
Abstract
Objective. The risk of clinically manifested major cardiovascular (CV) events in primary Sjögren syndrome (pSS) remains unclear. This study aimed to assess myocardial fibrosis in pSS and investigate the associated disease characteristics by cardiac magnetic resonance imaging (cMRI).
Methods. We performed a cross-sectional study of patients with pSS without cardiac symptoms. Labial gland biopsy was documented in 44 patients (85%). Patients without CV risk factors underwent contrast-enhanced cMRI. Late gadolinium enhancement (LGE) was used to assess myocardial fibrosis. Myocardial edema was assessed using T2-weighted imaging (T2WI). We compared the left ventricular (LV) geometry and function between the groups with and without LGE. Further, we explored the associations of cMRI abnormalities with pSS characteristics.
Results. Fifty-two women with pSS (median age 55, IQR 47.0–65.7 yrs) were enrolled in the study. LGE was observed in 10 patients (19%), two of whom showed high intensity on T2WI. High intensity on T2WI was observed in 3 patients (5.8%). LV mass index and LV mass/end-diastolic volume tended to be higher in the LGE-positive group than in the LGE-negative group (P = 0.078 and 0.093, respectively). Salivary gland focus score (FS) ≥ 3 was independently associated with LGE-positive in the multivariable analysis (OR 11.21, 95% CI 1.18–106.80).
Conclusion. Subclinical myocardial fibrosis, as detected by cMRI, was frequent in patients with pSS without cardiac symptoms. Abnormal cMRI findings were associated with salivary gland FS ≥ 3.
- cardiac magnetic resonance imaging
- late gadolinium enhancement
- myocardial fibrosis
- primary Sjögren syndrome
- salivary gland focus score
Primary Sjögren syndrome (pSS) is an autoimmune rheumatic disease in which exocrine glands such as the salivary and lacrimal glands are infiltrated by lymphocytes, causing inflammation and reduced exocrine function. It may also affect various organs, with extraglandular symptoms. It shares many clinical and pathophysiological characteristics with other autoimmune rheumatic diseases. Previously, many studies have reported increased cardiovascular disease (CVD) morbidity and premature mortality in patients with rheumatic diseases, such as systemic lupus erythematosus and rheumatoid arthritis (RA)1,2. A recent metaanalysis of CVD demonstrated the odds of heart failure (HF) were more than 2.54-fold higher for patients with pSS versus controls3. However, the prevalence of myocardial abnormalities in pSS remains uncertain. Importantly, myocardial abnormalities are typically clinically silent in patients with RA4 and may explain the paucity of case reports of cardiac complications in patients with pSS, since clinical and pathophysiological characteristics are often shared between RA and pSS.
Myocardial histopathology currently relies heavily on information obtained from an endomyocardial biopsy. However, this method is highly invasive and can be performed in limited patients. Rapid advancement in cardiac magnetic resonance imaging (cMRI) has enabled the evaluation of preclinical structural and functional changes in the left ventricle that precede the development of overt HF less invasively than endomyocardial biopsy5. Krumm, et al reported in a retrospective study that 13 (69%) of 19 patients with systemic sclerosis (SSc) and myocardial fibrosis, diagnosed based on endomyocardial biopsy, had late gadolinium enhancement (LGE), as confirmed by visual analysis6. While we have previously evaluated myocardial fibrosis in patients with RA and SSc using cMRI7,8, no studies have evaluated myocardial fibrosis in a substantial number of patients with pSS. We hypothesized that patients with pSS without cardiac symptoms would have myocardial abnormalities, and these would be independently associated with higher salivary gland focus scores (FS). Using contrast cMRI, we evaluated T2-weighted imaging (T2WI), allowing the imaging of myocardial edema (myocarditis), and LGE imaging, allowing the imaging of fibrosis9,10. Because disease activity is associated with morphological changes of the left ventricle in patients with RA, we speculated that classification and evaluation of the left ventricle based on morphological changes in left ventricular (LV) geometry would confirm the prognosis of myocardial fibrosis in patients with pSS11.
Therefore, we evaluated myocardial fibrosis in patients with pSS without cardiac symptoms using cMRI and examined the relationship between disease characteristics and myocardial fibrosis in patients with pSS.
METHODS
Patients and recruitment. This was a cross-sectional study of patients with pSS registered in our hospital between January 2014 and April 2017. There were very few male patients with pSS on entry, and most had CVD risk factors. As a result, only women were admitted in this study. Female patients with pSS without cardiac symptoms who met either the 2002 revised American-European Consensus Group classification criteria or the 2012 American College of Rheumatology classification criteria for case selection in clinical studies were enrolled12,13. We excluded patients with a history or diagnosis of myocardial infarction, HF, or angioplasty. Current or past smokers, patients with a history of diabetes mellitus (glycated hemoglobin > 6.1%), hypertension (> 140/90 mmHg), dyslipidemia [low-density lipoprotein (LDL) cholesterol > 140 mg/dL by the Friedewald equation, high-density lipoprotein (HDL) cholesterol < 40 mg/dL, triglycerides > 150 mg/dL], or bronchoconstriction, and those with claustrophobia or contrast media allergy were also excluded due to the difficulty in obtaining an MRI scan. This study was approved by the local ethics committee of Nihon University Itabashi Hospital, Japan (research number: RK-160112-07). Informed consent was obtained from all patients in accordance with the 1975 Declaration of Helsinki (as revised in Brazil 2013).
MRI acquisition and analysis. All patients underwent cine MRI, T2WI, and LGE examinations within 1 week after clinical examination. A 3.0T scanner (Achieva, Philips Healthcare) was used for MRI. A dose of 0.1 mmol/kg gadolinium diethylenetriamine pentaacetic acid (Magnevist, Schering AG) was used as the contrast agent. Regions indicated by LGE and T2WI were examined. All MR images were interpreted separately by 2 radiologists blinded to clinical information, and discordant interpretations were resolved by consensus.
LV function [ejection fraction (EF), %], end-systolic volume (ESV; mL), end-diastolic volume (EDV; mL), stroke volume (SV; mL), cardiac output (CO; L), LV mass (LVM; g), and LVM index (LVMI; i.e., LVM divided by the body surface area) were measured from cine MRI images. Based on the results of Kobayashi, et al, the figures for elevated LVMI and LVM/EDV (66.6 g/m2 and 1.02 g/mL, respectively) were defined by measuring these figures in healthy volunteers and computing the mean + 2 SD of each measure14. LV geometry was classified using the reference values as follows: (1) concentric remodeling (LVMI < 66.6 g/m2, LVM/EDV ≥ 1.02 g/mL); (2) concentric hypertrophy (LVMI ≥ 66.6 g/m2, LVM/EDV ≥ 1.02 g/mL); (3) eccentric hypertrophy (LVMI ≥ 66.6 g/m2, LVM/EDV < 1.02 g/mL); and (4) normal geometry (LVMI < 66.6 g/m2, LVM/EDV < 1.02 g/mL). Data from Kobayashi, et al14 were considered the control group because their data were from the same MRI facility as the current study.
Clinical assessments and pathological examination of SS. Disease activity in all patients was evaluated by the same observer using the European League Against Rheumatism Sjögren’s Syndrome Disease Activity Index (ESSDAI)15. The presence or absence of Raynaud phenomenon (RP) was determined using the international consensus classification criteria published in 201416. We also used medical records as a reference. Regarding the histological evaluation of labial gland biopsy with H&E staining, salivary gland FS was defined as the mean number of lymphocytic foci containing > 50 lymphocytes per 4 mm2 of periductal or perivascular tissue17. Additionally, the lymphocytic foci had to exist in close proximity to normal acinar cells. Histopathological analyses were performed by experienced pathologists and rheumatologists.
Laboratory assessments. Fasting serum and plasma samples were centrifuged and stored at –80°C. All assays were performed in our institute in accordance with our internal quality control procedures. Patients underwent measurement of total cholesterol, triglyceride, HDL cholesterol, LDL cholesterol, and fasting blood glucose concentration for the objective assessment of traditional atherosclerotic disease risk factors at the time of visit. We used typical variables required for pSS diagnosis (e.g., rheumatoid factor, anti-Ro/SSA antibodies, and anti-La/SSB antibodies). We measured anti-Ro/SSA and anti-La/SSB antibodies using a commercial ELISA kit based on purified antigens (Orgentec). Further, we separately measured anti-Ro52 and anti-Ro60 antibodies, subtypes of anti-Ro/SSA antibodies, using BioPlex 2200 ANA Screen (Bio-Rad Laboratories). The N-terminal pro B-type natriuretic peptide (NT-proBNP) level was measured with a Cobas 8000 e602 device (Roche Diagnostics), using a lower detection limit of 5 pg/mL and variation coefficients of 1.6% at 71.39 pg/mL and 1.8% at 103.4 pg/mL.
Statistical analysis. All continuous variables were considered non-normally distributed due to the small sample size. In groups categorized by the presence of delayed enhancement, medians and IQR were calculated for continuous variables and compared using the Wilcoxon rank-sum test. For categorical variables, counts and proportions were compared using Fisher exact test. To determine independent pSS characteristics for myocardial fibrosis detected by cMRI, we developed a multivariable logistic regression model. We first selected several pSS characteristics (i.e., explanatory variables) with reference to clinical significance, median difference between the LGE-positive and LGE-negative groups, and P values. In the multivariable analysis model 1, variables identified as significant in univariate logistic regression analysis (P < 0.05) were fed using the forced entry method. In model 2, variables identified as significant in univariate logistic regression analysis were fed into the model using the likelihood ratio. The cutoff values and the positive and negative predictive values of FS were calculated using the receiver-operating characteristic (ROC) curve for LGE detection. All statistical analyses were executed using JMP 14.0 software (SAS Institute Inc.). P < 0.05 was accepted as statistically significant.
RESULTS
Disease characteristics of patients with pSS. Fifty-two women with pSS (median age 55, IQR 47–65.7 yrs) were included in this study (Table 1). Majority had dry mouth and eye symptoms, but only 21% were diagnosed with RP. Forty-eight (92%) of 52 patients were anti-Ro/SSA antibody–positive [anti-Ro52 antibodies were observed in 21 (75%) of 28 patients; anti-Ro60 antibodies were observed in 25 (89%) of 28 patients], whereas 20 (38%) of 52 patients were anti-La/SSB antibody–positive.
Patient characteristics according to myocardial LGE status.
Salivary gland FS. Forty-four patients (85%) underwent labial gland biopsy. Majority had 0 ≤ FS < 3, but only 16% reported 3 ≤ FS < 6. No patient had FS ≥ 6.
ESSDAI. The median of total ESSDAI score was 4 (IQR 0–8). No patient had high disease activity in any domain. Most patients (56%) had a low ESSDAI, while only 7 (13%) had high disease activity based on the ESSDAI (data not shown).
Myocardial abnormalities in cMRI. cMRI revealed myocardial abnormalities in 11 patients (21%). Ten patients (19.2%) were LGE-positive, two (2/10 = 20%) of whom showed high intensity on T2WI. Three patients (5.8%) showed high intensity on T2WI. Of the 10 LGE-positive patients, 9 showed a linear enhancement pattern, whereas only 1 showed a patchy enhancement pattern. Five patients had LGE in the myocardium and 5 had LGE in the epicardium; none had LGE in the endocardium. T2WI images with patchy enhancement at the same site as LGE, and LGE images with linear enhancement are shown in Figure 1.

Images of LGE and T2WI. (A) LGE and T2WI showed patchy enhancement in the myocardium of the mid inferoseptal wall (arrows). (B) Observed curvilinear LGE images in the epicardium of the basal anteroseptal and inferoseptal walls (arrows). (C) Observed curvilinear LGE images in the myocardium of the basal inferolateral wall (arrows). (D) Two linear LGE images observed separately in the myocardium of the septum (arrows). LGE: late gadolinium enhancement; T2WI: T2-weighted imaging.
Association of LGE with pSS characteristics. Univariate analysis showed significant differences in RP and FS between the LGE-positive and LGE-negative groups (P = 0.003 and P = 0.009, respectively; Table 1). NT-pro BNP levels and the proportion of T2WI-positive patients were higher (but not significantly so) in the LGE-positive group than in the LGE-negative group (P = 0.08 and P = 0.09, respectively). The median NT-proBNP level in patients with pSS with LGE was more than twice as high as in those without LGE. There were no significant differences between the 2 groups with respect to other pSS characteristics (e.g., age, duration of the illness, anti-Ro/SSA antibodies, anti-La/SSB antibodies, and total ESSDAI score). Of traditional CVD risk factors, total cholesterol was higher in those with LGE, but this finding did not reach statistical significance in univariate analysis (P = 0.13).
Comparison of LV structure between LGE-positive and LGE-negative groups. There were no significant differences between the LGE-positive and LGE-negative groups in EF, ESV, EDV, SV, and CO. LVMI and LVM/EDV were higher, but not significantly, in the LGE-positive group than in the LGE-negative group (P = 0.08 and P = 0.09, respectively).
Regarding the results of LV geometry in 52 patients, 44 (84.6%) had normal LV geometry, 3 (5.8%) had concentric remodeling, and 5 (9.6%) had eccentric hypertrophy, whereas no patient had concentric hypertrophy (data not shown).
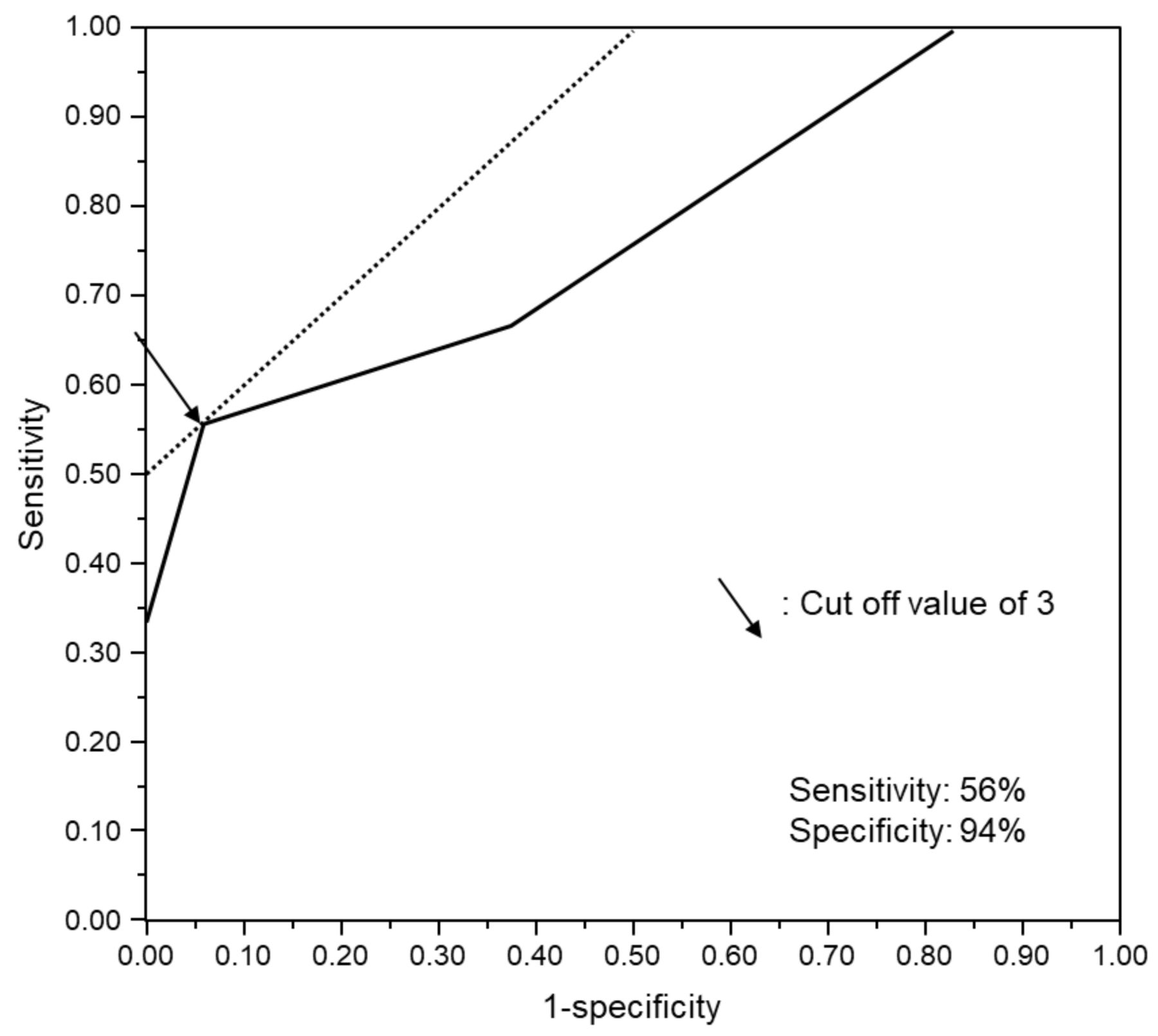
Multivariable analysis. FS was converted into binary data (FS ≥ 3 or < 3) using a cutoff value (FS = 3) with maximum sensitivity and specificity for identifying LGE-positive patients. Thereafter, it was used as a pSS characteristic in multivariable analysis with the ROC curve (Figure 2) described below.
{kind=link}
{kind=link}
ROC curve for the detection of LGE. ROC analysis demonstrated that salivary gland FS reliably detected LGE (AUC 0.77). Using a cutoff value of 3 and defining patients with pSS as those with conventional cMRI findings, the sensitivity and specificity FS in the detection of LGE were > 56% and > 94%, respectively. AUC: area under the curve; cMRI: cardiac magnetic resonance imaging; FS: focus score; LGE: late gadolinium enhancement; pSS: primary Sjögren syndrome; ROC: receiver-operating characteristic.
The 5 selected variables (FS ≥ 3, diagnosed RP, T2WI-positive, NT-proBNP, and LVMI) were all used in univariate logistic regression analysis (Table 2). When 3 variables identified as significant in univariate analysis were fed into the multivariable model 1 using the forced entry method, only FS ≥ 3 was extracted as an independent pSS characteristic related to positive LGE, even after adjustment (OR 11.21, 95% CI 1.18–106.80, P = 0.04). When 3 variables identified as significant in the univariate analysis were fed into the multivariable analysis model 2 using the forward selection method (likelihood ratio), as with model 1, only FS ≥ 3 was identified as an independent pSS characteristic related to positive LGE even after adjustment (OR 20.63, 95% CI 2.96–143.61, P = 0.002).
Logistic regression analysis of LGE.
ROC analysis for LGE detection. The ROC curve revealed a cutoff value with high levels of sensitivity and specificity for identifying LGE-positive patients with FS = 3 (area under the curve 0.77). When ≥ 3 was used as the cutoff value for labial gland biopsy (i.e., FS), the sensitivity, specificity, and positive and negative predictive LGE were 56%, 94%, 71%, and 89%, respectively.
Predictive accuracy of LGE detection. We investigated the accuracy of a FS-based classifier of LGE, namely, FS ≥ 3 and < 3, corresponding to LGE-positive and LGE-negative (the true condition), respectively (Table 3). Out of 44 predictive accuracy indicators, 38 were correct. The predictive accuracy indicators were as follows: accuracy, 86.4%; precision, 71.4%; recall, 55.6%; and F-measure (i.e., the harmonic mean of precision and recall), 0.63.
Predictive accuracy of salivary gland FS based on LGE status data.
DISCUSSION
We used cMRI to assess myocardial abnormalities in patients with pSS without cardiac symptoms. To the best of our knowledge, this is the first cMRI study with the largest number of patients with pSS. First, a higher prevalence than that expected of LGE was found in patients with pSS without cardiac symptoms. Second, positive LGE was independently associated with salivary gland FS ≥ 3.
In a metaanalysis by Beltai, et al, the OR of HF in patients with pSS was 2.54 compared with the control group3. However, that study had a limitation in that CVD risk factors were fed into the model for the pSS and control groups regardless of the presence or absence of such factors. Although ours was a cross-sectional study, we considered the effects of pSS on myocardial abnormalities by excluding patients with CVD risk factors.
A high prevalence of myocardial fibrosis was observed in the patients with pSS who underwent cMRI in our study. Unfortunately, there are no cMRI studies on a relatively large number of patients with pSS. Compared with our previous cMRI studies of patients with autoimmune diseases7,8, in which 19 (32%) of 60 patients with RA and 3 (33%) of 9 patients with SSc were LGE-positive, the prevalence of LGE in patients with pSS in the current study is somewhat lower. In our current study, we did not compare the rate of cMRI-detected myocardial fibrosis between patients with pSS and controls. However, in a cohort study of 1328 women (mean age 54, SD 8 yrs) with a low risk of CVD, only 9 (0.68%) were LGE-positive18. The mean age of the 52 female patients in this study was 53 years (SD 10). Therefore, the rate of cMRI-detected myocardial fibrosis in patients with pSS was substantially higher than in the previous study.
Our study showed an independent association between positive LGE and salivary gland FS ≥ 3. Although there are many reports showing cell infiltration into various organs (e.g., kidney, skin, and lung)19,20,21,22, only 1 case report directly identified the pathogenesis of myocarditis in patients with pSS from endomyocardial biopsy. A 35-year-old woman with pSS, who had a labial gland biopsy with a result of FS ≥ 1 and symptoms of HF, underwent catheterization and endomyocardial biopsy, which detected myocardial infiltration of lymphocytes and fibrotic changes due to pSS itself in the endomyocardium and interstitium23. It has also been reported that lymphocytic infiltration into and destruction of the exocrine glands lead to chronic activation of lymphocytes and the consequent lymphocytic infiltration into other organs24. In addition to the contents of these papers, given that FS ≥ 3 and LGE were shown to be related in this study, lymphocytic infiltration into the myocardium is conceivable as a pathological condition of pSS myocardial fibrosis. However, it is not an established view because lymphocytic infiltration is not always present in the region where there is a contrast effect in LGE, and lymphocytic infiltration into the myocardium of individual patients has not been confirmed histologically. The results of this study clearly show that the stronger the extent of lymphocytic infiltration into the small salivary glands, the higher the possibility of development of myocardial fibrosis.
Imaging characteristics alone cannot easily and accurately describe the various myocardial fibrosis observed in patients with different rheumatic diseases with regard to identifying disease characteristics and differences across these conditions. However, our study describes some unique, disease-specific factors as well as previous reports, such as a significant association between myocardial fibrosis and cytokine-mediated inflammation in patients with RA and a significant association between myocardial fibrosis and vasculopathy (i.e., digital ulcer) in patients with SSc7,8,14. In this study, we suggest a significant association between myocardial fibrosis and the degree of lymphocytic infiltration into the minor salivary glands as a unique predictor of pSS. Kakugawa, et al reported a significant association between FS ≥ 4 and the presence of pulmonary lesions (airway lesions and interstitial pneumonia) in patients with pSS using multivariable analysis25; to our knowledge, the only reports showing significant associations between the presence of extraglandular complications and higher FS were theirs and ours.
A prospective cohort study included 1726 patients with SS26 and evaluated the SS characteristics associated with FS ≥ 1. All SS characteristics independently associated with FS ≥ 1 in multivariate analysis were related to the presence of glandular symptoms or immunological abnormalities. FS ≥ 3 and FS ≥ 4 were significantly associated with the presence of extraglandular complications in studies performed by us and by Kakugawa, et al25. These results suggest that the greater the degree of lymphocytic infiltration into the labial gland, the more likely extraglandular symptoms will develop.
The positive and negative predictive values of LGE with FS ≥ 3 (positive) and FS < 3 (negative) were 71% and 89%, respectively, indicating that FS ≥ 3 acts as a good predictor of positive LGE. cMRI is an established instrument for the early diagnosis of myocardial fibrosis. Labial gland biopsy is included in the classification criteria and is an almost mandatory examination for patients with pSS. The demonstrated ability to predict myocardial fibrosis adds to the usefulness of salivary gland FS. However, it is still evident that salivary gland FS cannot replace cMRI as a test that can detect asymptomatic myocardial fibrosis. cMRI could be a tool for detecting asymptomatic myocardial fibrosis in patients with pSS with a higher salivary gland FS. Further accumulation of data in this field is warranted.
Although some studies in Western countries have evaluated LV function and structure using MRI, the data are not consistent because of the diversity among hospitals. Only 1 previous study evaluated LV function and structure in healthy Japanese individuals between 50 and 69 years of age with no known arteriosclerosis14. This study also evaluated morphological changes in LVMI and LVM/EDV as cMRI variables. No previous cMRI studies examined the presence or absence of morphological changes in patients with pSS and classified LV geometry. The current study showed a trend toward positive associations of LGE with higher LVMI and LVM/EDV, in line with a previously published report27. These results may suggest that such remodeling occurs in patients with pSS and that myocardial fibrosis may be involved in the background.
Although there was no independent association between RP and LGE, RP changed the association of FS ≥ 3 with LGE so dramatically in the model. In the field of rheumatic disease, the main cause of cardiac complications in SSc, as in RP, is reported to be the vasospasm of small blood vessels28.
The clinical effect of our findings is the suggestion that cardiac complications could be considered extraglandular complications of pSS. Further, they raise the possibility that individuals with pSS might benefit from CV screening to identify early myocardial disease at a stage when early intervention would improve prognosis, particularly among patients with higher salivary gland FS3.
This study has some limitations. First, while this was the largest cMRI study in patients with pSS, to our knowledge, the sample size was too small to achieve statistical power or provide a strong conclusion. Second, this study did not evaluate long-term prognosis. Therefore, future follow-up studies are required. Third, only patients with pSS with a low risk of CVD were included in this study. Also, we did not enroll male patients or patients with secondary SS. Fourth, this study did not perform quantitative evaluation of LGE. Currently, it is possible to perform quantitative evaluation using T1 mapping and extracellular volume analysis along with LGE. It has been reported that quantitative evaluation allows detailed evaluation of myocardial characteristics in early stages that is impossible in the evaluation of salivary gland FS29,30,31. Fifth, ischemic heart disease may have been missed as we did not perform cardiac catheterization. Nevertheless, as the orientation of coronary arteries did not match with those observed in the LGE images, ischemia can be ruled out as the cause of high-signal areas in LGE images.
In conclusion, the results of this cMRI study demonstrated a high prevalence of myocardial fibrosis in patients with pSS without cardiac symptoms. We will continue to examine whether extraglandular complications of pSS include cardiac complications.
ACKNOWLEDGMENT
We would like to express our sincere gratitude to all members and staff of the Division of Hematology and Rheumatology, Nihon University School of Medicine. We would also like to express our sincere gratitude to Dr. Jon T. Giles (Division of Rheumatology, Columbia University, College of Physicians and Surgeons, New York, USA) for the helpful discussion and comments on the manuscript.
Footnotes
All authors attest that they have no financial conflicts of interest pertaining to this investigation.
- Accepted for publication August 24, 2020.
- Copyright © 2021 by the Journal of Rheumatology
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.