
Abstract
Objective. We evaluated the associations between time-varying methotrexate (MTX) use and risk of cardiovascular events (CVE) in patients with rheumatoid arthritis (RA).
Methods. We studied an inception cohort of 23,994 patients with RA diagnosed after their 65th birthday. Multivariable Cox regression models were fit to evaluate the associations between time-varying MTX use, controlling for other risk factors, and time to CVE. Alternative models assessed the cumulative duration of MTX use over the (1) first year, (2) previous year (recent use), and (3) entire duration of followup. We also assessed whether the strength of the association varied over time.
Results. Over 115,453 patient-years (PY), 3294 (13.7%) patients experienced a CVE (28.5 events per 1000 PY; 95% CI 27.6–29.5). In the multivariable analyses, the model assessing time-varying continuous use in the most recent year yielded the best fit. Increasing recent MTX use was associated with lower CVE risks (HR 0.79 for continuous use vs no use in past 12 months, 95% CI 0.70–0.88; p < 0.0001). Greater MTX use in the first year after cohort entry was also protective (HR 0.84, 95% CI 0.72–0.96; p = 0.0048), but this effect decreased with increasing followup. In contrast, longer MTX use during the entire followup was not clearly associated with CVE risk (HR 0.98, 95% CI 0.95–1.01; p = 0.1441).
Conclusion. We observed about a 20% decrease in CVE associated with recent continuous MTX use. Greater MTX use in the first year of cohort entry also appeared to be important in the association between MTX and CVE risk.
- RHEUMATOID ARTHRITIS
- CARDIOVASCULAR DISEASE
- METHOTREXATE
- DISEASE-MODIFYING ANTIRHEUMATIC DRUGS
High cardiovascular morbidity is an unfortunate reality in rheumatoid arthritis (RA)1,2,3,4,5,6. Chronic high-grade systemic inflammation has been implicated in promoting atherogenesis and increased cardiovascular morbidity7,8,9,10. Thus, conventional synthetic disease-modifying antirheumatic drugs (csDMARD), which target inflammation, could influence atherogenesis and therefore cardiovascular risk in patients with RA.
A metaanalysis of 8 studies reported a 28% reduction in the risk of cardiovascular events (CVE) associated with methotrexate (MTX) use in patients with RA (RR 0.72, 95% CI 0.57–0.91)11. However, many of the underlying studies were heterogeneous and failed to account for the duration or timing of treatment exposure; rather MTX exposure was defined as a binary indicator of ever/never use, current use, or a baseline covariate12,13. In clinical practice, duration and timing of exposure to MTX and other csDMARD varies considerably within and among individual patients over time14. The potential beneficial effects of MTX and other csDMARD also may vary over time. For example, patients with greater early MTX use may require less MTX later. Conversely, some patients may use MTX in a consistent manner throughout their disease course, but initiate late, and the therapeutic window of opportunity may be missed15. Thus, patients with early intensive treatment and/or those who recently had persistent use of MTX will have a greater likelihood of obtaining a low disease activity state16 and thereby reducing systemic inflammation, which could offer greater potential for reducing CVE risk17.
Our aim was to assess the associations between time-varying use of MTX and other csDMARD and CVE risk to determine whether the effects vary by timing, recency, and duration of use, and whether effects vary over time.
MATERIALS AND METHODS
Study design
Using health administrative data in Ontario, Canada, we studied an inception cohort of patients with RA to examine the effects of time-varying RA treatment, controlling for other risk factors, on the risk of CVE. Our analyses were confined to persons aged 66 years or older for whom we had complete prescription drug histories (because the age cutoff for public drug coverage is 65 years and older; however, there may be delays in transitioning into public drug coverage).
Data sources
We used the Ontario Health Insurance Plan (OHIP) Claims History Database to identify diagnoses and procedures associated with physician services. We identified patient demographic information and vital status from the OHIP Registered Persons Database. Medication exposures were determined using the pharmacy claims database of the Ontario Drug Benefit Program. Hospital admissions and procedures were identified using the Canadian Institute for Health Information Discharge Abstract Database. These datasets are held securely in a linked coded form at the ICES. The study was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which means it did not require approval by a research ethics board.
Cohort selection
We identified patients with RA within the Ontario Rheumatoid Arthritis Dataset18. Our analyses were confined to individuals who had at least 3 physician service claims with an RA diagnosis (with at least 1 provided by a musculoskeletal specialist) within 2 years. This algorithm has about 80% sensitivity and positive predictive value for physician-diagnosed RA19. We defined the cohort entry date as the date when all criteria were met. Patients were required to be newly diagnosed after their 66th birthday (to ensure complete medication records after disease onset) between January 1, 2000, and March 1, 2013. Thus, patients were excluded if they had RA prior to their 66th birthday. Patients were excluded if they had missing demographic information, or were hospitalized or dead on the cohort entry date.
Outcome
The primary study outcome was a composite endpoint defined as the incidence of hospitalization for acute myocardial infarction (AMI), stroke, or congestive heart failure, or either percutaneous coronary intervention or coronary artery bypass graft surgery. Diagnosis and procedure codes (Supplementary Table 1, available with the online version of this article) used to define these events have been validated in Ontario and deemed to have a high specificity20,21,22,23,24.
Time-dependent medication exposures
The main exposures of interest were MTX and other csDMARD (azathioprine, sulfasalazine, gold, chloroquine, hydroxychloroquine, leflunomide, cyclosporine, minocycline, penicillamine, myochrysine, and cyclophosphamide), with nonuse as the referent category. We constructed a daily medication exposure matrix for each patient, incorporating each prescription start date, number of pills, dosage, and days supplied25. On this basis, we calculated a time-dependent, daily measure of cumulative duration of use of a specific medication, or class of medications, until a given day during the followup period26. The following assumptions were applied: for overlapping prescriptions of the same drug, we assumed the individual to have refilled early and completed the first prescription before starting the second. The same rule was applied to overlapping prescriptions of the same medication but with different doses and overlapping prescriptions for different medications within the same medication class. For combination use of csDMARD, prescriptions for each class of csDMARD were treated separately. When there was a gap of 7 days or fewer between 2 prescriptions of the same medication, or of different medications within the same class (excluding csDMARD), it was assumed that the medication was taken continuously and the gap was filled with the daily dose of the second prescription.
Using the same method, we also adjusted for time-varying cumulative duration of use of other medications since cohort entry: anti–tumor necrosis factor (anti-TNF) inhibitors, other biologic DMARD, cyclooxygenase-2 inhibitors (COXIB), nonselective nonsteroidal antiinflammatory drugs (NSAID), systemic glucocorticosteroids, statins, and antihypertensives.
Baseline medication exposures
We also identified binary time-invariant indicators of baseline exposures to MTX, other csDMARD, anti-TNF inhibitors, COXIB, NSAID, glucocorticosteroids, statins, and antihypertensives, defined as any prescription for the corresponding medication during the 1 year prior to cohort entry.
Other covariates
Potential risk factors and confounders for the association between the medications of interest and CVE were selected a priori. Sociodemographic variables included sex, age at cohort entry (in years and with a squared-age term added to account for nonlinear effects), place of residence (urban or rural, defined from postal codes), and regional socioeconomic status (income quintiles derived from census data). Baseline comorbidity was based on the 3 years prior to cohort entry, using diagnosis codes from all outpatient and hospital visits, and included hypertension, diabetes, cerebrovascular disease, acute renal failure, chronic kidney disease, prior AMI, coronary artery disease, chronic obstructive pulmonary disease or asthma, cancer, osteoarthritis, and prior joint replacement surgery (Supplementary Table 2, available with the online version of this article). To adjust for severity of baseline illness, we used the Johns Hopkins ACG System (version 10) case-mix adjustment system. To discriminate between higher and lower users of the healthcare system, we adjusted for a binary indicator of high use, defined as at least 20 physician visits during at least 1 year of the 3 years before baseline. As proxies for disease severity27, we used a time-varying number of rheumatologist visits (log-transformed because of a skewed distribution) and time-varying indicators for the development of extraarticular RA manifestations, including lung involvement (pleurisy, pulmonary fibrosis, rheumatoid lung, interstitial lung disease), hematological involvement (Felty syndrome), cardiac involvement (rheumatic carditis, endocarditis, myocarditis, pericarditis), eye involvement (scleritis, keratoconjunctivitis), dermatological complications (vasculitis, pyoderma gangrenosum), entrapment syndromes, neuropathies, and amyloidosis.
Statistical analysis
All primary analyses relied on time-to-event methodology. Time-to-event was defined as time from cohort entry to CVE. Subjects who had no CVE during followup were censored at the earliest of the dates of emigration, non-CVE death, or the end of the study period (December 31, 2015). The CVE incidence rate was estimated using the total person-time accumulated from cohort entry as the denominator.
Three separate time-dependent multivariable Cox proportional hazards models were fit to estimate adjusted HR and 95% CI for the associations between model-specific time-varying measures of the cumulative past duration of RA medication exposures and time to CVE. All models estimated separate, mutually adjusted associations with MTX and other csDMARD, and controlled for all aforementioned covariates.
Model A assessed the cumulative duration of use of MTX, and other csDMARD, in the first year after cohort entry only. These exposure measures were updated during the first year and then kept constant for the rest of followup. For Model B, the exposure, at any timepoint in the followup, was defined as the cumulative use in the past 12 months. Finally, Model C assessed the cumulative duration of past use since cohort entry. In models B and C, exposures were continuously updated during the followup. We compared the Akaike information criterion (AIC) values for the alternative exposure models, with a reduction in AIC of 4 points or more indicating an improved model fit28.
For each model, the proportional hazards assumption was assessed by testing the time-varying interaction between MTX use and followup time29. A statistically nonsignificant interaction (p > 0.05) was interpreted as lack of evidence that the strength of the association varies with followup29.
In sensitivity analyses, all 3 models were expanded to include an interaction term between the corresponding measures of the cumulative effects of MTX and other csDMARD. The interaction was tested to determine whether the associations of interest differed depending on the use of the other medication class (MTX and csDMARD categories), and was removed from the final model if not statistically significant at α = 0.05 for a 2-tailed model-based Wald test30.
In a final sensitivity analysis, we excluded patients who had preexisting coronary artery disease or cerebrovascular disease prior to cohort entry.
All analyses were performed using SAS Enterprise Guide 6.1.
RESULTS
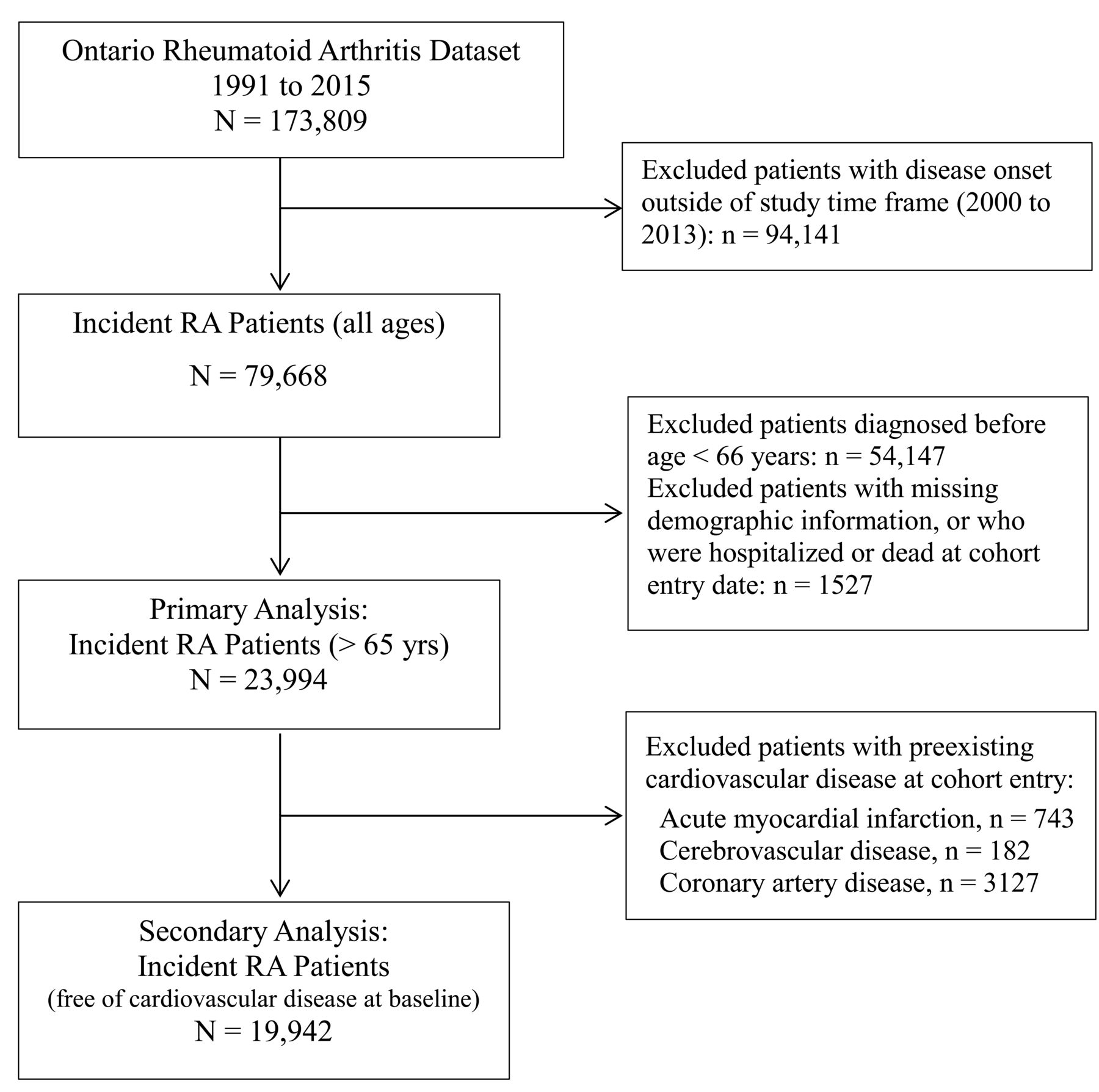
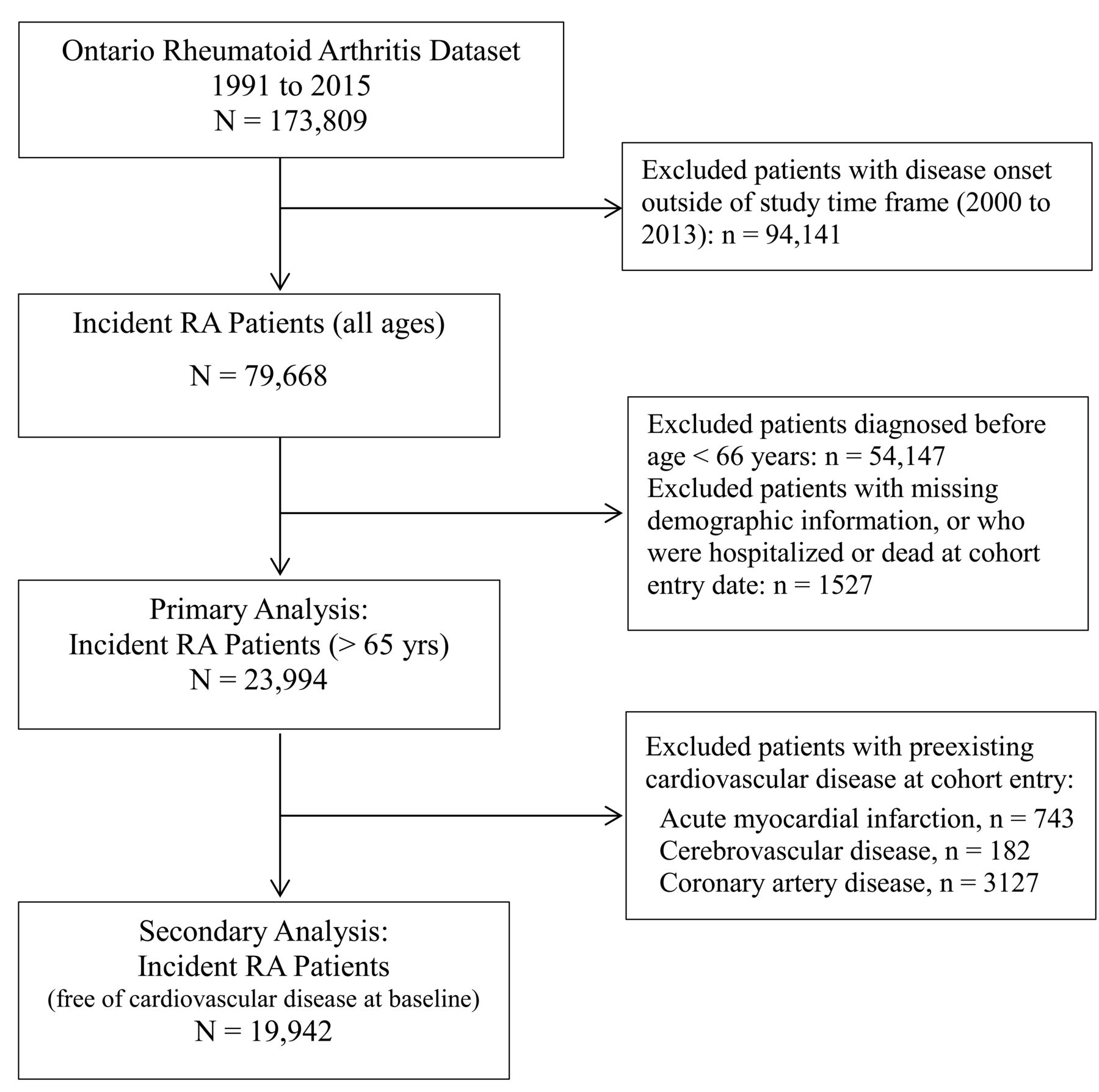
A schematic representation of the cohort selection is detailed in Figure 1.
{kind=link}
Schematic representation of the process used to select patients for inclusion in the final cohort. RA: rheumatoid arthritis.
Among 23,994 incident patients with RA, two-thirds were female (67%) and mean age was 75 years. Patients had a high CVE risk burden at cohort entry (70% had preexisting hypertension, 23% diabetes, 16% coronary artery disease, 3% previous AMI, and 1% cerebrovascular disease; Table 1). Within the year prior to cohort entry, immune-modulating drug use included glucocorticosteroids (57%), other csDMARD (36%), and MTX (32%). During followup, 50% of patients had at least 1 prescription for MTX, 54% for other csDMARD, and 68% for glucocorticosteroids (Table 2).
Baseline characteristics of 23,994 incident patients with RA.
Baseline and followup medication exposures.
During the total of 115,453 patient-years (PY) of followup, 3294 patients (13.7%) experienced a CVE (28.5 events per 1000 PY; 95% CI 27.6–29.5).
In the adjusted multivariable analyses, Model B assessing time-varying duration of use in the most recent year of followup yielded the best fit (lowest AIC, Table 3). Continuous MTX use in the past 12 months was associated with 20% CVE risk reduction (adjusted HR 0.79, 95% CI 0.70–0.88, p < 0.0001) relative to those who did not use any MTX in the past year (Table 3). This association was reasonably constant over followup (p = 0.086 for testing the proportional hazards hypothesis), with a minor trend to become weaker over time (data not shown).
Comparison of 3 different time-varying measures.
In Model A, early MTX use, in the first year after cohort entry, was also protective (HR 0.84, 95% CI 0.72–0.96, for full year of use vs no use, p = 0.005), but a statistically significant interaction with time suggested this effect weakens with increasing followup duration (p = 0.033).
In contrast, in Model C greater cumulative duration of past MTX use since cohort entry had no association with CVE risk (HR 0.98, 95% CI 0.95–1.01 for each additional year of past use, p = 0.144), and this model yielded the worst fit to data (Table 3).
In all 3 models, the different time-varying exposures for other csDMARD were not systematically associated with CVE risks (Table 3).
Sensitivity analyses identified no statistically significant interactions between corresponding exposures to the 2 classes of medications, indicating that the beneficial effects of MTX use did not vary depending on whether the patient used other csDMARD (all interaction p values > 0.27).
In the best-fitting multivariable analysis (Model B), longer duration of past use since cohort entry was associated with a lower CVE risk for statins (HR 0.96 per each additional year of use, 95% CI 0.94–0.98; Table 4), but with an increased risk for glucocorticosteroids (HR 1.08 per additional year of use, 95% CI 1.05–1.11). We did not detect an association with CVE risk related to greater use of anti-TNF during followup (HR 1.02 per additional year of use, 95% CI 0.94–1.12), likely due to the small number of anti-TNF users. The strongest independent risk factors for a major CVE were preexisting comorbidities at time of RA diagnosis (Table 4).
Best-fitting multivariable model.
A sensitivity analysis involving 19,942 patients with RA without prior cardiovascular disease at cohort entry (Figure 1) produced results similar to those in the primary analysis (Supplementary Table 3, available with the online version of this article).
DISCUSSION
In this large population-based inception RA cohort, we used alternative time-varying exposures to examine the associations between MTX use (and other csDMARD) and risk of CVE. This allowed us to assess whether the effects varied by timing, recency, and duration of medication use, and whether the observed associations were sustained over time.
In our sample, we observed about a 20% decrease in CVE risk associated with recent (past 12 mos) continuous MTX use. This effect slightly weakened later in followup, suggesting that the observed effects may be strongest in the early phase of RA. We were unable to show an association of decreased events with greater cumulative MTX duration from the cohort entry to a current timepoint during followup. This suggests that patients may have to continue MTX throughout followup to maintain a decreased CVE risk. Further, first-year use also having a statistically significant association may suggest that a window of opportunity may be missed if MTX is not used early in the disease course. Because there is evidence that aggressive treatment soon after RA onset increases the chance of csDMARD-free remission15, these individuals subsequently may have less cumulative MTX or other csDMARD use throughout their entire disease course. The potential risk of high homocysteine levels and other adverse effects associated with chronic MTX use in some patients31,32 are also potential explanations for the weaker associations between MTX and CVE risk later in followup.
Our findings are compatible with a metaanalysis that estimated that MTX in RA was associated with 28% lower CVE risk, although the underlying studies were heterogeneous11. However, our methods were specifically designed to account for the time-varying nature of RA medication use, in contrast to previous studies, which mostly defined treatment use in a time-invariant manner12,13. Indeed, a systematic review reported that over 40% of the reviewed studies ignored the presence of time-varying exposures in the analyses33. However, in clinical practice, especially in chronic diseases such as RA, medication use is often time-variant, because treatment is frequently initiated at different intervals during a patient’s disease course and may be interrupted and/or reinitiated at some later time(s). Thus, our study fills an important gap in the literature because prior studies may have overestimated the treatment effect size or increased the risk of type II error (failure to detect a true association)28,34.
We found that preexisting comorbidities and glucocorticosteroids are associated with increased CVE risk, while statins were associated with a reduced risk. There is an accumulating body of evidence to support the use of statins for primary prevention of CVE in RA35,36,37. Statins not only provide a cholesterol-reducing effect in RA similar to those without RA38,39, they may also have some antiinflammatory and immunomodulatory properties that could attenuate RA-related inflammation and disease activity40,41. Whether all patients with RA would benefit from treatment with statins, irrespective of lipid levels, still requires investigation42.
Our study is unique, to our knowledge, in that it includes a large inception population-based RA cohort with detailed prescription data that enabled us to compare different time-varying treatment measures. However, several potential limitations warrant discussion. Evaluating the associations of RA treatments on CVE risk is difficult because greater medication use may be associated with more severe RA and the severity of RA may itself have effects on cardiovascular disease. Thus, similar to most other large administrative database studies of the effectiveness or safety of RA medications43,44,45, confounding by indication (or disease severity) cannot be ruled out, whereby MTX may be used less in patients with greater comorbidity (or lower disease activity) and/or those with a higher cardiovascular risk. Information on other potential confounders or effect modifiers, such as body mass index, physical activity, inflammatory markers, alcohol and tobacco use, folate supplementation, and over-the-counter acetylsalicylic acid and NSAID were not available to us. However, if MTX use was more frequent among patients with more severe RA, this would bias our results in the direction of higher estimated risks for users, and thus cannot explain the protective effects we found. Additionally, a recent analysis found no important differences in the distribution of these potential confounders across drug exposure categories (MTX vs other csDMARD)46.
While our analysis was confined to RA onset at a later age, the incidence of RA increases with age47 and our sample is thus an important component of the entire RA population, and one at high risk of CVE. Admittedly, the presentation, treatment regimens, severity, and prognosis of RA may differ for patients diagnosed at later ages48,49,50 and these differences may influence the generalizability of our findings. Thus replication in other cohorts may be in order. In addition, accurate dates of symptom onset were not available to us in administrative data and some RA may not have been truly incident.
While our analysis included a composite outcome (to identify the first occurrence of cardiovascular disease) and the treatment effects may vary across these individual events, prior studies that have separated their composite outcome into separate endpoints found the risk estimates to be similar to those using the composite endpoint46.
Greater recent use of MTX, particularly early in the disease course, is associated with a decreased risk of CVE in elderly-onset RA. Our alternative time-varying analyses provide important insights into the associations of MTX and cardiovascular morbidity in RA. The timing of MTX initiation, recency and duration of use appeared to be important factors in the observed associations between MTX and CVE risk. Our epidemiological evidence supports clinical recommendations that patients with RA should initiate MTX treatment early, with appropriate continuation to control disease over time.
Acknowledgment
We thank Brogan Inc., Ottawa, for use of its Drug Product and Therapeutic Class Database.
Footnotes
This analysis was supported by the Canadian Network for Advanced Interdisciplinary Methods for comparative effectiveness research, which is funded by the Canadian Institutes of Health Research Drug Safety and Effectiveness Network (funding reference no. TD3-137716). JW was supported by fellowship awards from The Arthritis Society and the Canadian Institutes of Health Research (Banting) during the course of this work; SB holds a career award from the Fonds de la recherche en santé du Québec; MA is a James McGill Professor of Biostatistics at McGill University. This study was supported by the ICES, a nonprofit research corporation funded by the Ontario Ministry of Health and Long-Term Care. Parts of this material are based on data and/or information compiled and provided by the Canadian Institutes of Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed in the material are those of the authors and not necessarily those of CIHI.
- Accepted for publication August 22, 2018.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.