
Abstract
Objective. A systematic literature review was performed to document published magnetic resonance imaging (MRI) lesion definitions and scoring systems for enthesitis in spondyloarthritis (SpA).
Methods. PubMed, Embase, and Cochrane Library databases were searched for original publications involving adult patients with SpA undergoing MRI of axial/peripheral joints. Selected articles were assessed for quality using a standardized assessment tool and metric indices.
Results. Considering the heterogeneous design, quality, and outcome measures of studies, statistical data pooling was considered inappropriate. A qualitative narrative of results was undertaken based on study designs.
Conclusion. Lack of a comprehensive, validated score warrants additional research to develop an MRI enthesitis scoring system. PROSPERO registration number: CRD42018090537.
- ENTHESOPATHY
- MAGNETIC RESONANCE IMAGING
- SPONDYLOARTHROPATHY
- INFLAMMATION
- OMERACT
Enthesitis, inflammation at the insertion site of tendon, ligament, or joint capsule into bone, is considered a key pathological feature in spondyloarthritis (SpA) and psoriatic arthritis (PsA)1. Compared to conventional assessment of enthesitis using clinical scores, magnetic resonance imaging (MRI) detects both soft tissue and intraosseous abnormalities in active enthesitis, potentially aiding early diagnosis and outcome measurement in SpA and PsA2. With the advent of the treat-to-target concept and novel therapies, objective and sensitive monitoring of response of enthesitis to therapy is desirable, and a validated MRI scoring system would be a useful adjunct to clinical practice as well as providing additional information as an outcome measure in clinical trials.
The Outcome Measures in Rheumatology (OMERACT) MRI in Inflammatory Arthritis Working Group undertook a systematic literature review to describe the MRI variables, definitions, and scoring systems used to diagnose and monitor enthesitis in SpA. We assessed the quality and reported psychometric qualities, including validity, reliability, and responsiveness of original publications, to understand whether there was a need for a novel MRI scoring system for enthesitis in SpA3,4.
MATERIALS AND METHODS
Selection criteria and search strategies
We searched Medline, Embase, and Cochrane Library databases from their inception until February 2018 for original publications involving adult patients (> 18 yrs) with SpA in whom MRI of axial or peripheral joints had been performed using a high-field magnet (≥ 1.5T) to assess enthesitis. Exclusion criteria included studies on enthesitis related to other conditions, such as degenerative, trauma-related, and inflammatory diseases other than SpA. The search strategy was designed to select cross-sectional, case control, randomized controlled, and nonrandomized studies in the English language containing at least 1 term from each of the following search blocks: (1) spondyloarthritis, spondylarthritis, psoriatic arthritis, or ankylosing spondylitis; (2) enthesopathy, enthesitis or enthesis; and (3) magnetic resonance imaging or MRI. The selected studies were evaluated for definitions of MRI enthesitis lesions, quality of studies using a standardized assessment tool, and for their metric qualities.
Selection of studies and data extraction
Two reviewers (AJM and SK) independently selected the studies and systematically screened the titles and abstracts, applying inclusion and exclusion criteria. Selected articles were retrieved in full, and the same reviewers assessed each article for its eligibility. Disagreements between the reviewers on article selection were resolved by discussion. Data were extracted to a standardized form. Any discordance in opinion was resolved by consensus and involvement of a third reviewer (MØ). The data extraction sheet contained the following information: author, year of publication, study design, study population, number of participants, intervention, comparator, MRI field strength, sequences used, MRI sites used for evaluating enthesitis, definitions of MRI inflammatory and structural enthesitis, and scoring system used (Table 1).
Characteristics of included studies.
Quality assessment of selected studies
A standardized tool (Supplementary Table 1, available with the online version of this article) for quality assessment of the analyzed studies based on a set of 12 predefined criteria addressing the following components was developed and assessed in a binary mode (yes/no): study population, enthesitis imaging feature, outcome of interest, study design and analysis, and data presentation. Concepts from review of quality assessment tools in systematic reviews of observational studies were adapted for developing these criteria5. Quality was reported on a scale of 0–12, with higher scores indicating better quality. Included studies that scored < 3 on the scale were excluded from the final analysis.
Psychometric properties of included studies
Each selected article was analyzed and assessed to determine whether it satisfied certain aspects of validity. The following metric qualities were evaluated: face and content validity, construct validity, criterion validity, and discriminant validity (reliability and responsiveness; Table 2).
Psychometric properties and quality scores of selected studies (n = 38).
Statistical analysis
Details of the studies were reported with descriptive statistics such as frequencies and percentages for categorical data and mean and SD for continuous data. Because of variability in studies, metaanalysis could not be performed. PROSPERO registration number: CRD42018090537.
RESULTS
Literature search
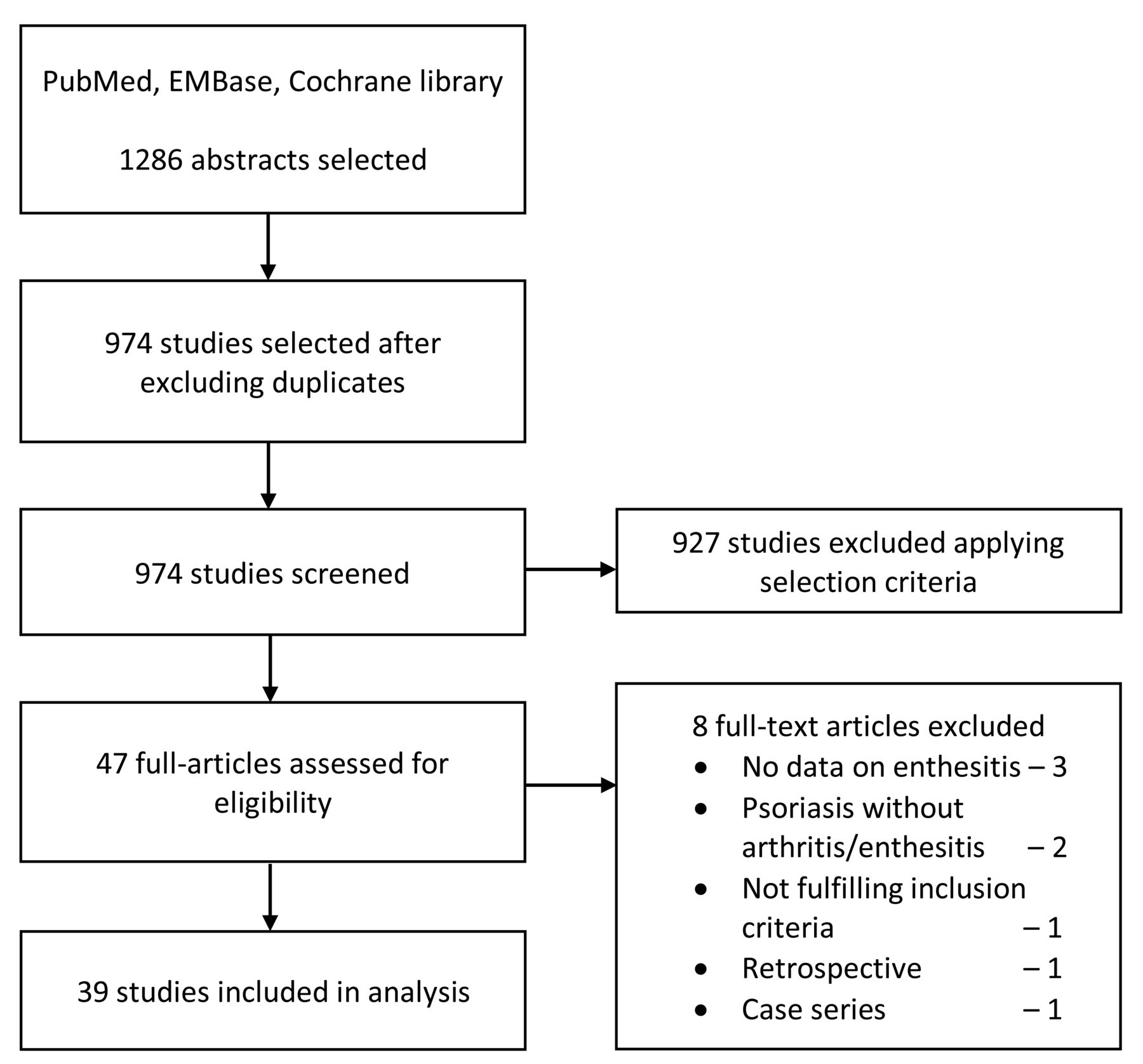
The study selection process is depicted in a PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) flow diagram (Figure 1).
{kind=link}
Flow diagram of article selection (PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses).
Study characteristics
Attributes of the included studies are summarized in Table 12,6–43. The majority of included studies were of cross-sectional design (20; 51%)2,6–17,19–24,28. Eight case-control18,25–27,29–32, 6 cohort33,34,35,36,37,38, 3 randomized controlled trials39,40,41, and 2 other longitudinal studies42,43 were included. Study populations involved SpA in 22, ankylosing spondylitis in 7, and PsA in 9 studies, and chronic low back pain in 1 study. In total, 1534 individuals (range 8–127) in different groups were evaluated for MRI enthesitis in all the studies together. Peripheral enthesitis were evaluated in 24 (62%) studies7,10,11,15–29,31,32,34,36,38,39, axial enthesitis in 8 studies6,8,12,15,14,36,42,43, and enthesitis at both sites using whole-body MRI in 7 studies2,9,30,33,37,40,41. Both T1-weighted (T1w) and T2w fat-suppressed or its comparable sequences were included in all the studies. Comparison with other methods of evaluating enthesitis [ultrasonography (US) and clinical assessment] was described in 10 studies7,9,10,11,18,30,31,32,35,36, while 5 studies compared different MRI sequences to assess enthesitis6,13,14,25,42. Only 4 studies compared efficacy of MRI against a gold standard11,13,35,42.
Qualitative assessment of enthesitis at different regions was used in 82% of studies. Only 8 studies mentioned a semiquantitative or quantitative MRI scoring system2,14,16,17,19,25,39,40. No studies described a validated, comprehensive MRI scoring system measuring all the aspects of enthesitis in any region. The majority of studies defined inflammatory enthesitis as enhancement of ligaments, increased signal intensity, perientheseal increased signal intensity, adjacent bone marrow edema (BME), soft tissue signal around ligaments or tendons, thickening of ligaments, capsulitis in sacroiliac joints, extracapsular soft tissue enhancement, Achilles tendon diameter of BME, perientheseal fluid and/or tendinitis in T1w post-gadolinium, or short-tau inversion recovery sequences. Entheseal structural damage defined by few studies includes bone erosions, enthesophytes, focal signal intensity changes, and calcaneal spur in T1w sequences2,7,16,25,27,28,29,32.
Quality assessment of included studies
Quality scores assessed using a standardized tool are provided in Table 2. With 1 exception, all 38 studies met the minimal quality requirement score of 4. High quality scores (10–12) were present in only 2 studies2,40, while the remaining 36 studies had moderate quality scores (5–9).
Assessment of psychometric properties
Table 2 describes psychometric properties of the selected studies. Face validity was assessed in 33 (87%) studies, content validity in 19 (50%) studies, and construct validity of MRI as related to ultrasound (US) and clinical examination in 5 (13%) and 6 (16%) studies, respectively. Five studies reported construct validity of different MRI sequences in relation to each other6,13,14,25,42. Criterion validity of MRI in relation to histology was described only by Tan, et al22. Reliability of MRI in detecting enthesitis using various scoring methods was reported by 26 (68%) studies in which images were evaluated by 2 independent readers who were blinded to clinical outcomes. Responsiveness of various MRI enthesitis scores was reported in 6 (18%) studies, of which 3 showed statistically significant changes (p < 0.05)37,40,41.
DISCUSSION
Axial and peripheral enthesitis constitutes a core feature of SpA and PsA. The OMERACT PsA core domain set includes enthesitis, which makes it mandatory to be assessed in all clinical trials and observational studies44. MRI allows sensitive assessment of enthesitis in clinical trials. We have critically evaluated the published literature for available methods of evaluating enthesitis using MRI in patients with SpA and PsA, and identified notable limitations regarding standardization of MRI enthesitis definitions across studies and validity of available semiquantitative scores as outcome measures. The findings suggest there is no currently available reliable and validated MRI scoring system for enthesitis. Many studies have included different definitions of MRI lesions suggestive of enthesitis, hindering direct comparison of the available methods. A fifth of the selected studies described a semiquantitative scoring system, albeit without standardization and internal validity, because all were developed based on expert opinion.
Poor content validity of reported scoring methods was another limitation of the literature. Most studies have focused on assessing inflammatory aspects of enthesitis and not the structural variables, which denote chronic, irreversible changes. MRI inflammatory lesions are amenable to change and responsive to therapy. Wide variation in the entheseal sites to be assessed adds to the challenge in standardization. Lack of a standardized definition to define the borders of enthesitis makes it difficult to differentiate it from other inflammatory variables, such as synovitis and tenosynovitis, thus increasing the variability of scores in each study.
Construct validity was evaluated in relation to US and clinical examination. Most of the studies showed poor correlation between MRI and US. This again emphasizes the lack of standardized definitions of MRI enthesitis lesions. Limited information exists regarding criterion validity because only 1 study compared MRI with histology. Lack of significant responsiveness of available qualitative and semiquantitative MRI enthesitis scores suggests limited utility as outcome measures in clinical trials.
The above-mentioned limitations and the lack of validated, generally accepted MRI enthesitis assessment systems warrant the development of a reliable and feasible MRI enthesitis scoring system to increase the utility of MRI as an outcome measure in SpA and PsA clinical trials.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
AJB and PGC are supported in part through the NIHR Leeds BRC. The views expressed in this article are those of the authors and not necessarily those of the NHS, the NIHR, or the UK Department of Health.
- Accepted for publication January 9, 2019.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.