.50 Thus, further examination into how the distribution and determinants of chronic conditions differ between groups is vital in planning for a global aging population. Future investigations can expand this work by examining the modifying effects of sex within ethnic strata, identifying predictors of recurring attacks to further elucidate the long-term effects of poorly controlled gout, and calculating the financial cost of gout within underserved groups.
Footnotes
This study received no funding support. The interview data from the Multiethnic Cohort Study were collected and maintained by the University of Hawai‘i Cancer Center, Honolulu, and sponsored by the National Institutes of Health, National Cancer Institute (U01 CA164973).
This study was adapted from a portion of the Master of Science thesis of MDT. The authors declare no conflicts of interest relevant to this article.
- Accepted for publication January 14, 2022.
- Copyright © 2022 The Journal of Rheumatology
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.