
Abstract
Objective. To investigate expression of terminal complement components C3a and C5a on circulating myeloperoxidase (MPO)-positive microparticles (MPO+MP) in relation to disease activity and renal involvement in patients with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV).
Methods. Forty-six clinically well-characterized patients with AAV and 23 age- and sex-matched healthy controls were included. The concentration of MPO+MP expressing C3a and C5a was analyzed from citrate plasma by flow cytometry. Serum levels of C3a and C5a were determined using commercial ELISA. The assessment of vasculitis disease activity was performed using the Birmingham Vasculitis Activity Score (BVAS). Among patients, 23 had active disease with BVAS ≥ 2 and 14 patients had active renal flares.
Results. AAV patients had significantly increased expression of C3a and C5a on MPO+MP compared to controls (both p < 0.0001). When the group of patients with active AAV was divided according to the presence of renal activity, the concentration of MPO+MP expressing C3a and C5a was significantly higher in patients with renal involvement compared to patients with nonrenal disease and controls (p < 0.05 and p < 0.01, respectively). The serum levels of C3a were significantly decreased (p < 0.01) in the renal subgroup, while there were no changes in serum levels of C5a comparing the renal and nonrenal groups. There was significant correlation between the disease activity measured by BVAS and the levels of C3a and C5a expressed on MPO+MP.
Conclusion. Determination of C3a and C5a on MPO+MP might be considered as a novel biomarker of renal involvement in patients with AAV and may be of importance in the pathogenetic process.
- ANTINEUTROPHIL CYTOPLASMIC ANTIBODY-ASSOCIATED VASCULITIS
- COMPLEMENT
- MICROPARTICLES
Antineutrophil cytoplasmic antibody (ANCA)–associated vasculitis (AAV) is a heterogeneous group of multisystem disorders characterized by pauciimmune necrotizing vasculitis, affecting small- to medium-sized blood vessels, together with neutrophil- or eosinophil-enriched granulomatous inflammation. It comprises 3 distinct systemic subsets, including microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA; formerly known as Wegener granulomatosis), and eosinophilic GPA (previously Churg-Strauss syndrome)1.
Although AAV is generally considered a pauciimmune disease, there is a growing body of experimental and clinical observations indicating that complement activation is critical in the development of ANCA-mediated disease2,3,4. In vitro studies could demonstrate that complement activation, especially through the alternative pathway, acts as positive feedback amplification of neutrophil activation, resulting in the aggressive necrotizing inflammation in AAV5. Additionally, the levels of complement activation fragments (Bb, C3a, C5a, and soluble C5b-9) have been shown to be elevated in the plasma and urine of patients with active disease6. Although C3 deposits are less prominent in the glomeruli of patients with AAV than in the glomeruli of patients with immune complex diseases, C3d deposits are detected in a high percentage of patients7,8 and have been shown to correlate with poor outcome7,8. The crucial evidence of the involvement of complement in AAV pathogenesis is the engagement of C5a receptors (CD88) on neutrophils, suggesting that blockade of this receptor might have therapeutic efficacy in patients with AAV, as shown in a recent phase II clinical trial9.
C3a and C5a are ∼10 kDa peptides that exhibit delicate biological effects by interactions with their widely expressed high-specific receptors C3aR, C5aR1 (CD88), and C5aR2 (C5L2 or GPR77)10. The C5a molecule is primarily proinflammatory, including leukocyte chemotaxis, neutrophil degranulation, histamine release by basophils and mast cells, and oxidative bursts on macrophages11, but is also prothrombotic, inducing tissue factor expression12. In the vasculitis model, the interaction between C5a and the C5aR1 receptor creates an amplification loop that is a central contributing factor in ANCA-mediated neutrophil activation4. The role of C3a is more subtle, as reviewed by Coulthard and Woodruff13. In the acute setting, C3a seems to prevent mobilization of neutrophils and limits their accumulation into tissues, thereby reducing the inflammatory response at the tissue level. Yet in certain chronic disease models such as rheumatoid arthritis (RA), C3a clearly demonstrates proinflammatory activity and contributes to disease progression14. This dual role of C3a is exerted not only by interaction with C3aR but is reported to be dependent on the presence of C5aR2, suggesting that C5aR2 may contribute to C3a signaling through interactions with C3aR15. The role of C3a in AAV seems to be less pronounced regarding neutrophil activation4.
Microparticles (MP) are membrane-bound small vesicles, with diameters from 0.1 to 1 µm. When released from the cell membrane upon cell activation or during the apoptosis, MP act as biological effectors in inflammation, angiogenesis, endothelial injury, and thrombosis16. The property of carrying markers of the parental cell (MP contain membrane, cytoplasmic, and nuclear constituents characteristic of their precursor cell) enables detection of cellular origin, mainly platelets, but also red blood cells, leukocytes, or endothelial cells17. Moreover, MP are implicated in a variety of biological processes, such as intracellular communication and transport of surface proteins and thereby serve as markers of disease activity in a variety of pathological processes18. However, only a few studies have previously elucidated the role of MP in AAV19,20,21,22,23,24.
Considering the putative role of complement activation in the pathogenesis of AAV, the aim of our study was to evaluate expression of C3a and C5a on myeloperoxidase (MPO)-positive MP (MPO+MP) during active disease and remission, compared to healthy control subjects.
MATERIALS AND METHODS
A group of 46 ANCA-positive patients with AAV, either GPA or MPA, were included. These patients, recruited from the Departments of Nephrology and Rheumatology at Karolinska University Hospital, were diagnosed according to the validated algorithm for epidemiological studies of AAV25. The assessment of vasculitis disease activity was performed using the Birmingham Vasculitis Activity Score (BVAS, version 2003), according to the European League Against Rheumatism recommendations26. Patients with a BVAS of 0 were considered to be in remission. Renal involvement was defined as pathological changes on a recent renal biopsy (seen in 14 patients with active disease, renal biopsy performed in 13 cases) and/or by the presence of significant hematuria and/or elevated creatinine values (Table 1).
General features of patients and controls.
Control samples were obtained from 23 healthy age-/sex-matched subjects. The local ethics committee approved the study protocol (Dnr: 2008/1143-31) and informed consent for publication of study results was obtained from each subject.
Blood sampling
Peripheral venous blood was collected into Vacutainer tubes (Becton Dickinson) containing clot activator or trisodium citrate (0.129 mol/l, pH 7.4; 1 part trisodium citrate and 9 parts blood). Serum, specifically platelet-poor plasma, was obtained within 60 min of sampling by centrifugation at 2000 × g for 20 min at room temperature, then divided into aliquots and stored frozen at −70°C.
Detection of microparticles using flow cytometry
Platelet-poor plasma was thawed in a water bath at 37°C for about 5 min, followed by centrifugation of samples at 2000 g for 20 min at room temperature, to remove any cells or debris that may interfere with the analysis. The supernatant was centrifuged again at 13,000 g for 2 min at room temperature. Twenty ml of the supernatant were incubated in the dark for 20 min with 5 µl of monoclonal antibodies, anti–MPO-phycoerythrin (PE; Beckman Coulter) together with anti–C3a-FITC and anti–C5a-Dylite 755 (Thermo Fisher Scientific Inc.). After incubation, samples were fixed prior to analysis (Cellfix). Measurement of MP was performed by flow cytometry on a Beckman Gallios instrument (Beckman Coulter). The MP gate was determined using Megamix beads (0.3–1.0 μm, BioCytex). MPO+MP were defined as particles < 1 μm. Conjugate isotype-matched immunoglobulins with no reactivity against human antigens were used as negative controls. In the present study, results are shown as numbers of MPO+MP events measured in 30-s analysis. The intra- and interassay coefficients of variation (CV) for MPO+MP measurement were < 9%.
Serological markers
ANCA were detected by standard multiplex assay (BIO-RAD, BioPlex TM 2200) according to clinical routine at the Karolinska University Hospital.
Complement factor C3 in serum was analyzed according to clinical routine using turbidimetry at the Department of Immunology at the Karolinska University Hospital. The normal range was 0.77–1.62 g/l.
Detection of C3a
Serum levels of C3a were measured using MicroVue C3a Enzyme Immunoassay (Quidel Corp.). This is a 3-step procedure using (1) a microassay plate coated with a murine monoclonal antibody specific for a neo-epitope on human C3a, (2) a horseradish peroxidase (HRP)-conjugated polyclonal antibody to the C3a region of C3, and (3) a chromogenic substrate. The color intensity of the reaction mixture is proportional to the concentration of C3a present in the standards, controls, and diluted test specimens. Results are calculated from the generated standard curve using 4-parameter analysis and expressed as ng/ml. The interassay CV is 5.3% and intraassay CV is 8.3%.
Detection of C5a
Serum levels of C5a were measured using MicroVue C5a Enzyme Immunoassay (Quidel Corp.). This is a direct capture immunoassay for the measurement of C5a in human serum, plasma, and other biological or experimental samples. A 3-step procedure is performed using (1) a microassay plate coated with a murine monoclonal antibody specific for a neo-epitope on human C5a, (2) an HRP-conjugated murine monoclonal antibody to the C5a region of C5, and (3) a chromogenic substrate. The color intensity of the reaction mixture is proportional to the concentration of C5a present in the diluted test specimens, standards, and controls. Results are calculated from the generated standard curve using linear regression analysis and expressed as ng/ml. The interassay CV is 3.8% and intraassay CV is 7.8%.
Routine laboratory analyses were carried out using standard methods at the Karolinska University Hospital, including C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and plasma creatinine levels. The Cockcroft-Gault formula was used to estimate creatinine clearance (estimated glomerular filtration rate; eGFR)27.
Statistical analysis
Data were analyzed using GraphPad Prism, version 4 (GraphPad Software). Descriptive statistics were used for presentation of patient characteristics. For continuous variables, means and SD or medians with ranges were used, whereas categorical variables were presented as percentages. For comparison of more than 2 groups of individuals, 1-way ANOVA was used. A p value < 0.05 was regarded as statistically significant. Correlation between variables was examined using Pearson and Spearman correlation analysis, depending on data type and distribution.
RESULTS
General patient data
Detailed characteristics of the patients and controls, including age, sex, diagnosis, ANCA antibody type, disease activity score (BVAS), and renal function, are listed in Table 1. There was no difference between active and inactive patients regarding these characteristics, although creatinine levels were significantly increased and eGFR levels significantly decreased in both groups of patients with AAV compared to controls.
All patients with active disease had recent onset of disease prior to inclusion in the study. The median time from diagnosis to inclusion and blood sampling was 5 days (range 0–287 days). The patients with inactive disease had a median disease duration of 5.3 years (range 1.2–12 yrs).
Twenty-three patients had active disease defined as a BVAS > 0 (mean BVAS 14.0 ± 8.1; Table 1).
Table 2 demonstrates clinical and laboratory variables of patients with active and inactive AAV. Data regarding the treatment in respective groups of patients are also shown in Table 2.
Clinical manifestations and treatment of patients with AAV.
C3a- and C5a-positive neutrophil MP (NMP)
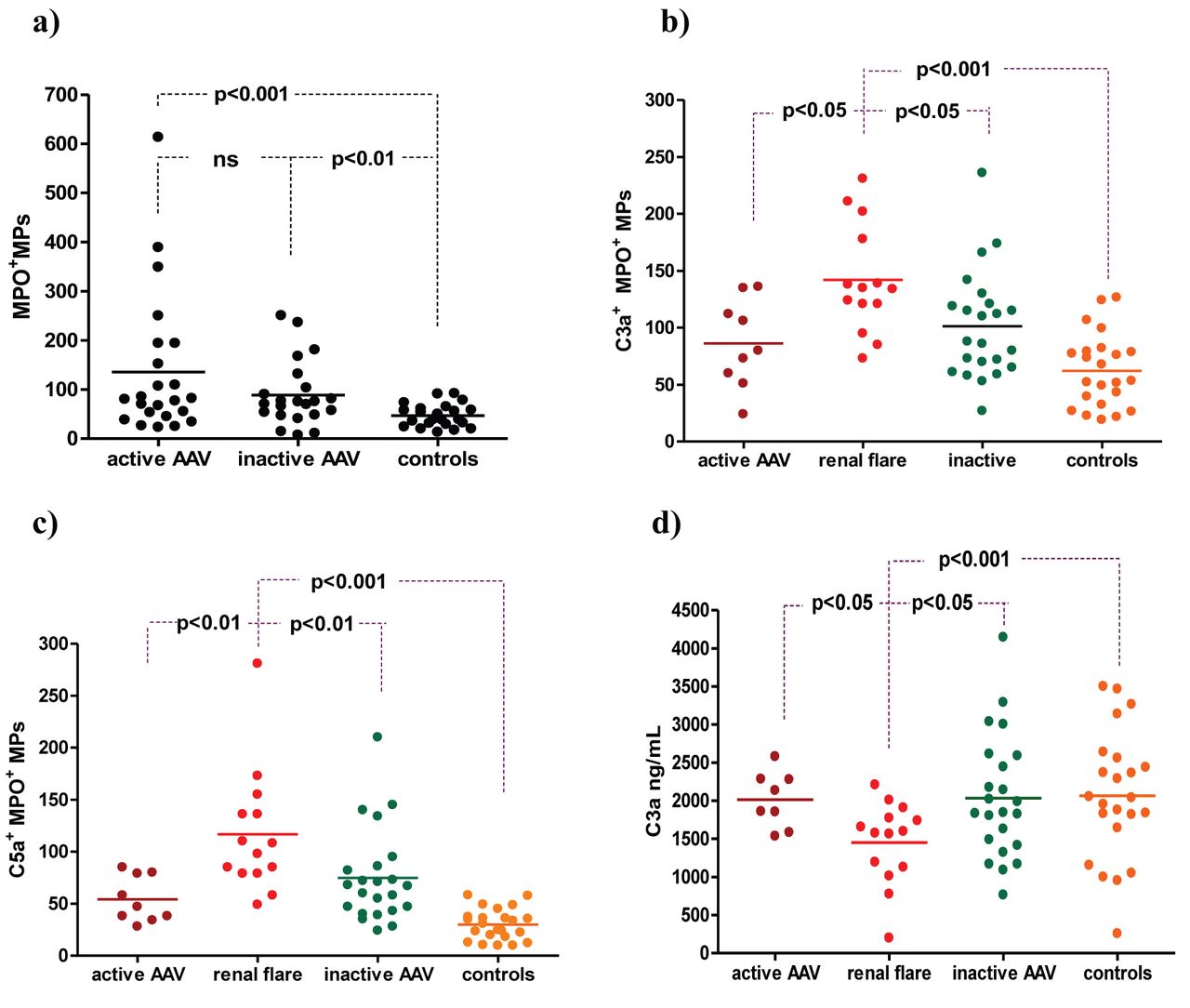
The concentration of MPO+MP was significantly higher in patients with AAV compared to controls, without significant differences between the subgroups of active and inactive AAV patients (Table 3, Figure 1A).

A. Concentration of myeloperoxidase-positive microparticles (MPO+MP) in patients with active and inactive AAV, and controls. B and C. C3a- and C5a-positive MPO+MP in patients with AAV (active, with renal flare, and inactive) and controls. D. Levels of C3a in serum in patients with AAV (active, with renal flare, and inactive) and controls. MPO+MP: myeloperoxidase-positive microparticles; AAV: antineutrophil cytoplasmic antibody–associated vasculitis.
Serum levels of C3a and C5a and the concentration of MPO+MP, and C3a-positive and C5a-positive MPO+MP in plasma of patients with AAV as well as controls.
The concentration of MPO+MP expressing C3a was significantly higher in patients with AAV compared to controls (Table 3), while no difference was found between the active and inactive patients. However, when the group of patients with active AAV was divided according to the presence of active renal flare or nonrenal disease, the concentration of MPO+MP expressing C3a was significantly higher in the renal group of patients compared to the nonrenal group as well as inactive AAV patients and controls (Figure 1B).
As demonstrated in Table 3, the same pattern for MPO+MP expressing C5a was observed regarding the distribution among patients with AAV and compared to controls. Figure 1C presents significantly increased levels of MPO+MP expressing C5a in patients with renal flare compared to nonrenal active AAV patients.
Serum levels of C3a (Table 3) were lower in patients with active disease compared to inactive disease, as well as to controls (p = 0.06 and p = 0.07, respectively), but the significance was reached only when dividing the groups of active patients into those with renal and nonrenal disease (Figure 1D). This was not the case regarding serum C5a levels, neither in the whole group of patients nor in the subgroup of patients with active renal flare. Accordingly, the inverse correlation between the serum levels and expression on MPO+MP existed only in active AAV patients and C3a levels (p = 0.01, r = −0.52).
Serum levels of complement factor C3 did not differ between patients and controls (1.42 ± 0.34 vs 1.54 ± 0.30 g/l, respectively), whether the patients had active or inactive AAV (1.43 ± 0.38 vs 1.42 ± 0.30 g/l, respectively).
A correlation between the levels of C3 and C3a in serum or MPO+MP expressing C3a was not observed.
There were no differences found in the MPO+MP expressing C3a and C5a or serum levels of C3a and C5a between MPO-ANCA– and proteinase 3-ANCA–positive patients.
In the group of active patients, 5 out of 23 were sampled before the treatment with corticosteroids was started. The results of C3a and C5a expression on MPO+MP in these patients were not different compared to the rest of the patients in the active group. There was no correlation between the prednisolone dose and levels of C3a and C5a expressed on MPO+MP in the group of active patients.
In the group of inactive patients, 8 out of 23 were not treated with prednisolone at the time of blood sampling. The levels of investigated variables did not differ between patients with ongoing prednisolone treatment and those without treatment in this group.
There was no correlation between age of the patients, ESR and CRP at the time of blood sampling, renal dysfunction measured by creatinine or eGFR levels, and the levels of the investigated markers on MPO+MP or in serum observed in the whole group of patients. However, a significant correlation was observed between creatinine levels and MPO+MP expressing C3a (p < 0.001, r = 0.57). This correlation was not found for MPO+MP expressing C5a. A highly significant correlation was observed between disease activity measured by BVAS and levels of C3a as well as C5a expressed on MPO+MP (Figure 2). Regarding the serum markers, only C3a was inversely correlated to BVAS (p = 0.03, r = −0.44).
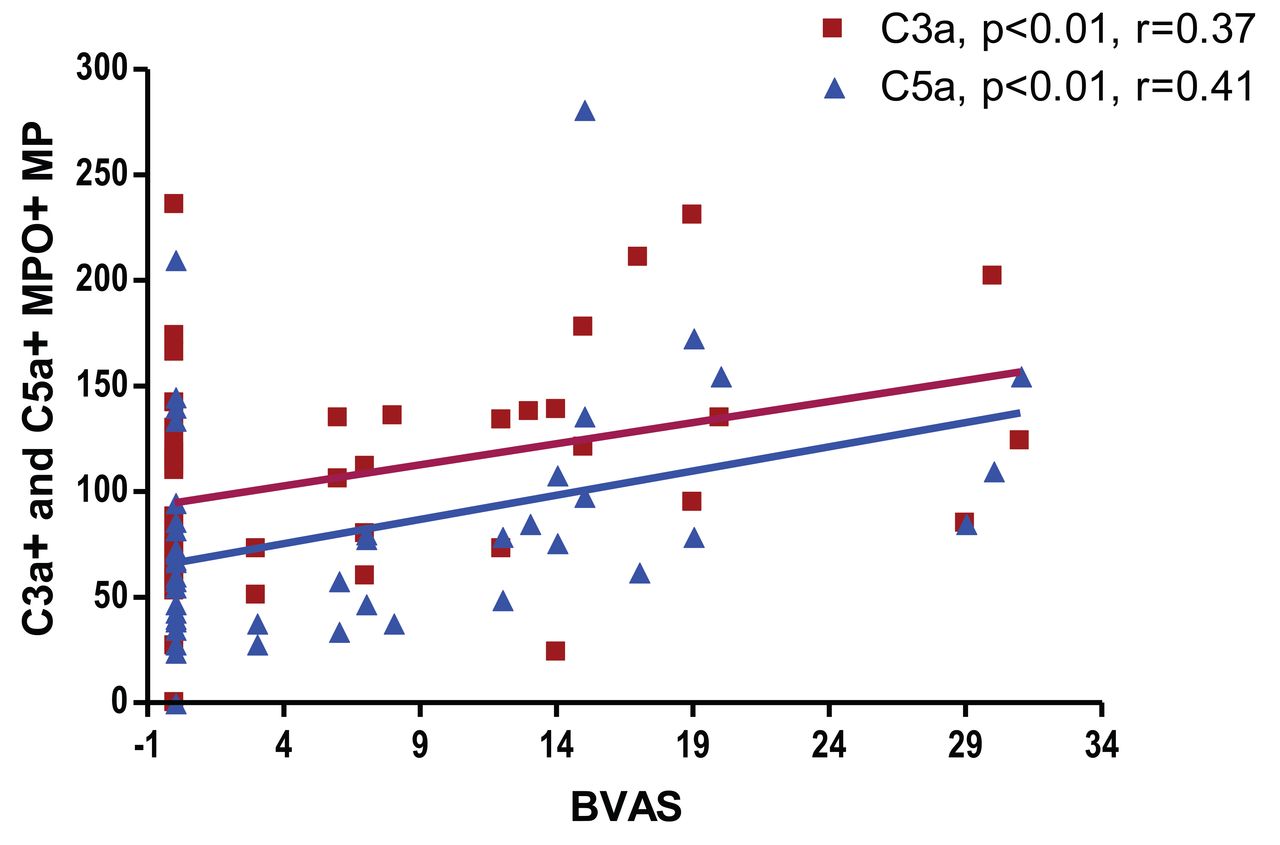
Correlation between disease activity measured by BVAS and levels of C3a and C5a expressed on myeloperoxidase-positive microparticles (MPO+MP). BVAS: Birmingham Vasculitis Activity Score.
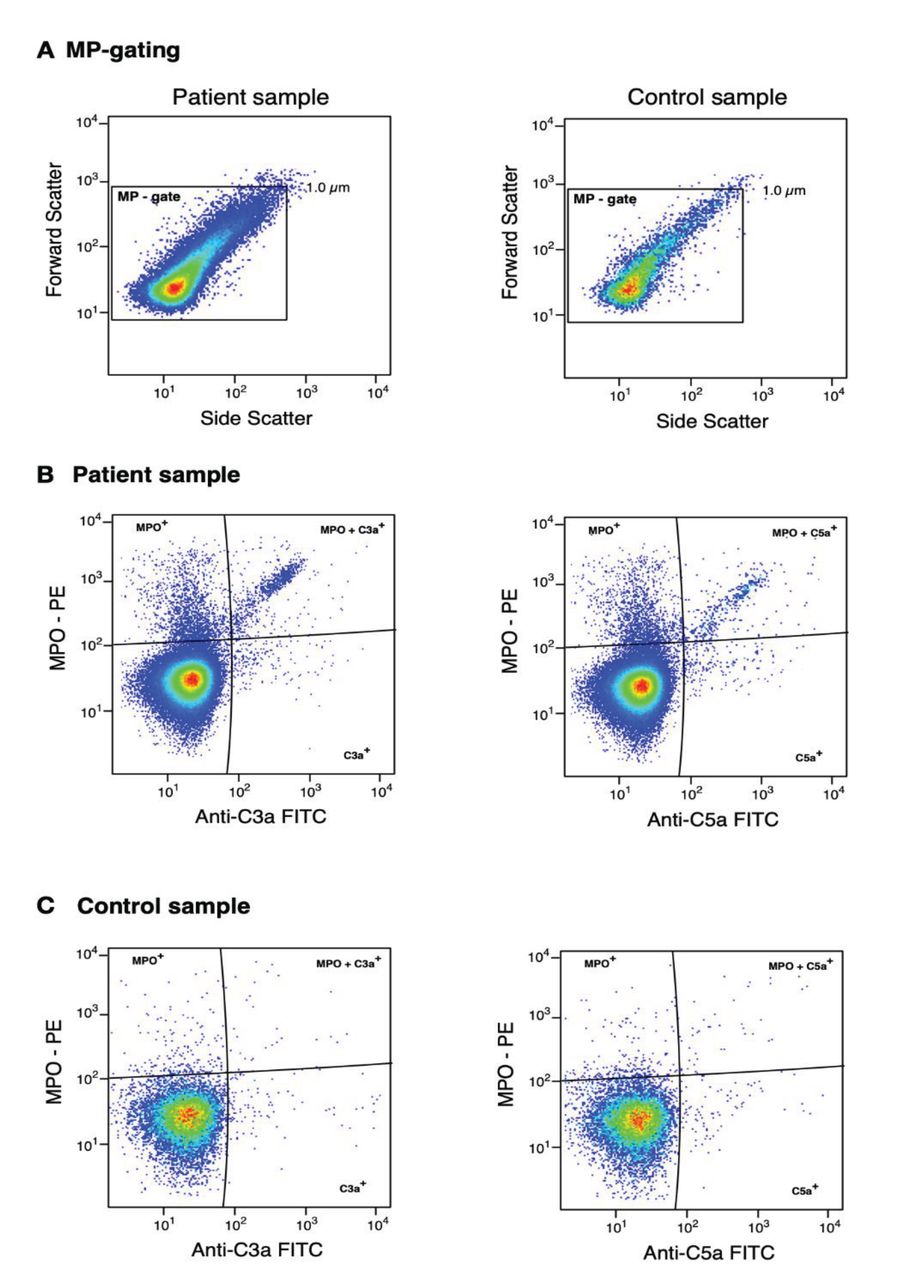
Representative flow cytometry plots of MP expressing MPO together with C3a or C5a are presented in Figure 3.

{kind=link}
{kind=link}
{kind=link}
Representative flow cytometry plots of MP expressing MPO together with C3a or C5a. MP are measured by flow cytometry and defined as particles < 1 μm in size. Moreover, the MP were phenotyped based on MPO and C3a and C5a expression. A. MP in the MP gate in a patient and control sample. B. MP in a patient sample co-expressing MPO together with C3a and/or C5a. C. MP in a control sample co-expressing MPO together with C3a and/or C5a. MP: microparticles; MPO: myeloperoxidase; PE: phycoerythrin.
DISCUSSION
To the best of our knowledge, this is the first study to assess expression of terminal complement components C3a and C5a on MPO+MP in patients with AAV, stipulating the role of C3a and C5a in the pathogenesis of this disease. We have observed strong correlation between the disease activity measured by BVAS and levels of C3a as well as C5a expressed on MPO+MP. Moreover, the expression of C3a and C5a was significantly increased in AAV patients with ongoing renal involvement, suggesting that these highly proinflammatory split products of the complement cascade might be a novel biomarker of renal flare in patients with AAV.
Previous studies have provided evidence that human NMP contain active MPO, suggesting that they may activate endothelial cells and give rise to lesions present in vasculitis22,23. MPO is an enzyme primarily found in granules of neutrophils, but it is also expressed in monocytes, although in lower concentrations28,29. Therefore, the majority of the MPO+MP in the present study originate from neutrophils. Hong and colleagues22 showed that neutrophils primed with tumor necrosis factor-α and stimulated with ANCA antibodies release MP that activate endothelial cells by a reactive oxygen species–dependent mechanism. Further, in vitro studies by Pitanga, et al confirmed that MP released upon neutrophil activation can cause injury to vascular endothelial cells24. More recent studies provide evidence of tissue factor expression on NMP, upon activation of neutrophils by ANCA, indicating a mechanism for hypercoagulability in AAV30,31. Although the presence of bound complement components C1q, C3b, and C4b on cell-derived MP previously were investigated in patients with other autoimmune disorders such as systemic lupus erythematosus and RA32,33,34, this has not been the case in patients with AAV.
Investigation of complement activation in AAV has been focused on C5a since Schreiber, et al4 demonstrated that supernatants from ANCA-activated neutrophils can trigger the complement system through the alternative pathway, resulting in the production of C3a and C5a. C5a could further prime neutrophils for ANCA-induced activation, and only blocking of the C5a receptor on neutrophils could prevent this process. Thereby, the authors could conclude that generation of C5a but not C3a upregulates the membrane expression of ANCA antigens and primes neutrophils for a subsequent ANCA-induced respiratory burst. In the complement cascade, C3 is upstream of C5 and conceivably, C3 is needed for C5a generation as opposed to a direct role in ANCA-induced neutrophil activation. Several experimental data in animal models and observations in patients with AAV verified the role of C5a in the pathogenesis of ANCA-driven diseases, not only by amplification of neutrophil activation but also by attracting more neutrophils at the site of inflammation2,3,4,5,6.
Gou, et al have described increased plasma levels of C3a, C5a, soluble C5b-9, and Bb in patients with active AAV compared with inactive disease35, investigating a cohort with advanced renal involvement in AAV. Further, novel findings indicate that C3d-positive glomerular staining is an independent risk factor for the development of endstage renal disease in ANCA-associated renal vasculitis7. Our study could not demonstrate significant differences in serum C3a and C5a levels between AAV patients and controls. Compared to the study by Gou, et al including patients with advanced impairment of renal function owing to AAV35, we have studied a group of patients with early renal involvement and mainly preserved renal function, even in the group of patients with active AAV. The sample size in our present study may also be a contributing factor to the discrepancies, as well as eventual artifacts due to handling of the samples known to influence complement activation in vitro, and we cannot, in the present setting, confirm the findings of Gou, et al. However, our results of MPO+MP expressing C3a and C5a revealed clear differences and could be a more sensitive method for detection of C3a and C5a, and discriminating between renal and nonrenal involvement. Serum levels of C5a remained similar even in the group of patients with active renal flare, while C3a was decreased in these patients. The inverse relationship between the levels of C3a in serum and those expressed on MPO+MP could be demonstrated in patients with active disease, while this was not the case for C5a. We might speculate that rather than existing in the soluble form in serum, C3a and C5a as acute proinflammatory split products of the complement cascade became available on the surface of circulating MP upon the activation of neutrophils. Thereby, these terminal complement components may be involved in the further enhancement of neutrophil activation.
Previous immunohistochemical examinations of renal biopsy specimens from patients with AAV indeed revealed Bb, C3d, and C5b-9 in glomeruli and in small arteries36. The focal accumulation of complement activation components at sites of glomerular and vascular inflammation and necrosis in ANCA glomerulonephritis differs from the more evenly distributed immunoglobulin and complement components in immune complex–mediated glomerulonephritis36. These findings point toward complement activation at localized sites of inflammation and necrosis in ANCA-associated disease.
Our study of MPO+MP in AAV patients with varying disease phenotypes and activity demonstrates that MPO+MP expressing C3a and C5a are potential novel markers of disease activity in AAV, in particular in renal disease.
Footnotes
This study was performed with the help of ALF funding from Stockholm County Council and Karolinska Institutet, Gustav V’s 80-year Foundation, and the Swedish Rheumatism Association.
- Accepted for publication July 8, 2019.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.