
Abstract
Objective. Describe strategies used to manage rheumatoid arthritis (RA) flares that contribute to a successful postflare outcome.
Methods. Data were collected from the BRASS registry, including clinical and patient-reported outcomes, and a survey with a Likert scale assessing postflare symptoms (better, unchanged, or worse). A logistic regression analysis adjusting for age, sex, flare number in the past 6 months, flare pain severity, home management, clinical consultation, and medication change was performed to evaluate factors influencing flare outcome.
Results. Of 503 participants, 185 reported at least 1 flare that had resolved in the past 6 months, with median (interquartile range) 28-joint count Disease Activity Score based on C-reactive protein 3 score 2.1 (1.7–2.8). Compared with RA symptoms before the flare, 22 (12%) patients felt worse, 125 (68%) were unchanged, and 38 (20%) felt better. To manage flares, 72% of patients used home-based remedies, 23% sought clinical consultation, and 56% made medication change. Of 103 patients who changed medication, 70% did so without seeking clinical advice. Making a medication change (OR 3.48, 95% CI 1.68–7.21) and having lower flare pain (OR 0.83, 95% CI 0.71–0.97) were associated with better flare outcome.
Conclusion. Flares occur frequently even in patients with low disease activity. Independent of home-based or clinically guided care, making a medication change and having less severe pain during a flare were associated with better flare outcomes. Of interest, the decision to change medications was frequently made without clinical advice. Future studies might address how best to intervene when patients experience flares and whether patient-initiated medication changes have adverse outcomes.
- RHEUMATOID ARTHRITIS
- DISEASE-MODIFYING ANTIRHEUMATIC DRUGS
- PAIN
Rheumatoid arthritis (RA) is a chronic, multisystem auto-immune disease primarily affecting the joints. Uncontrolled RA disease activity can lead to joint deterioration and disability1. While therapeutic advancements have been made in treating RA, patients still experience episodes of worsening disease activity called flares, which can worsen longterm functional outcomes2,3,4,5.
Patients with RA, even those in remission, can experience frequent flares6. Recurring flares can increase the risk for cardiovascular disease, radiographic progression, and disability2,3,4,7. Several qualitative studies have been published that report on the range of strategies patients use to manage RA flares8,9,10. These included self-management with rest, heat/cold, or exercise. Additionally, patients sometimes sought assistance from family and friends to help with daily activities. Patients frequently reported adding or changing medications such as nonsteroidal antiinflammatory drugs (NSAID) or corticosteroids. Seeking clinical consultation from a rheumatologist or a primary care physician was often described as a last resort after other remedies have failed9,10.
Little is known about the effectiveness of these types of flare management strategies. A better understanding of these strategies and their efficacy is needed to improve home and clinical care and improve longterm outcomes. This study intends to examine in depth how patients manage their flares, and to expand on previous work11 with this cohort. The aim is to learn about the types of strategies patients use and how they affect postflare outcomes, with the goal of improving longterm clinical and functional outcomes.
MATERIALS AND METHODS
Study population
Data were collected from participants in the Brigham Rheumatoid Arthritis Sequential Study (BRASS), which was initiated in 2003. BRASS is a single-center, prospective RA registry of patients with a clinical diagnosis of RA followed by a hospital-based practice of rheumatologists in Boston, Massachusetts, USA. Participants completed yearly study visits that included an interview, a physician assessment (including a joint count), and a self-administered questionnaire (SAQ) collecting patient-reported outcomes (PRO). Participants were also mailed an SAQ to collect data at the midpoint between annual visits. The registry collects a wide range of clinical data and PRO including, but not limited to, medications, comorbidities, disability, healthcare use, functional status, and 28-joint count Disease Activity Score based on C-reactive protein 3 (DAS28-CRP3). Additional details related to the BRASS registry are described elsewhere12. All patients enrolled in the BRASS study provided informed written consent before starting study procedures. All questionnaires and methods for this study were done in compliance with the Partners Healthcare Institutional Review Board (approval number: 2002P001762; clinical trial registration number, ClinicalTrials.gov: NCT01793103).
Questionnaire
As part of the annual visit, participants were given a survey that collected information about flares. The survey asked participants, “During the past 6 months, have you had a flare in your rheumatoid arthritis?” The survey also asked about the number of flares, the severity of pain for the most recent flare, the duration of the flare, and management strategies for the most recent flare. Strategies included methods used by patients at home (home management) and whether they consulted any physician or clinical service (clinical consultation). Participants were also asked if they increased the strength of a medication already being used or added a new medication to manage their flare, and if so, they were asked details about dosage and duration of use.
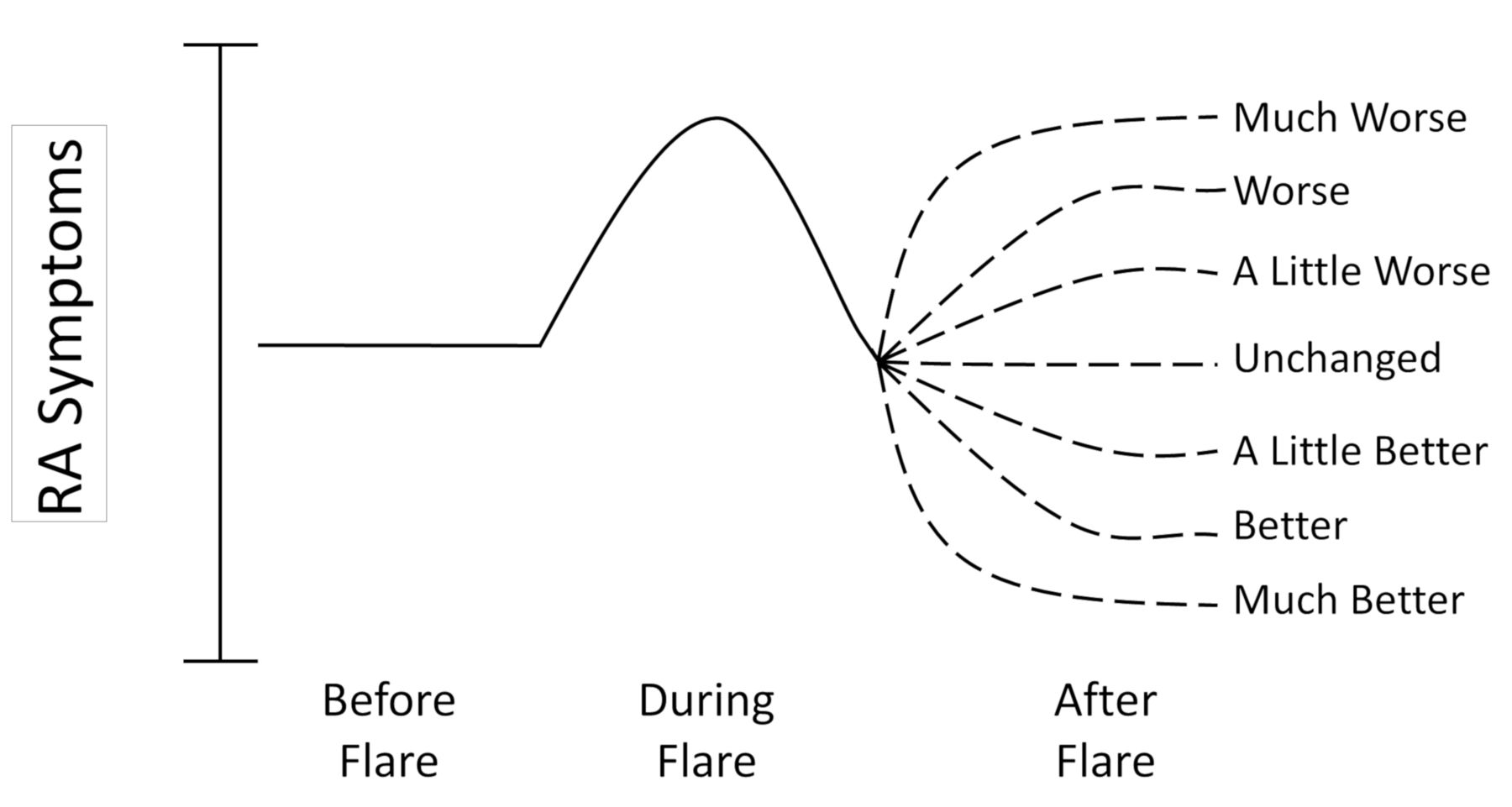
Participants included in this analysis were BRASS patients who reported a flare in the past 6 months that had ended by the time of the survey. The primary outcome was a Likert scale assessing postflare symptoms. Participants were asked to complete the following: “As compared to the symptoms just before my most recent flare, my overall RA symptoms after my flare were …,” with “much worse,” “worse,” “a little worse,” “unchanged,” “a little better,” “better,” or “much better.” This, combined with a visual representation, prompted participants to compare their postflare symptoms relative to their pre-flare symptoms. For the purposes of the analysis, the 7 categories were collapsed into 3: worse, unchanged, or better (Figure 1).

Likert scale assessing postflare outcomes. RA: rheumatoid arthritis.
Statistical analyses
Descriptive statistics were used to generate summary tables of the cohort. Different statistical methods were used based on type of variable to test whether there were significant differences between the response groups (worse, unchanged, or better postflare symptoms). For the normally distributed variable (age), a 1-way ANOVA test was performed. The non-normally distributed variables (no. flares and flare pain severity) were analyzed with a nonparametric Kruskal-Wallis test. The categorical variables (sex, any home management, any clinical management, flare duration, any medication change) were examined with the exact Mantel-Haenszel chi-square test. From the univariate analyses, age, sex, and all variables with a p ≤ 0.2 were included in the final model. In the next step, a proportional odds logistics regression analysis was performed using postflare symptoms (worse, unchanged, or better) as the dependent variable, and age, number of flares, flare pain severity, sex, any home management, any clinical management, and any medication change as the independent variables. A secondary analysis was performed with the individuals who had a previous DAS28-CRP3 measured and this covariate was included in the model. The results of the final model were presented as OR estimates with their 95% Wald CI calculated. Model assumptions were also tested using a backward selection analysis.
In an additional analysis, proportional odds logistics regression was performed with all the same independent variables, but with the any medication variable separated by type: NSAID (yes/no), corticosteroid (yes/no), and disease-modifying antirheumatic drug (DMARD; yes/no). A p value < 0.05 was considered statistically significant. Data collected in the surveys were maintained using a Microsoft Access Database. All statistical analyses were performed using SAS 9.4 (SAS Institute Inc.).
RESULTS
Of the 503 participants who completed the survey, 185 reported at least 1 prior flare that had ended in the last 6 months; these were included in the analyses. Most participants were female, white, and had a college or graduate school degree (86%, 93%, and 72%, respectively). Their mean (SD) age was 59 (14) years, 76% had seropositive RA, and the median (interquartile range) disease duration was 15 (9–24) years. Participants already taking biologics made up 63% of the cohort and 23% used oral corticosteroids as part of their ongoing therapy. More than 85% of this cohort had low disease activity at the time of the survey and the median DAS28-CRP3 was 2.1 (1.7–2.8; Table 1).
Demographics and clinical characteristics of study cohort (n = 185).
The median number of flares in the previous 6 months was 2 (1–4), with a median flare pain severity of 7 (5–8) for the most recent flare. The most common flare duration category for the most recent flare was 1–3 days (Table 2). While only 20% of participants reported that their RA symptoms were improved after their flare, 12% reported that their symptoms worsened, and 68% reported that their symptoms were unchanged.
Description of flares and flare management strategies (n = 185).
Seventy-two percent of participants (n = 133) who had a flare used home management strategies as part of their treatment for the most recent flare. The most commonly reported strategies were rest, application of heat/cold, and/or use of an assistive device (brace, splint, cane). Fifty-six percent (n = 103) made a medication change (increasing dosage and/or adding new medication) to treat their flare symptoms, and 23% (n = 43) sought clinical consultation. Of the 43 participants who sought clinical consultation, 36 (84%) sought the advice of their rheumatologist. Those 36 used multiple modes of contacting their rheumatologist, including 22 in-person visits, 15 phone calls, and 7 e-mail messages. Only 3 (7%) participants consulted a primary care physician for help managing their flare (Table 2). Among those who consulted with their primary care physicians, there were 2 office visits, 2 phone calls, and 1 e-mail.
Of the 103 participants who made a medication change to manage their flares, 50 modified their NSAID regimen, 28 modified their corticosteroid use, and 22 modified their DMARD regimen. Out of the 50 NSAID changes, 16 participants increased their current dose, and 34 added a new NSAID. Seven of the 28 corticosteroid alterations were increases in dose (mean increase in dosage was 6.4 mg ± 5.3 mg), while 21 were new starts (mean new dose was 14.3 mg ± 14.1 mg). Out of the 22 subjects who made modifications to their DMARD, 12 increased their current dose and 10 added 1 or more DMARD. Of the DMARD modified, 14 were nonbiologics, all of which were methotrexate (MTX). Twelve of the DMARD modified were biologics (9 were tumor necrosis factor–α inhibitors in addition to 1 each of tofacitinib, tocilizumab, and abatacept). Only 3 participants added a new narcotic (2 oxycodone, 1 tramadol) and none increased their existing dose for their flare management (Table 3). Overall, the average duration of an increased dosage of any medication for flare management was 33.2 (47.6) days. Those who used a new medication did so for an average of 39.5 (59.3) days. Notably, 72 (70%) of those who made any medication change did so without consulting a physician, and 32% of the changes to DMARD were also made without physician consultation. All medication changes described here were made to manage the most recent flare.
Type of medication change for flare management according to type of consultation (n = 103).
A comparison was done of the demographic and clinical variables in Table 1, comparing those who initiated home management with those who did not. No differences were found between the 2 groups, other than a higher number of women using home management strategies [122 (92%) vs 37 (71%), p = 0.0003]. Similarly, in a comparison of demographic and clinical variables (Table 1) of those who initiated medication management versus those who did not, no significant differences were found. There were 69 (37%) patients who used both home management and medication changes for their flares.
Table 4 illustrates the univariate comparisons among the flare outcome groups (worse, unchanged, better) by clinical and demographic variables. Among all the variables, lower flare pain severity (p = 0.03) and making a medication change (p < 0.0001) were significantly associated with better flare outcomes at the p value < 0.05 level.
Univariate comparisons of flare outcomes by clinical and demographic variables.
An analysis was done to compare those who did and those who did not have a flare in the preceding 6 months. Participants who flared in the last 6 months were younger [58.5 (13.5) vs 63.3 (12.6) yrs, p = 0.0004], had a higher median DAS28-CRP3 score [2.1 (1.7–2.8) vs 1.8 (1.5–2.4), p = 0.001], and were more likely to be seropositive (76% vs 64%, p = 0.0114). There were some differences in medication use as well. Participants who flared in the last 6 months were more likely to use narcotics (11% vs 4%, p = 0.0066) and had a higher median MTX dosage [20 (15–25) vs 17.5 (15–25) mg per week, p = 0.0227; Appendix 1].
A proportional odds logistic regression analysis was performed to determine which factors were associated with a better flare outcome (Figure 2A). In the adjusted model, only flare pain severity and making a medication change to manage a flare were associated with a better flare outcome. Participants with higher pain severity during their most recent flare had lower odds of having a better flare outcome (OR 0.8, p = 0.02). Those who made any medication change had higher odds of having a better flare outcome (OR 3.5, p = 0.0008). This result was further reinforced by a backward selection model using the same predictors — flare pain severity (OR 0.9, p = 0.03) and making a medication change (OR 3.7, p = 0.0002) remained in the model.

{kind=link}
{kind=link}
A. Adjusted OR estimating better postflare symptoms (n = 181). B. Adjusted OR estimating better postflare symptoms by medication category (n = 169). DMARD: disease-modifying antirheumatic drug; NSAID: nonsteroidal antirheumatic drug.
A similar logistic regression model was performed separating out the medication change variable by category. The different medication categories (NSAID, corticosteroids, and DMARD) showed similar results, where the type of medication changed predicted a better flare outcome compared with no medication change (Figure 2B). A model that made comparisons between the medication categories did not find that any one category was more likely to predict better outcomes.
An additional proportional odds logistic regression analysis was run that included a subset of subjects with a prior DAS28-CRP3 score (n = 110) to evaluate whether previous disease activity affected postflare RA symptoms. Making any medication change was still the strongest factor affecting postflare RA symptoms (OR 4.0, 95% CI 1.5–10.6). Adding this variable did not alter the findings of the main model. Additionally, among the 110 patients who had consecutive DAS28-CRP3 scores, there was little within-patient difference of scores (mean 0.11 ± 1.12, p = 0.33 Wilcoxon signed-rank test for paired data).
DISCUSSION
In our study, flares occurred frequently, and most patients who experienced a flare had more than one in the last 6 months. Nearly three-quarters of the patients who flared used home-based interventions (such as rest, heat, or cold) to manage their symptoms; however, only making a medication change was associated with a better flare outcome. More than half of the participants in this cohort modified their medications to manage their flare symptoms; interestingly, most participants who made medication changes did so without seeking clinician input. While most of the medication changes were to NSAID or corticosteroid use, many also modified DMARD on their own. Having a milder flare also contributed to a better flare outcome, indicating that it is both management and clinical factors that contribute to an improved flare resolution.
A previous study of the BRASS registry by Bykerk, et al11 reported that a similar percentage of participants modified DMARD during a flare, and these changes were more likely to have been made by those with longer duration flares. In this analysis, a higher flare pain severity diminished the likelihood of a better flare outcome, while medication changes increased that likelihood. Flare duration was influential in the study by Bykerk, et al; however, it did not have an influence on flare outcome in our study. It is possible that indirectly, flare duration had an effect on flare outcome by triggering patients to make a change in pharmacologic therapy. Similar to findings in this analysis, in Bykerk’s analysis nearly three-fourths of the patients used either home-based or pharmacologic strategies to manage their flares. They were unable to provide data on whether patients consulted physicians for help managing their flare but hypothesized that patients often self-manage flares. This study was initiated to address those questions and better understand which strategies contributed to improved flare outcomes, postulating that this might be associated with better longterm clinical and functional outcomes.
This analysis found that the majority of individuals who made a medication change to manage their flare symptoms did so without seeking clinical advice. This is similar to findings reported by Hewlett, et al10, which found that flares were frequently self-managed and that increasing medication use also commonly occurred without clinical advice. In that study, patients sought help when symptoms could not be contained, or were described as complex whole-body experiences. In this analysis, patients were not specifically queried as to why they may or may not have consulted their physician. More patients made changes to NSAID without clinical advice than to DMARD. Conversely, more patients who changed their DMARD sought clinical advice compared with those who made NSAID or corticosteroid changes. Nevertheless, all medications have possible adverse effects and clinical input may improve patient safety. This illustrates the need to understand whether accessibility issues or self-efficacy factor into patients’ decision-making process when modifying medications. Given how frequently patients self-manage their flares, it could be beneficial for clinicians to consider a prespecified plan with their patients on how to better manage their symptoms and when to call for clinical advice.
Even though there has been some research on flare management strategies11, little is known about predictors of better flare outcomes. Flares occur frequently in RA, and research has demonstrated that they are associated with worse longterm clinical outcomes, such as lower functional status and radiographic progression3,4. There is a need for additional research on how patients manage their flares and which strategies contribute to improved longterm outcomes. The results of this study support the finding that, in the short term, individualized drug therapy adjustments may be an effective way to manage flares.
Our study has several limitations. This cohort is mostly composed of patients in remission or with low disease activity; thus it is difficult to extend these findings to newly diagnosed RA or moderate to high disease activity groups. Similarly, the cohort is predominantly white and highly educated (college or graduate school degree). These findings may not be generalizable to less educated or non-white populations. Additionally, the longterm effects of patients making self-initiated medication changes cannot be assessed because of the cross-sectional design. Another limitation of this analysis is that it is based on patients’ recall of their flare(s) in the last 6 months, which is less reliable than real-time reporting of flare intensity or having DAS28-CRP3 scores before and after the flare. Further, having had some information about an individual’s immediate pre-flare pain level may have helped shed light on their choice of management strategies. Nevertheless, a strength of this analysis is its ability to detail the most effective patient-initiated strategies for flare management, which has not been previously studied in depth, to our knowledge.
This study demonstrates that patients, even those in low disease activity, can experience several flares in a 6-month time period. Patients implemented home-based and/or pharmacological interventions to manage their flares and patients who managed their flare symptoms with a medication change often did so without clinician input. Better flare outcomes were associated with making a medication change of any type, and having lower pain severity during the flare. These findings help explain how a patient’s self-management of flares contributes to better flare outcomes and informs future initiatives on flare management. Future studies should focus on the reasons patients initiate medication changes for flare management without contacting their rheumatologist and whether doing so is associated with any longterm adverse events. This would illuminate the best methods to maximize patient safety through more proactive clinical engagement or an education module to optimize patients’ self-initiated flare management strategies.
APPENDIX 1. Demographic and clinical characteristics of those who did and did not have a flare in the preceding 6 monthsa.
Footnotes
Research reported in this publication was supported by Mallinckrodt Pharmaceuticals. The funders had no role in study design, data collection, analysis, decision to publish, or preparation of the manuscript. Additionally, the BRASS registry is funded by Amgen, Bristol-Myers Squibb, Crescendo Bioscience, Regeneron, and Sanofi.
- Accepted for publication May 30, 2019.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.