
Abstract
Objective Therapeutic response was evaluated among new apremilast, methotrexate (MTX), or biologic disease-modifying antirheumatic drug (bDMARD) initiators with oligoarticular psoriatic arthritis (PsA).
Methods Patients with oligoarticular PsA in the Corrona PsA/Spondyloarthritis Registry initiating treatment with apremilast, MTX, or bDMARD, and completing 6-month follow-up were included.
Results In total, 150 patients initiated monotherapy (apremilast: n = 34; MTX: n = 15; bDMARD: n = 101). Apremilast initiators had higher baseline disease activity than MTX initiators. At follow-up, apremilast initiators experienced numerically greater disease activity improvements than MTX initiators and similar improvements to bDMARD initiators.
Conclusion Findings suggest apremilast monotherapy is an effective option for patients with oligoarticular PsA.
- arthritis
- methotrexate
- psoriatic arthritis
- TNF receptors
Oligoarticular psoriatic arthritis (PsA), defined as < 5 involved joints1,2, affects ≈50% of patients with PsA3. Typical randomized controlled trials have not focused on this population, and on average, patients enrolled have swollen and tender joint counts of 12 and 21, respectively4. Despite the high prevalence of oligoarticular PsA, data are lacking in this population, and recommendations for management remain largely unaddressed4,5,6.
Our study assessed baseline clinical characteristics of patients with oligoarticular PsA (≤ 4 swollen joints) to determine the effect of apremilast or methotrexate (MTX) treatment on disease activity. Patients initiating biologic disease-modifying antirheumatic drug (bDMARD) monotherapy were examined as a point of reference.
MATERIALS AND METHODS
Study design. A cohort study was performed in the Corrona Psoriatic Arthritis/Spondyloarthritis (PsA/SpA) Registry, a multicenter registry that recruited patients among > 50 participating rheumatologists in the United States7. Adults (aged ≥ 18 yrs) were included if they had PsA and oligoarthritis (defined as ≤ 4 swollen joints); were enrolled in the Corrona PsA/SpA Registry; initiated apremilast, MTX, or bDMARD monotherapy as the first initiation within the registry between June 1, 2014, and March 1, 2018; and had a 6-month follow-up visit with a time window of 3 to 9 months within the same period. Patients were defined as having polyarticular or oligoarticular PsA at the time of therapy initiation. Patients defined as having oligoarticular PsA may have had polyarticular disease previously, as they may have had changing numbers of joints involved with therapy selection based on patient characteristics.
Outcomes. Outcomes at 6 months included assessments of disease activity and patient-reported outcome (PRO) measures. Included were the proportion of patients with > 1 swollen joint or > 1 tender joint at baseline achieving a swollen joint count (SJC) of 0 or 1 or a tender joint count (TJC) of 0 or 1, respectively; change from baseline in SJC and TJC; and change from baseline in the Clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) score and the cDAPSA core components.
The cDAPSA score was calculated as SJC (0–66) plus TJC (0–68) plus the patient global assessment of disease activity‒arthritis and psoriasis (PtGA-PsO) visual analog scale (VAS) score (0–10 cm) plus the overall pain VAS (0–10 cm) score. Additional PRO measures included the change from baseline in fatigue VAS (0–100 mm) score, proportion of patients achieving the minimal clinically important difference (MCID; ≥ 0.35-point decrease) in the Health Assessment Questionnaire–Disability Index (HAQ-DI) score, change from baseline in PtGA-arthritis (PtGA-PsA) VAS score (0–100 mm), and the proportion of patients without physician-reported clinical characteristics of nail psoriasis at 6 months.
Statistical analysis. Descriptive statistics were calculated for patient demographic, clinical, and treatment characteristics at the index visit and outcomes at the 6-month follow-up visit. The index visit was defined as the visit in which patients reported treatment initiation with apremilast, MTX, or bDMARD. All data were analyzed descriptively using means and SD for continuous variables and presented as counts and percentages of patients for categorical variables.
Ethical conduct. All participating investigators were required to obtain full board approval for conducting research involving human subjects. Sponsor approval and continuing review was obtained through a central investigational review board (New England Independent Review Board, NEIRB No. 120160610); there were > 50 study sites. For academic investigative sites that did not receive a waiver to use the central investigational review board, full board approval was obtained from the respective governing investigational review boards and documentation of approval was submitted to the sponsor before initiating any study procedures. All registry patients were required to provide written informed consent before participating.
RESULTS
Index visit: patient demographics and clinical characteristics. A total of 1593 patients with oligoarticular PsA were listed in the Corrona PsA/SpA Registry between June 2014 and March 2018. Of these patients, 150 had initiated monotherapy with apremilast (n = 34), MTX (n = 15), or bDMARD (n = 101) as the first initiation during follow-up for oligoarticular PsA (Supplementary Figure 1, available with the online version of this article). Patient demographic, clinical, and treatment characteristics at the index visit are presented in Table 1. Patients who initiated MTX monotherapy were slightly older and a higher proportion were female compared with patients in the apremilast and bDMARD monotherapy groups. More than half of patients in all 3 monotherapy groups were obese. Mean disease duration was generally similar among monotherapy groups.
Baseline patient characteristics.
Overall, treatment and clinical characteristics of apremilast initiators were suggestive of more refractory oligoarticular PsA compared with MTX initiators (Table 1). Among apremilast and MTX initiators, 79% and 20% received ≥ 1 prior bDMARD, respectively. Patients who initiated apremilast had higher levels of disease activity at baseline, measured by a cDAPSA score > 13 (moderate or high disease activity), and fewer had minimal disease activity (MDA) at baseline compared with patients who initiated MTX or bDMARD. Patients initiating apremilast monotherapy also reported numerically higher mean scores of PRO measures at baseline, including PtGA-PsA and fatigue VAS scores; likewise, the proportion of patients with a HAQ-DI score > 0.5 was also higher with apremilast monotherapy.
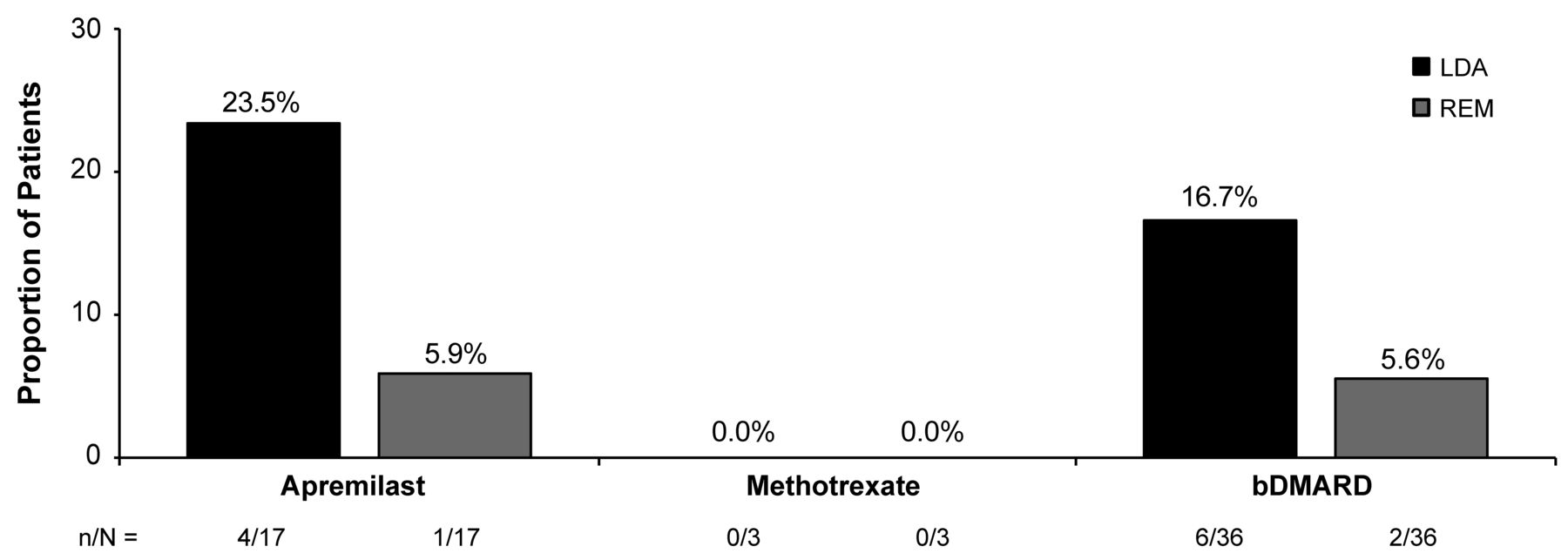
Disease activity assessments. A numerically greater proportion of patients with an SJC > 1 or TJC > 1 at baseline who received apremilast monotherapy achieved an SJC ≤ 1 or TJC ≤ 1 at 6 months than those who received monotherapy with MTX or bDMARD (Figure 1). Achievement of an SJC ≤ 1 or TJC ≤ 1 in the apremilast monotherapy group was more similar to the bDMARD monotherapy group than to the MTX monotherapy group (Figure 1). Mean changes in SJC and TJC, respectively, from baseline were numerically greater with apremilast monotherapy (−0.4 and −0.4) compared with MTX (0.1 and −0.3) or bDMARD (0.2 and −0.1) monotherapy. A numerically greater proportion of apremilast monotherapy initiators who were in a moderate or high disease activity cDAPSA category at baseline achieved low disease activity (LDA) or remission (REM) at 6 months compared with MTX and bDMARD monotherapy initiators (Figure 2). Achievement of LDA or REM in the apremilast monotherapy initiators was more comparable to bDMARD monotherapy initiators than to MTX monotherapy initiators (Figure 2). Of those patients who did not have MDA at initiation, 8.7% (2/23) in the apremilast monotherapy group, 0% (0/7) in the MTX group, and 17.9% (10/56) in the bDMARD monotherapy group achieved MDA at the 6-month visit. None of the patients receiving apremilast monotherapy or MTX who did not have very LDA (VLDA) at initiation achieved VLDA at the 6-month visit; 4.8% (4/84) initiating bDMARD monotherapy achieved VLDA. The mean improvement from baseline in cDAPSA score was numerically greater in patients receiving apremilast monotherapy (−1.5) compared with those receiving MTX (−0.2) or bDMARD (−0.1) monotherapy.

The proportions of patients with > 1 swollen joint or > 1 tender joint at baseline achieving (A) swollen joint count (SJC) ≤1 and (B) tender joint count (TJC) ≤1 at 6 months. bDMARD: biologic disease-modifying antirheumatic drug; n/N: number of responders/patients with sufficient data for evaluation.
{kind=link}
{kind=link}
Achievement of low disease activity (LDA)/remission (REM). Proportions of patients in moderate or high Clinical Disease Activity Index for Psoriatic Arthritis (cDAPSA) categories at baseline achieving cDAPSA LDA or REM categories at 6 months. bDMARD: biologic disease-modifying antirheumatic drug; n/N: number of responders/patients with sufficient data for evaluation.
PRO measures. At 6 months, patients in all 3 monotherapy groups experienced minimal changes from baseline in mean PtGA-PsA VAS, overall pain VAS, fatigue VAS, and PtGA-PsO VAS scores. Changes from baseline in the apremilast, MTX, and bDMARD monotherapy groups were −0.2, 2.5, and 0.4 for mean PtGA-PsA VAS scores; 0.2, −0.1, and 0.1 for overall pain VAS scores; −1.4, 0.3, and −0.3 for mean fatigue VAS scores; and −2.3, 1.7, and −2.0 for PtGA-PsO VAS scores, respectively. The proportions of patients achieving at least a 0.35-point improvement in HAQ-DI MCID were similar in the apremilast, MTX, and bDMARD monotherapy groups (Supplementary Figure 2, available with the online version of this article). A numerically greater proportion of patients with physician-reported nail psoriasis at baseline were without physician-reported nail psoriasis at 6 months in the apremilast monotherapy group compared with the MTX and bDMARD monotherapy groups (Supplementary Figure 3). Improvement in nail psoriasis in the apremilast monotherapy group was more similar to the bDMARD monotherapy group than to the MTX monotherapy group (Supplementary Figure 3).
DISCUSSION
Although oligoarticular PsA, by definition, involves fewer joints than polyarticular PsA, the 2 subgroups had comparable disease burden8,9,10. Oligoarticular PsA, while common11,12,13,14,15,16, remains understudied and identification of effective management of this PsA phenotype is warranted. Despite use in a more often treatment-refractory patient population, the apremilast monotherapy group experienced improvements in disease activity and PRO measures; improvements were also experienced in the MTX group. The improvements observed with apremilast monotherapy in this population were comparable with bDMARD monotherapy. Our comparison of the 3 groups was descriptive, without statistical testing, because we cannot fully address confounding by indication when comparing different therapy classes across different lines of therapy. Of note, in many cases, patients included in this study were receiving apremilast shortly after its approval. As is generally observed, due to physician comfort with a new medication and payer preference, new-to-market therapies are often used in a more recalcitrant patient population. Over time, apremilast has been more commonly used earlier in the disease course17. A limitation of this study is the small sample size and therefore statistical testing was not performed. Further, only patients who completed the 6-month follow-up visit were analyzed, which can introduce selection bias. A larger phase IV, multicenter, randomized, double-blind, placebo-controlled, parallel-group study (ClinicalTrials.gov: NCT03747939) is currently assessing the efficacy of apremilast in patients with early oligoarticular PsA despite initial stable treatment with either nonsteroidal anti-inflammatory drugs and/or 1 conventional synthetic DMARD. Overall, findings from this exploratory analysis suggest that apremilast monotherapy is an effective treatment option for oligoarticular PsA.
ACKNOWLEDGMENT
Writing support was funded by Celgene Corporation and provided by Kristin Carlin, RPh, MBA, of Peloton Advantage, LLC, an OPEN Health company. The authors, however, directed and are fully responsible for all content and editorial decisions for this report.
Footnotes
All authors contributed to the interpretation of the results.
Full Release Article. For details see Reprints and Permissions at jrheum.org.
This study was sponsored by Corrona, LLC, and the analysis was funded by Celgene Corporation. Amgen acquired the worldwide rights to Otezla (apremilast) on November 21, 2019. Access to study data was limited to Corrona, and Corrona statisticians completed all of the analysis.
AO has received grant/research support from Pfizer Inc. and Novartis and has served as a consultant to AbbVie, Amgen, Bristol Myers Squibb, Celgene Corporation, Corrona, Eli Lilly and Company, Novartis, Pfizer Inc., and Takeda. ML, MG, and KE have worked on Corrona-contracted subscriptions for AbbVie, Amgen, Bristol Myers Squibb, Boehringer Ingelheim, Celgene Corporation, Crescendo, Eli Lilly and Company, Genentech, Gilead, GSK, Janssen, Momenta Pharmaceuticals, Novartis, Pfizer Inc., Regeneron, Roche, Merck, UCB, and Valeant. LRH is an employee and shareholder of Corrona, LLC, received grants from Pfizer Inc., and has served as a consultant to AbbVie, Bristol Myers Squibb and Roche. SR and BG are employees of Amgen Inc. and were employees of Celgene Corporation at the time of study conduct. PJM has received grant/research support from and served as a consultant for Abbott, Amgen, Biogen Idec, Bristol Myers Squibb, Celgene Corporation, Eli Lilly and Company, Genentech, Janssen, Novartis, Pfizer Inc., Roche, and UCB, and has served on the speakers bureau for Abbott, Amgen, Biogen Idec, Bristol Myers Squibb, Eli Lilly and Company, Genentech, Janssen, Pfizer Inc., and UCB. Corrona has been supported through contracted subscriptions in the last 2 years by AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene Corporation, Crescendo, Eli Lilly and Company, Genentech, Gilead, GSK, Janssen, Merck, Momenta Pharmaceuticals, Novartis, Ortho Dermatologics, Pfizer Inc., Regeneron, Roche, Sanofi, Sun, and UCB.
- Accepted for publication October 23, 2020.
- Copyright © 2021 by the Journal of Rheumatology
Free online via JRheum Full Release option
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
DATA SHARING
The Corrona dataset is based on a large US multicenter study adhering to a number of institutional review boards, with complex logistics. Patients did not provide consent to raw data sharing during the data collection for this purpose, and the Corrona data sharing policies do not permit raw data sharing for this purpose. An aggregated limited dataset from the current analyses is available to qualified investigators with an approved protocol. Data requests may be sent to Corrona, represented by Dr. Jeffrey Greenberg; email: jgreenberg{at}corrona.org.