
To the Editor:
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disorder characterized by fluctuating levels of immune response hyperactivity, high serum titers of nucleic antigen-specific autoantibodies, and persistent production of type-I interferon (IFN)1. One route to controlling SLE has been to exploit the properties of T cell lymphocyte costimulation inhibitor (CTLA-4), a selective costimulation inhibitor, which suppresses auto-antigen-specific T cell response intensity2. Although the full-length cell-surface receptor CTLA-4 is well characterized, other alternatively spliced isoforms exist, including a soluble form of the molecule (sCTLA-4)3. Initial analysis of sCTLA-4 in patients with SLE described raised serum levels compared with healthy donors, and sCTLA-4 levels correlated with disease activity4, but little is known of whether it plays any role in SLE. Currently, this is a relevant question because there is anecdotal evidence that CTLA4-Ig can have clinical benefits for some patients with SLE5.
Studies of sCTLA-4 using current anti–CTLA-4 antibodies should be interpreted with caution because they are raised against the extracellular region, found in the receptor, cleaved receptor artifact and the soluble isoform, hence obscuring the contribution of native sCTLA-4. Here, using antibodies raised specifically against native sCTLA-46,7, we determined whether sCTLA-4 contributes to the immune response underlying SLE, particularly regarding SLE markers IFN-α and anti-dsDNA antibody levels. The study included 104 patients with SLE and 40 healthy volunteer donors and first compared serum levels of IFN-α (Figure 1). All methods were carried out in accordance with the Grampian Health Board (UK) and the University of Aberdeen ethical committee. Experimental protocols were approved by East of Scotland Research Ethics Committee (ref: REC 10/S1401/20). Written informed consent was obtained from all donors.
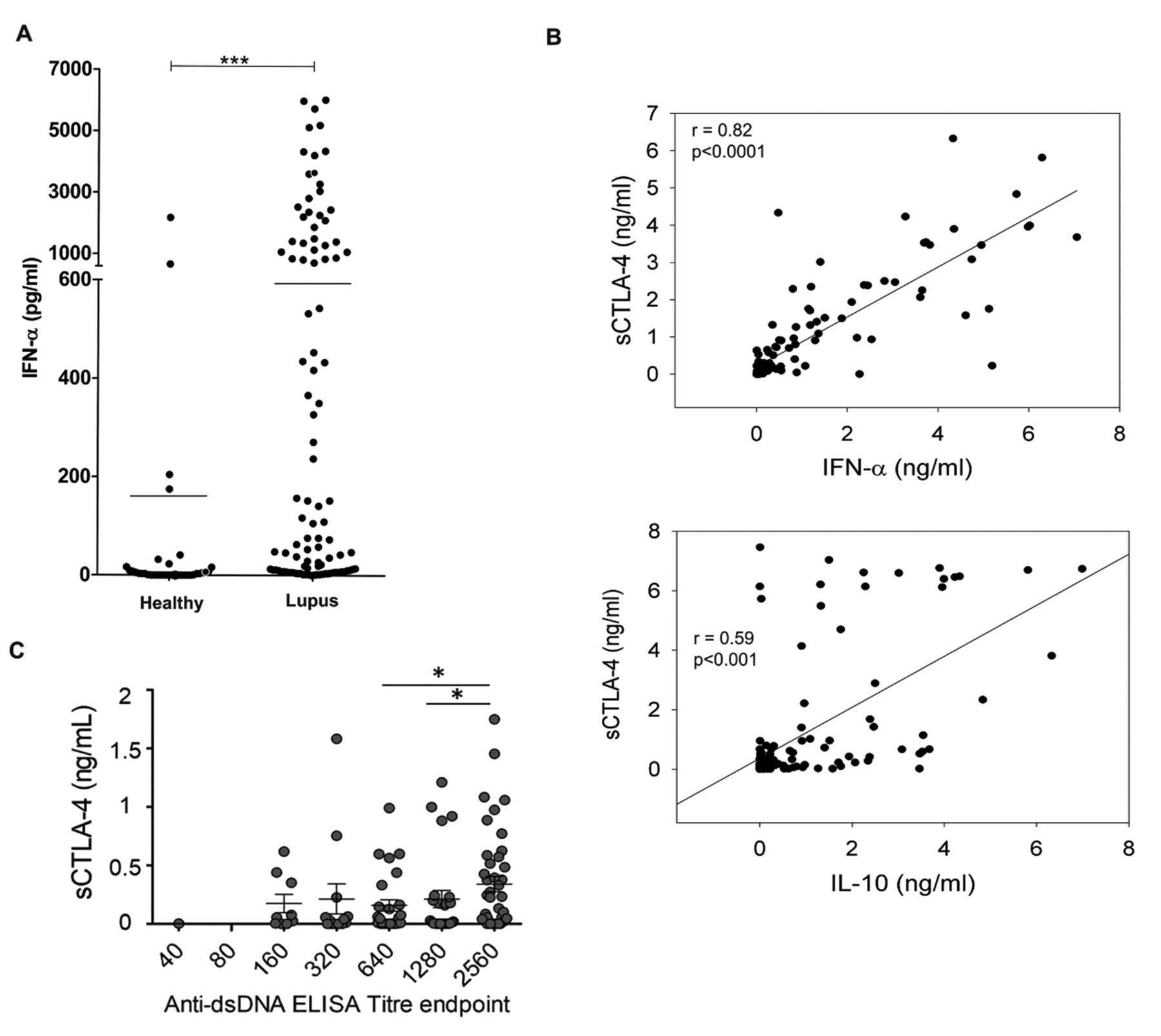
Correlation analysis of sCTLA-4 serum levels with IFN-α, IL-10, and anti-dsDNA antibody titer in patients with SLE. A. IFN-α levels were measured by ELISA in serum from patients with SLE (n = 104) versus healthy volunteer donors (n = 40; *** p < 0.001; p values determined by nonparametric Mann-Whitney U test) using Mabtech human IFN-α ELISA development kit. B. Regression analysis of IFN-α (upper panel) and IL-10 (lower panel) with sCTLA-4 serum levels from patients with SLE (n = 104, Spearman rank analysis). C. Comparison of mean sCTLA-4 levels with anti-dsDNA autoantibody titer in serum samples from patients with SLE (n = 119). Error bars represent SD, horizontal bar indicates median. * p < 0.05. sCTLA-4: soluble T cell lymphocyte costimulation inhibitor; IFN: interferon; IL: interleukin; SLE: systemic lupus erythematosus.
As expected, serum levels of IFN-α in the cohort of patients with SLE were significantly higher than in the healthy volunteer group (p < 0.0001), with 52% of patients having serum levels of IFN-α > 100 pg/ml and 33% of patients with levels of > 1 ng/ml (Figure 1A, p < 0.0001). Further, IFN-α levels correlated closely with serum levels of sCTLA-4 in the cohort of patients with SLE (r = 0.82, p < 0.0001, Figure 1B, top panel). This demonstrates for the first time, to our knowledge, a positive correlation between serum levels of these molecules. Although the general inhibitory effects of interleukin (IL)-10 on antigen-presenting cells and T cell activation are well-known in SLE, interleukin 10 (IL-10) also augments B cell proliferation and immunoglobulin class-switching, leading to increased autoantibody production8. We compared sCTLA-4 and IL-10 levels in patient serum, which revealed another significant but weaker correlation (r = 0.59, p < 0.001, Figure 1B, lower panel). Mean serum levels of sCTLA-4 were generally raised and significantly elevated in patients with higher titers of anti-dsDNA autoantibodies (Figure 1C).
We next analyzed whether genetic variation within the CTLA-4 gene was associated with the IFN-α levels seen in patients with SLE. Previously, the CT60 (rs3087243) G/G single-nucleotide polymorphism (SNP) has been reported as an autoimmune disease susceptible haplotype with a tendency to produce lower levels of sCTLA-4 compared to the A/A disease-resistant haplotype9. We also included in the study 2 other functional CTLA-4 SNP, +49G>A (rs231775) and −318C>T (rs5742909). We genotyped 125 patients with SLE and performed correlation analysis of genotype with sCTLA-4, IFN-α, and IL-10 levels from serum or resting cell culture supernatants, following 72 h of patient peripheral blood mononuclear cell cultures (Figure 2). In our analysis, levels of serum or cell-culture supernatant sCTLA-4 did not differ in individuals carrying the G/G or A/A homozygous haplotype compared to the A/G heterozygous haplotype (Figure 2). Interestingly, while there was no statistically significant difference in IFN-α serum levels between any of the SNP cohorts, patients with SLE who carried the CT60 risk genotype (G/G) had raised levels of resting cell supernatant levels of IFN-α compared with those carrying the heterozygous (A/G) genotype (p = 0.055). Analysis of IL-10 in cell supernatants based on CT60 genotype showed significantly raised levels in the G/G cohort compared with the nominally resistant A/A group (Figure 2; Kruskal-Wallis nonparametric ANOVA p < 0.05). We did not find any other significant association between sCTLA-4, IFN-α, or IL-10 levels and the alleles associated with the +49G>A and −318CT SNP (data not shown). The trends identified in this analysis are potentially related to study sample size, and suggest that a much larger study cohort should be considered to fully evaluate the relationship between particular CTLA-4 SNP and levels of sCTLA-4, IFN-α, and IL-10 in SLE.

{kind=link}
{kind=link}
Analysis of sCTLA-4, IFN-α, and IL-10 levels in serum and supernatant of patients with SLE segregated according to CT60 SNP genotype (A/A “resistant”, G/G “susceptible”; statistical values determined by nonparametric Kruskal-Wallis ANOVA with a Dunn’s multiple comparison post-test; median values are shown, * p < 0.05). Genomic DNA was extracted from 100 µl of whole blood using Qiagen DNeasy blood and tissue kit according to manufacturer’s instruction. SNP CT60 in the 3′ untranslated region (rs3087243) of the CTLA-4 gene were typed by allelic discrimination methods using TaqMan SNP assays (Applied Biosystems). sCTLA-4: soluble T cell lymphocyte costimulation inhibitor; SNP: single-nucleotide polymorphism; IFN: interferon; IL: interleukin; SLE: systemic lupus erythematosus.
We detect a correlation between serum levels of sCTLA-4 and IFN-α and other characteristic features of SLE including IL-10 and anti-dsDNA autoantibody serum levels. Given these correlations, one important question is whether sCTLA-4 actually contributes to or restricts disease activity in some way, perhaps through modulation of IFN-α function. The data here suggest the latter and may in part explain why CTLA4-Ig is relevant therapeutically to SLE but has been relatively difficult to bring successfully through clinical trials10. In support of this latter notion, natural sCTLA-4 is likely to be functionally similar in many respects to recombinant CTLA4-Ig and thus its presence at high levels in serum might both confound interpretation of efficacy data and obscure the therapeutic benefits of CTLA4-Ig in SLE. It will therefore be important to assess whether such a correlation exists in other broad ranges of type I interferonopathies and if sCTLA-4 could be used as a prognostic/diagnostic biomarker of disease activity and therapeutic outcome.
Acknowledgment
We are grateful to Dr. Nick Fluck, Dr. Neil Basu, Dr. Lars P Erwig, and Dr. Hazem Youssef for their invaluable support in recruiting patients for the study; Prof. Georgina L. Hold for assistance and interpretation with SNP studies; and Vivien Vaughan for her expertise in recruiting study participants and maintaining ethical documentation.
Footnotes
This work was supported by Arthritis Research UK (Grant no. 19282). F.J. Ward, L.N. Dahal, and R.N. Barker have filed a patent covering the use of the monoclonal antibody targeting the soluble isoform of CTLA-4 as a therapeutic agent. L.N. Dahal and F.J. Ward share joint senior authorship of this article.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.