
Abstract
Objective Comorbidity burden and obesity may affect treatment response in patients with rheumatoid arthritis (RA). Few real-world studies have evaluated the effect of comorbidity burden or obesity on the effectiveness of tocilizumab (TCZ). This study evaluated TCZ effectiveness in treating RA patients with high versus low comorbidity burden and obesity versus nonobesity in US clinical practice.
Methods Patients in the Corrona RA registry who initiated TCZ were stratified by low or high comorbidity burden using a modified Charlson Comorbidity Index (mCCI) and by obese or nonobese status using body mass index (BMI). Improvements in disease activity and functionality after TCZ initiation were compared for the above strata of patients at 6 and 12 months after adjusting for statistically significant differences in baseline characteristics.
Results We identified patients with high (mCCI ≥ 2; n = 195) and low (mCCI < 2; n = 575) comorbidity burden and patients categorized as obese (BMI ≥ 30; n = 356) and nonobese (BMI < 30; n = 449) who were treated with TCZ. Most patients (> 95%) were biologic experienced and about one-third of patients received TCZ as monotherapy, with no significant differences between patients by comorbidity burden or obesity status. Improvement in disease activity and functionality at 6 and 12 months was similar between groups, regardless of comorbidity burden or obesity status.
Conclusion In this real-world analysis, TCZ was frequently used to treat patients with high comorbidity burden or obesity. Effectiveness of TCZ did not differ by comorbidity or obesity status.
- comorbidity
- obesity
- registry
- rheumatoid arthritis
- tocilizumab
Rheumatoid arthritis (RA) is a chronic autoimmune disease that leads to inflammation and progressive destruction of synovial joints. Comorbid conditions are more common, often more severe, and less well-managed in patients with RA compared with the general population1,2. Higher comorbidity burden is associated with a higher degree of disease activity and physical disability and a poorer health-related quality of life3,4. In addition, higher comorbidity burden was reported to impair response to treatment in patients with RA5. One common comorbidity, obesity, is more prevalent in patients with RA than in the general population6,7. Obese patients with RA often have higher disease activity8 and poorer responses to therapy than nonobese patients9,10,11,12,13.
Tocilizumab (TCZ) is a humanized monoclonal antibody against the interleukin 6 receptor approved for patients with moderate to severe RA14. Although caution should be used in patients with diverticulitis, chronic or recurrent infections, neutropenia, or thrombocytopenia, the existence of prior comorbidities does not contraindicate its use14. The dose of TCZ can be adjusted based on patient weight. Few studies have investigated the use of TCZ in patients with high comorbidity burden or obesity and their effect on the effectiveness of TCZ in routine clinical practice15,16. This analysis evaluated the clinical response to TCZ in patients with RA stratified by comorbidity burden and obesity.
MATERIALS AND METHODS
Study setting
The Corrona RA registry is an ongoing, independent, prospective, observational cohort of patients with RA (ClinicalTrials.gov: NCT01402661)17,18 and has been previously described18. Patients are recruited from 174 private and academic practice sites across 41 states in the United States, with 686 participating rheumatologists. As of March 31, 2018, data on 48,535 patients with RA were collected. The Corrona database includes 367,457 patient visits and about 169,968 patient-years of follow-up observation time. The mean duration of patient follow-up is 4.30 years (median 3.35 yrs).
Patient population
This study included patients with RA aged ≥ 18 years in the Corrona registry who initiated TCZ between January 1, 2010, and October 31, 2017, and had follow-up visits at 6 and 12 months (± 2 mos) after initiation, regardless of whether TCZ was continued for the entire follow-up period. For analysis inclusion, patients must have had baseline body mass index (BMI) available and the necessary data for a modified Charlson Comorbidity Index (mCCI) score.
The study was conducted according to the current version of the Declaration of Helsinki. Ethics approvals were obtained from the New England Independent Review Board (IRB; no. 120160610) for private practice sites and the local IRB of participating academic sites. All patients provided written informed consent.
Study design and outcomes
This was a retrospective study to evaluate the use of TCZ and to determine whether the effectiveness of TCZ differs in obese versus nonobese patients and high versus low comorbidity burden at baseline.
For comorbidity burden, patients were stratified into low versus high comorbidity burden groups by mCCI. CCI is a weighted index of comorbid conditions that functions as a predictor of mortality19. The mCCI was calculated as the sum of prior (history of ) physician-reported comorbid conditions in the Corrona registry, including myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, chronic obstructive pulmonary disease (COPD), peptic ulcer disease, diabetes mellitus, leukemia, lymphoma, solid-tumor cancer (excluding nonmelanoma of the skin), and liver disease. Conditions that were not captured and were excluded from mCCI score include dementia, kidney disease, hemiplegia, and acquired immunodeficiency syndrome. The CCI includes connective tissue disease, which was coded as 1 for all participants, because the population was limited to patients with RA. Low comorbidity burden was an mCCI score of < 2 and high comorbidity burden was an mCCI score of ≥ 2.
To assess the effect of obesity, patients were stratified into the nonobese group if BMI was < 30 and into the obese group if BMI was ≥ 30. BMI and mCCI were calculated at the time of TCZ initiation.
Outcomes were evaluated at 6 and 12 months post-TCZ initiation; ± 2 months was allowed in order to classify a visit as a 6- or 12-month follow-up visit. The primary endpoint was mean change in Clinical Disease Activity Index (CDAI) from baseline to 6 months and from baseline to 12 months. Secondary endpoints were evaluated at the same timepoints and included TCZ dose, mean change in Health Assessment Questionnaire (HAQ) score, the proportion of patients who achieved low disease activity (LDA; CDAI ≤ 10), and patients with change greater than or equal to the minimum clinically important difference (MCID) in CDAI and HAQ. MCID for CDAI was calculated based on baseline CDAI (if CDAI ≤ 10 at baseline, then MCID = 2; if CDAI > 10 to ≤ 22 at baseline, then MCID = 6; if CDAI > 22 at baseline, then MCID = 11)20. MCID for HAQ was defined as a reduction from baseline ≥ 0.2220.
Statistical analysis
Patients were categorized based on mCCI (high vs low comorbidity burden) and BMI (obese vs nonobese). Baseline demographics, clinical characteristics, disease activity, and treatment history were described for all patient categories. Standardized differences were calculated between high versus low mCCI and obese versus nonobese patients to identify statistically significant differences at baseline (time of TCZ initiation).
Outcomes at 6 and 12 months were compared in both unadjusted and adjusted analyses. Baseline characteristics with an absolute standardized difference > 0.1 were identified as covariates for inclusion in adjusted comparisons. Outcomes were compared between cohorts using 2-sample t tests or chi-square tests in unadjusted analyses, and linear or logistic regression models in adjusted analyses.
For patients who discontinued TCZ but did not switch to another biologic prior to the 6- or 12-month follow-up visit, outcomes at the 6- and 12-month visits were included as observed. For patients who discontinued TCZ and switched to a different biologic prior to the 6- or 12-month follow-up visit, disease activity and patient-reported outcomes (PRO) at the time of switch were used as the 6- or 12-month endpoints (last observation on TCZ carried forward) for evaluation of continuous outcomes, and nonresponse was imputed for analysis of binary outcomes.
RESULTS
Patient baseline characteristics by comorbidity burden
Of 805 patients who initiated TCZ, 770 had mCCI data available at baseline; 575 patients (74.7%) had a low mCCI, and 195 (25.3%) had a high mCCI. As shown in Table 1B, over 95% of patients were biologic experienced, and about one-third received TCZ monotherapy. Most patients (93.8%) received intravenous (IV) TCZ (Supplementary Table 1, available with the online version of this article). Of the 706 patients (93.8% of all initiators) who received IV TCZ, 528 (74.7%) had a low mCCI and 178 (25.2%) had a high mCCI. Among all IV TCZ initiators, 407 (57.6%) had baseline dose information [low mCCI: 316 (59.8%); high mCCI: 91 (51.1%)]. Of IV TCZ initiators with dose available (n = 407), 230 (56.5%) received 4 mg/kg [low mCCI: 172 (54.4%); high mCCI: 58 (63.7%)] and 177 (43.5%) received 8 mg/kg [low mCCI: 144 (45.6%); high mCCI: 33 (36.3%)]. Of the 47 (6.1% of all initiators) patients who initiated subcutaneous (SC) TCZ, 36 (76.6%) had a low mCCI and 11 (23.4%) had a high mCCI. Of SC TCZ initiators, 30 (63.8%) had baseline dose frequency available [low mCCI: 26 (72.2%); high mCCI: 4 (36.4%)]. Of SC TCZ initiators with dose available (n = 30), 13 (43.3%) received TCZ every 2 weeks [low mCCI: 10 (38.5%); high mCCI: 3 (75.0%)] and 17 (56.7%) received TCZ every week [low mCCI: 16 (61.5%); high mCCI: 1 (25.0%)].
Compared with patients with mCCI < 2, patients with mCCI ≥ 2 were older [mean (SD) age, 56.9 (13.1) vs 61.5 (12.3) yrs], more likely to be obese (41.7% vs 52.8%), had a longer mean (SD) disease duration [11.6 (8.9) vs 12.8 (9.9) yrs], and had higher mean (SD) baseline HAQ scores [0.6 (0.5) vs 0.7 (0.6); Table 1A–B,]. Baseline mean CDAI was in the high disease activity range in both subgroups but was higher in patients with a high mCCI [mean (SD) 23.9 (13.9) vs 25.7 (13.4)].
Patient demographics at baseline among patients with low versus high comorbidity burden who initiated TCZ.
Clinical characteristics at baseline among patients with low versus high comorbidity burden who initiated TCZ.
Among patients with a high mCCI score, the mean (SD) mCCI was 2.3 (0.6) and the most common comorbidities were diabetes mellitus (42.6%), solid-tumor cancer (21.0%), liver disease (20.5%), and COPD (10.3%; Supplementary Table 2, available with the online version of this article). The distribution of mCCI among this patient population is shown in Supplementary Table 3. The majority of patients in the high mCCI group (153 patients, 78.5%) had 1 comorbid condition in addition to RA (mCCI = 2), while a smaller number of patients had 2 (34 patients, 17.4%), 3 (3 patients, 1.5%), or 4 (5 patients, 2.6%) comorbid conditions in addition to RA.
Study outcomes by comorbidity burden
The unadjusted analysis of changes in disease activity and HAQ at 6 and 12 months is presented in Table 2. Patients in both comorbidity cohorts had improvement from baseline in CDAI and HAQ at 6 and 12 months, with no significant differences between high versus low mCCI. Similar results were observed in the adjusted analyses (Figure 1); variables are included in Figure 1 legend and included baseline disease activity and baseline functional status. Regarding the primary endpoint, the mean change in CDAI at 6 months was −7.57 for patients with low mCCI and −7.72 for patients with high mCCI. At 12 months, the mean CDAI change was −8.42 for patients with low mCCI and −7.82 for patients with high mCCI (p > 0.05).

Adjusted changes in disease activity and HAQ at 6 and 12 months* after initiation of TCZ in patients with high (mCCI ≥ 2) versus low (mCCI < 2) comorbidity burden. * The 6-month visit occurred in a window of 4–8 months; the 12-month visit occurred in a window of 10–14 months. † A β coefficient < 0 indicates that, on average, patients with high comorbidity burden show a greater level of improvement in the outcome when compared to those with low disease burden, after adjustment for covariates. Additionally, an OR > 1 indicates that patients with high comorbidity burden have higher odds of achieving the outcome compared to those with low disease burden, after adjustment for covariates. Adjustment covariates: age, duration of RA, race, college education, smoking status, alcohol consumption, BMI, work status, insurance type, number of prior csDMARD, current csDMARD use, number of prior biologics used, current prednisone use, CDAI at initiation, HAQ at initiation, patient-reported fatigue at initiation, and duration of morning stiffness at initiation. ‡ CDAI ≤ 10 at baseline, MCID = 2; CDAI > 10 to ≤ 22 at baseline, MCID = 6; CDAI > 22 at baseline, MCID = 11. § MCID = 0.22. ‖ LDA, CDAI ≤ 10. BMI: body mass index; CDAI: Clinical Disease Activity Index; csDMARD: conventional synthetic disease-modifying antirheumatic drug; HAQ: Health Assessment Questionnaire; LDA: low disease activity; mCCI: modified Charlson Comorbidity Index; MCID: minimum clinically important difference; RA: rheumatoid arthritis; TCZ: tocilizumab.
Unadjusted changes in disease activity and HAQ at 6 and 12 months* after initiation of TCZ in patients with low vs high comorbidity burden.
At 6 months, 75.5% of patients with low mCCI and 74.4% of patients with high mCCI were still receiving TCZ (Supplementary Table 1, available with the online version of this article). Among the 364 patients with low mCCI and 124 patients with high mCCI who received IV TCZ and had available dose information at 6 months, 23.6% and 22.6%, respectively, received 4 mg/kg and 76.4% and 77.4%, respectively, received 8 mg/kg. Of the 34 patients with low mCCI and 6 patients with high mCCI who received SC TCZ and had dose frequency information available at 6 months, 47.1% and 66.7%, respectively, received SC TCZ every 2 weeks and 52.9% and 33.3%, respectively, received SC TCZ every week. At 12 months, 61.4% of patients with a low mCCI and 62.6% of those with a high mCCI were still receiving TCZ. Of the 306 patients with low mCCI and 106 patients with high mCCI receiving IV TCZ with available dose information at 12 months, 16% and 18.9%, respectively, received IV TCZ 4 mg/kg, and 84.0% and 81.1%, respectively, received IV TCZ 8 mg/kg. Of the 25 patients with low mCCI and 7 patients with high mCCI who received SC TCZ and had dose frequency information available at 12 months, 56.0% and 71.4%, respectively, received SC TCZ every 2 weeks, and 44.0% and 28.6%, respectively, received SC TCZ every week. The proportions of patients with an increase in IV dose or SC TCZ frequency at 6 and 12 months are shown in Supplementary Table 1 (available with the online version of this article) and were similar between high and low mCCI.
Patient baseline characteristics by BMI
Of the 805 TCZ initiators, 449 (55.8%) were categorized as nonobese [BMI ≤ 30; mean (SD) BMI, 24.9 (3.1) kg/m2], of whom 31 were under-weight (BMI < 18.5), 185 were normal weight (BMI > 18.5 and ≤ 24.9), and 233 were overweight (BMI > 25 and ≤ 29.9). There were 356 patients (44.2%) categorized as obese [BMI > 30; mean (SD) BMI, 36.7 (6.2) kg/m2], of whom 180 were obese class I (BMI > 30 and ≤ 34.9) and 176 were obese class II or III (BMI ≥ 35; Table 3A). A total of 152 obese patients and 2 nonobese patients weighed ≥ 100 kg at baseline (Supplementary Table 4, available with the online version of this article). As shown in Table 3B, > 95% of patients were biologic experienced, and about one-third of patients received TCZ as monotherapy. Most patients [n = 739 (91.8% of all initiators)] were treated with IV TCZ. Of the IV TCZ initiators, 416 (56.3%) were nonobese and 323 (43.7%) were obese; 428 (57.9%) had available dose information at baseline [nonobese: 231 (55.5%); obese: 197 (61.0%)]. Of the IV TCZ initiators with dose available, 243 (56.8%) received 4 mg/kg [nonobese: 127 (55.0%); obese: 116 (58.9%)] and 185 (43.2%) received 8 mg/kg [nonobese: 104 (45.0%); obese: 81 (41.1%); Supplementary Table 5]. Of the 48 (6.0% of all initiators) patients who initiated SC TCZ, 23 (47.9%) were nonobese and 25 (52.1%) were obese. Of the 48 SC TCZ initiators, 30 (62.5%) had baseline dose frequency available [nonobese: 16 (69.6%); obese: 14 (56.0%)]. Of these, 13 (43.3%) received TCZ every 2 weeks [nonobese: 8 (50.0%); obese: 5 (35.7%)] and 17 (56.7%) received TCZ every week [nonobese: 8 (50.0%); obese: 9 (64.3%)].
Patient demographics at baseline in nonobese versus obese patients who initiated TCZ.
Clinical characteristics at baseline in nonobese vs obese patients who initiated TCZ.
Compared with nonobese patients, obese patients were younger [mean (SD) age, 56.7 (12.0) vs 59.0 (13.7) yrs], had a shorter mean (SD) disease duration [11.4 (8.6) vs 12.6 (9.7) yrs], had higher mean (SD) baseline HAQ [0.7 (0.5) vs 0.6 (0.5)] scores, higher mean (SD) mCCI scores [1.4 (0.7) vs 1.3 (0.6)], and worse mean (SD) patient-reported fatigue scores [55.9 (28.3) vs 50.6 (28.5); Table 3A–B]. Baseline mean CDAI was in the high disease activity range in both subgroups but was higher in patients who were obese [mean (SD): 25.4 (14.3) vs 23.6 (13.4)].
Study outcomes by BMI
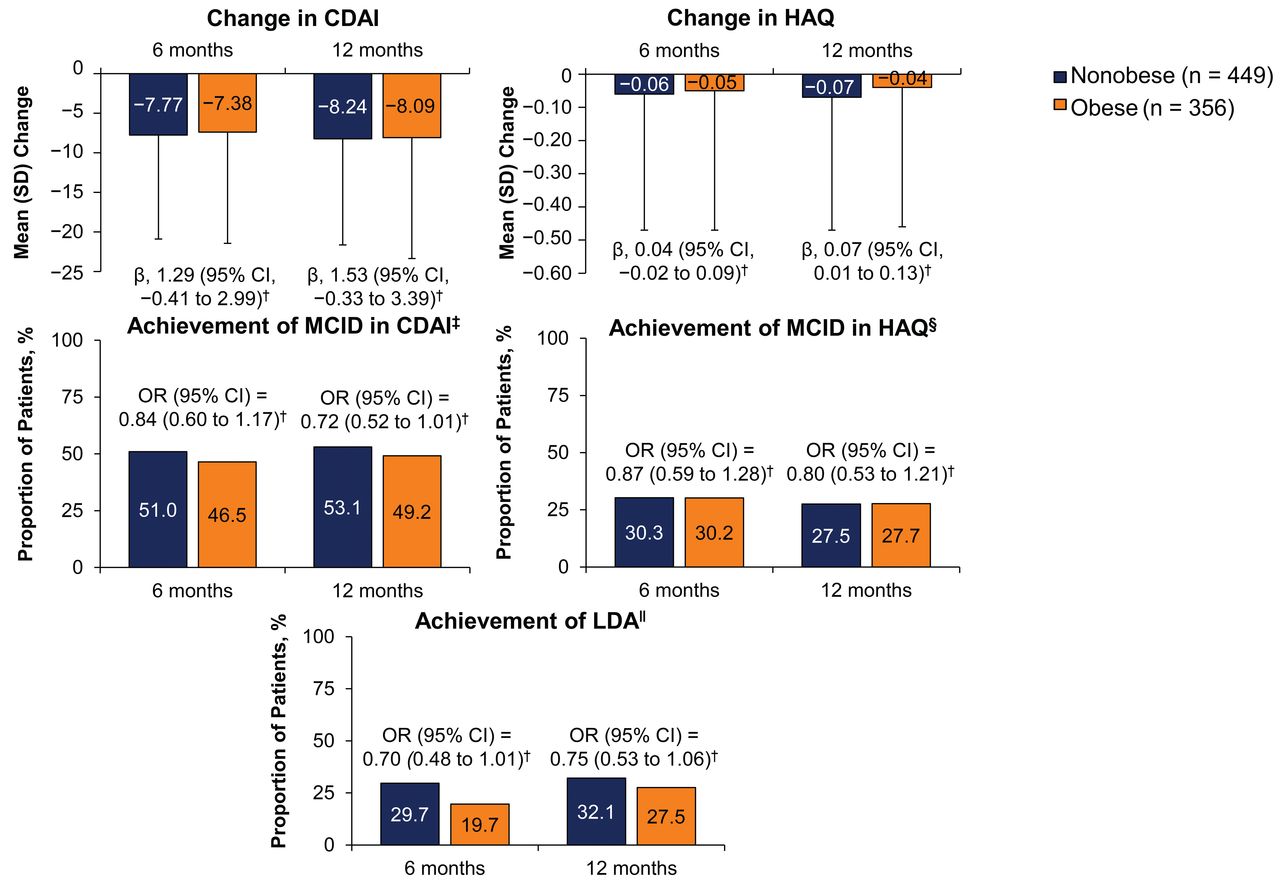
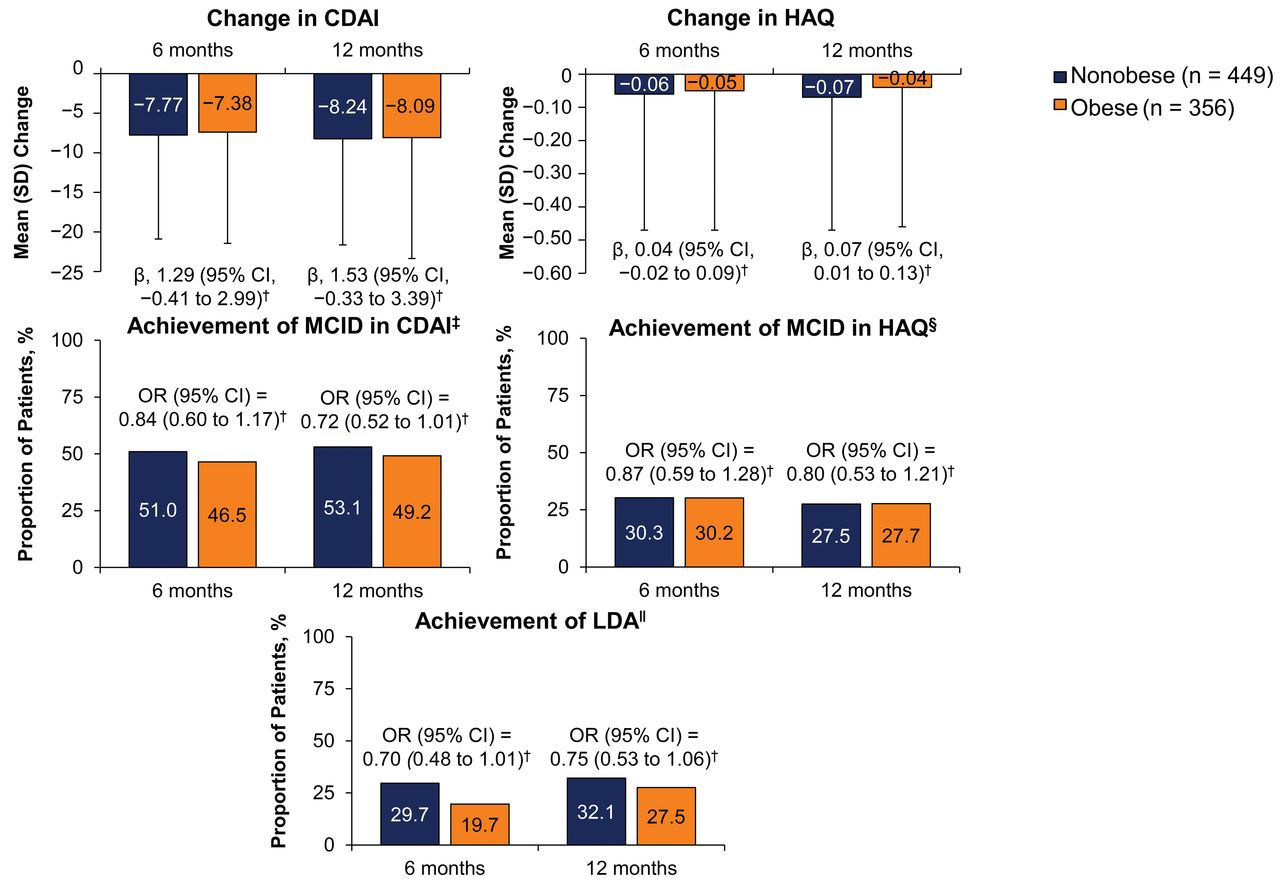
The unadjusted analyses of changes in disease activity and HAQ at 6 and 12 months are shown in Table 4. Patients in both obesity cohorts had comparable improvement from baseline in CDAI and HAQ at 6 and 12 months. Similar results were noted in adjusted analyses (Figure 2). The variables for which the regression models were adjusted are included in the legend of Figure 2 and included baseline disease activity and baseline functional status. Regarding the primary outcome, the mean change in CDAI at 6 months was −7.77 for nonobese patients and −7.38 for obese patients, and at 12 months was −8.24 for nonobese patients and −8.09 for obese patients (p > 0.05). Only HAQ improvement reached statistical significance between the groups at 12 months, in favor of nonobese patients; however, the β coefficient was below the reference MCID for HAQ (0.11).
{kind=link}
{kind=link}
Adjusted changes in disease activity and HAQ at 6 and 12 months* after initiation of TCZ in obese (BMI ≥ 30) versus nonobese (BMI < 30) patients. * The 6-month visit occurred in a window of 4–8 months; the 12-month visit occurred in a window of 10–14 months. † A β coefficient < 0 indicates that, on average, obese patients show a greater level of improvement in the outcome when compared to nonobese patients, after adjustment for covariates. Additionally, an OR > 1 indicates that obese patients have higher odds of achieving the outcome compared to nonobese patients, after adjustment for covariates. Adjustment covariates: age, duration of RA, race, college education, smoking status, alcohol consumption, BMI, work status, insurance type, number of prior csDMARD, current csDMARD use, number of prior biologics used, current prednisone use, CDAI at initiation, HAQ at initiation, patient-reported fatigue at initiation, and duration of morning stiffness at initiation. ‡ CDAI ≤ 10 at baseline, MCID = 2; CDAI > 10 to ≤ 22 at baseline, MCID = 6; CDAI > 22 at baseline, MCID = 11. § MCID = 0.22. ‖ LDA, CDAI ≤ 10. BMI: body mass index; CDAI: Clinical Disease Activity Index; csDMARD: conventional synthetic disease-modifying antirheumatic drug; HAQ: Health Assessment Questionnaire; LDA: low disease activity; MCID: minimum clinically important difference; RA: rheumatoid arthritis; TCZ: tocilizumab.
Unadjusted changes in disease activity and HAQ at 6 and 12 months* after initiation of TCZ in nonobese versus obese patients.
At 6 months, 76.2% of nonobese patients and 73.3% of obese patients were still receiving TCZ (Supplementary Table 5, available with the online version of this article). Among the 288 nonobese patients and 221 obese patients who received IV TCZ and had available dose information at 6 months, 21.2% and 26.7%, respectively, received 4 mg/kg, and 78.8% and 73.3%, respectively, received 8 mg/kg. Of the 23 nonobese patients and 18 obese patients who received SC TCZ and had dose frequency information available at 6 months, 56.5% and 38.9%, respectively, received SC TCZ every 2 weeks and 43.5% and 61.1%, respectively, received SC TCZ every week. At 12 months, 63.9% of nonobese patients and 58.1% of obese patients were still receiving TCZ. Of the 245 nonobese patients and 184 obese patients receiving IV TCZ with available dose information at 12 months, 15.9% and 17.4%, respectively, received IV TCZ 4 mg/kg and 84.1% and 82.6% received IV TCZ 8 mg/kg. Of the 26 nonobese patients and 7 obese patients who received SC TCZ and had dose frequency information available at 12 months, 57.7% and 57.1%, respectively, received SC TCZ every 2 weeks and 42.3% and 42.9%, respectively, received SC TCZ every week. The proportions of patients with an increase in IV TCZ dose or SC TCZ frequency at 6 and 12 months are shown in Supplementary Table 5 and were similar for obese and nonobese patients.
DISCUSSION
The high prevalence of comorbidities1,21 and of obesity7 in patients with RA and the association between comorbidity and RA disease progression22 have led to extensive investigation into the potential effect of comorbid conditions and of obesity on disease-modifying antirheumatic drug (DMARD) efficacy. Patients with a higher comorbidity burden may be less likely to start a biologic agent early in their disease course21. Obesity has also been associated with poorer clinical outcomes in patients with RA, despite DMARD therapy, and efficacy of tumor necrosis factor inhibitors is negatively affected by patients’ weight10,12,13,16,23,24,25. The effect of TCZ in patients with higher comorbidity burden has not previously been evaluated in patients with RA. Also, few real-world studies have investigated the effectiveness of TCZ in obese patients26,27. Using data from the largest US-based RA registry, we demonstrated that patients who initiated TCZ improved in CDAI and HAQ at 6 and 12 months, with similar improvements in patients with high and low comorbidity burden and obese and nonobese patients.
The current study provides insight into TCZ use in real-life practice in the United States. We found TCZ is frequently used in patients with comorbidities and obesity, as 25% of TCZ initiators in our study had a high mCCI and 45% were categorized as obese. More than 95% of the patients included in our analysis had failed other biologics prior to TCZ initiation. The vast majority of patients received IV TCZ, and most patients were treated with IV TCZ 8 mg/kg at 6 months post-initiation. Patients in the Corrona registry are not mandated to receive a specific therapeutic regimen. Instead, treatment decisions related to the choice of medication as well as changes in dosage and frequency rely on the physician’s discretion. The fact that IV TCZ is administered on a mg/kg basis may have allowed rheumatologists to more easily tailor TCZ dose based on patients’ weight or lack of response to the recommended initial dosing of 4 mg/kg every 4 weeks (increasing to 8 mg/kg based on clinical response). Thus, the dose flexibility of TCZ may have improved disease control in patients who would have been nonresponders if treated with a biologic not adjusted for body weight.
The major strength of this study was the use of a large US database collecting real-world data on clinical response in patients, along with BMI and comorbid conditions. Although previously published studies investigating TCZ in obese patients with RA have similarly shown no difference in clinical response compared to nonobese patients26,27, a recent report showed impaired improvement in 28-joint count Disease Activity Score in women with RA treated with TCZ28. Our present study expands upon previous findings to present data from patients in the United States and to describe changes in CDAI and HAQ in a larger sample of patients.
There are several notable points to consider in the interpretation of our findings. The distribution of mCCI indicates that the majority of patients in this analysis with mCCI ≥ 2 had 1–2 comorbidities plus RA. TCZ effectiveness was not separately analyzed for patients with > 2 comorbidities, and the relationship between specific comorbidities on TCZ efficacy was not examined. The effectiveness of TCZ in patients with extreme obesity or with weight > 100 kg, populations who would be more likely to receive the maximum dose of TCZ (162 mg weekly for SC TCZ and 800 mg/kg every 4 weeks for IV TCZ), was not separately examined. Thus, these results should be interpreted with caution for patients with multiple comorbidities or extreme obesity. The mCCI does not include all comorbidities in patients with RA (e.g., interstitial lung disease), and it is possible some patients in the low comorbidity burden group may have had a comorbidity that was not recorded by the mCCI; however, the CCI has been extensively validated and has shown strong correlation with other comorbidity indices in patients with RA29. Baseline TCZ dose information was available for only about 57% of patients, resulting in an insufficient sample size for meaningful comparison of TCZ effectiveness stratified by dose in low versus high comorbidity burden or in nonobese versus obese groups. Because most patients received IV TCZ, our results may not be generalizable to SC use. The sample size of patients receiving SC TCZ was not sufficient to generate meaningful results in a separate analysis — only 47 of the 770 TCZ initiators included in the analysis of comorbidity burden and 48 of the 805 TCZ initiators included in the analysis of obesity initiated SC TCZ. However, clinical studies have demonstrated no difference in the efficacy of SC TCZ compared with IV TCZ for improving disease activity in patients with RA30,31. Thus, our results may provide relevant information for patients treated with SC TCZ. Regarding the missing dose information on the robustness of our results, our study was not undertaken to establish the effectiveness of a specific TCZ dose in the setting of obesity or comorbidities. While the dose information data are incomplete, they still reflect the actual use of TCZ in the registry. The percentage of missing data by TCZ dose was not different by obesity or comorbidity status. The distribution of IV TCZ 4 versus 8 mg/kg dose at baseline is also balanced between the cohorts, and similar patterns are noted for the percentage of patients who increase their IV TCZ dose from 4 to 8 mg/kg at 6 and 12 months. Therefore, the lack of dosing data was not believed to preferentially skew the results in favor of patients with high or low comorbidities or BMI. The overwhelming use of IV TCZ in the United States is 8 mg/kg, and because 93.8% of the patients were receiving IV TCZ in our study, these findings appear representative of patients receiving TCZ in real-world situations.
This analysis demonstrates that TCZ is used frequently in real-world practice in patients with RA with comorbid conditions or obesity and was effective regardless of comorbidity burden or obesity.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
Support for third-party writing assistance for this manuscript, furnished by Health Interactions Inc., was provided by Genentech, Inc.
Footnotes
Full Release Article. For details see Reprints and Permissions at jrheum.org
This study is sponsored by Corrona, LLC. Corrona, LLC has been supported through contracted subscriptions in the last 2 years by AbbVie, Amgen, Bristol-Myers Squibb, Crescendo, Eli Lilly and Co., Genentech, GSK, Horizon Pharma USA, Janssen, Momenta Pharmaceuticals, Novartis, Pfizer, Roche, and UCB. The study design and conduct were the result of a collaborative effort between Corrona, LLC and Genentech, Inc., and financial support for the study was provided by Genentech, Inc., which manufactures tocilizumab. Genentech, Inc. participated in the interpretation of data, review, and approval of the manuscript. All authors had full access to all the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis.
D.A. Pappas is an employee of Corrona, LLC, a consultant for AbbVie, and has received grant support from AbbVie. C.J. Etzel is an employee and shareholder of Corrona, LLC, and is a member of an advisory board for Merck. M. Crabtree is an employee of Corrona, LLC. J. Best and S. Zlotnick are employees and shareholders of Genentech, Inc. J.M. Kremer is an employee and shareholder of Corrona, LLC, and a consultant for AbbVie, Amgen, Bristol-Myers Squibb, Genentech, GlaxoSmithKline, Lilly, Pfizer, Regeneron, and Sanofi.
- Accepted for publication December 12, 2019.
Free online via JRheum Full Release option
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.