
Abstract
Objective. To assess patient-reported burden of disease in pediatric patients with relapsing polychondritis (RP) and to compare those findings to adult patients.
Methods. A survey based on known clinical symptoms of RP was developed and administered to patients with a pediatric diagnosis of RP. Adult patients completed a similar survey.
Results. Twenty-one pediatric patients, or their parents, completed surveys. Median age at symptom onset was 6 years (interquartile range 1.8–12). Prior to diagnosis, most pediatric patients went to the emergency room (ER; 61.9%), saw > 3 physicians (57.1%), and took > 1 year to be diagnosed (61.9%). Pediatric patients were often diagnosed with asthma (42.9%), ear infections (42.9%), or sinusitis (33.3%) prior to diagnosis of RP. Symptoms prior to diagnosis included ear pain/redness (85.7%), joint pain/swelling (61.9%), and airway symptoms (38.1%). Four pediatric patients (19%) reported tracheomalacia requiring tracheostomy. Pediatric patients frequently missed school because of their disease (71.4%). Surveys from 290 adult patients were compared to pediatric patients. Pediatric patients were significantly more likely to undergo biopsy (42.9% vs 17.4%; p < 0.01) and be treated with biologics (42.9% vs 19%; p = 0.02). Adults were significantly more likely to be female (87.8% vs 28.6%; p < 0.01) and to report airway symptoms (77.9% vs 47.6%; p = 0.01). Prevalence of disease complications was not significantly different between adult and pediatric patients.
Conclusions. The burden of disease in pediatric patients with RP includes missed school, diagnostic delay, ER visits, and multisystem disease, with resultant damage to cartilaginous structures. Differences in airway involvement and treatment approaches may exist between pediatric and adult patients.
- PEDIATRIC RHEUMATIC DISEASES
- CARTILAGE
- SELF-ASSESSMENT
Relapsing polychondritis (RP) is a rare immune-mediated disease of unknown etiology characterized by recurrent episodes of chondritis1. Although the disease has a predilection for cartilaginous structures, particularly ears2, nose3, laryngotracheobronchial tree4, and joints/chest wall5,6, the disease can affect multiple organs including eyes7, central nervous system8, inner ear9, skin10, and vasculature11,12. The pathogenesis of RP is poorly understood, and clinical manifestations may be variable. End-organ damage can lead to significant morbidity and mortality. RP is rare in children and is estimated to account for < 5% of all cases based upon limited case series13. Pediatric-onset RP may have distinguishing features from adult-onset RP, including a higher rate of severe airway disease13,14. However, pediatric RP cohorts are often very small, and these associations have not been consistently observed across studies.
Recently, our group reported the results of an international survey describing patient-reported perception of RP-related symptoms, complications, organ pattern involvement, and treatment approaches in a cohort of adult patients with RP15. The results of this published survey provided novel information on the patient experience of RP. Further, the survey highlighted the need to develop a standardized set of classification criteria that better encompass the heterogeneity of disease manifestations uncovered by the survey. Whether adult and pediatric RP differ sufficiently in clinical phenotype as to require distinct classification criteria is unknown.
The objective of our current study was to describe the patient-reported perception of disease in a cohort of patients with a pediatric diagnosis of RP and to compare patient/parent-reported characteristics of disease between pediatric and adult patients with RP.
MATERIALS AND METHODS
Survey administration
Adult and pediatric patients were recruited through the Relapsing Polychondritis Awareness and Support Foundation (RPASF) and asked to participate in an online survey. A link to the surveys was provided to the participants on the patient support page. Patients were informed prior to completing the surveys that their participation was voluntary, anonymous, and that no personally identifying information would be collected. Because the surveys were conducted anonymously, the US National Institutes of Health, Office of Human Subjects Research Protections, considered them exempt from institutional review board approval.
Adult study population and survey elements
The development, implementation, and results from the adult survey have been reported elsewhere15. This previous work included data on patients who were ≥ 18 years old at the time of completing the adult survey. This previously reported data was reproduced here, but with minor modification to the inclusion criteria. Data from patients who completed the adult survey were included here only if the patients were ≥ 18 years old at the time of diagnosis with RP. This was done to allow for direct comparisons between adult and pediatric patients.
Pediatric study population and survey elements
The pediatric survey was essentially unchanged from the adult survey, with the exception of minor modifications to be age-appropriate and minor differences in question framing and response choices. For example, the pediatric survey did not include items querying about alcohol use, smoking, or pregnancy, but did include items related to missed school. The complete adult and pediatric surveys are included in Supplementary Files 1 and 2 (available with the online version of this article). The pediatric survey was open to participants from August 2016 to March 2017. Either the patient or the parent of the patient with pediatric RP answered the survey. Only patients who were < 18 years old at time of diagnosis were included in analyses of the pediatric survey.
Statistical analysis
SPSS 25 was used for descriptive statistical analyses. Fisher’s exact tests were performed using Prism 7. A 2-sided p value < 0.05 was considered statistically significant.
RESULTS
Pediatric patient demographics
Thirty-one surveys were completed. Results from 9 respondents were excluded from further analysis because of diagnosis of RP as an adult (> 18 yrs of age). A further patient was excluded from the analyses because the patient reported suspected disease but had not been formally diagnosed with RP. A total of 21 surveys were ultimately included in the analyses and patient characteristics are shown in Table 1. The patients were predominantly male (71.4%, n = 15), white (66.7%, n = 14), and from the United States (81%, n = 17). The median age of the patients at the time of answering the survey was 15 years [interquartile range (IQR) 8.5–16]. The median age that symptoms attributable to RP were first noticed was 6 years (IQR 1.8–12). The median age of diagnosis with RP was 9 years (IQR 6.5–14). The majority of the surveys were filled out by the mothers of the patients (90.5%, n = 19).
Demographic characteristics of 21 patients with a pediatric diagnosis of relapsing polychondritis who completed the survey.
Patient-reported symptoms
Patients with a pediatric diagnosis of RP reported a variety of initial symptoms prior to diagnosis. Ear pain (71.4%, n = 15) and ear redness (81%, n = 17) were the most commonly endorsed symptoms. Joint pain was the next most commonly experienced symptom (52.4%, n = 11). In particular, knee (28.6%, n = 6) and ankle (33.3%, n = 7) were the most commonly painful joints. Several patients also reported shortness of breath (33.3%, n = 7), painful breathing (9.5%, n = 2), and voice changes (23.8%, n = 5) suggestive of airway involvement. Despite ear involvement with pain and redness being a characteristic feature of RP, 3 patients (14.3%) denied any ear-related symptoms (pain or redness) prior to diagnosis. Two of these 3 patients continued to experience no ear pain or redness at the time of the survey. One patient (4.8%) reported isolated airway and joint symptoms with no ear/nose-related symptoms. Symptoms experienced prior to diagnosis and cumulative symptoms are summarized in Figure 1.
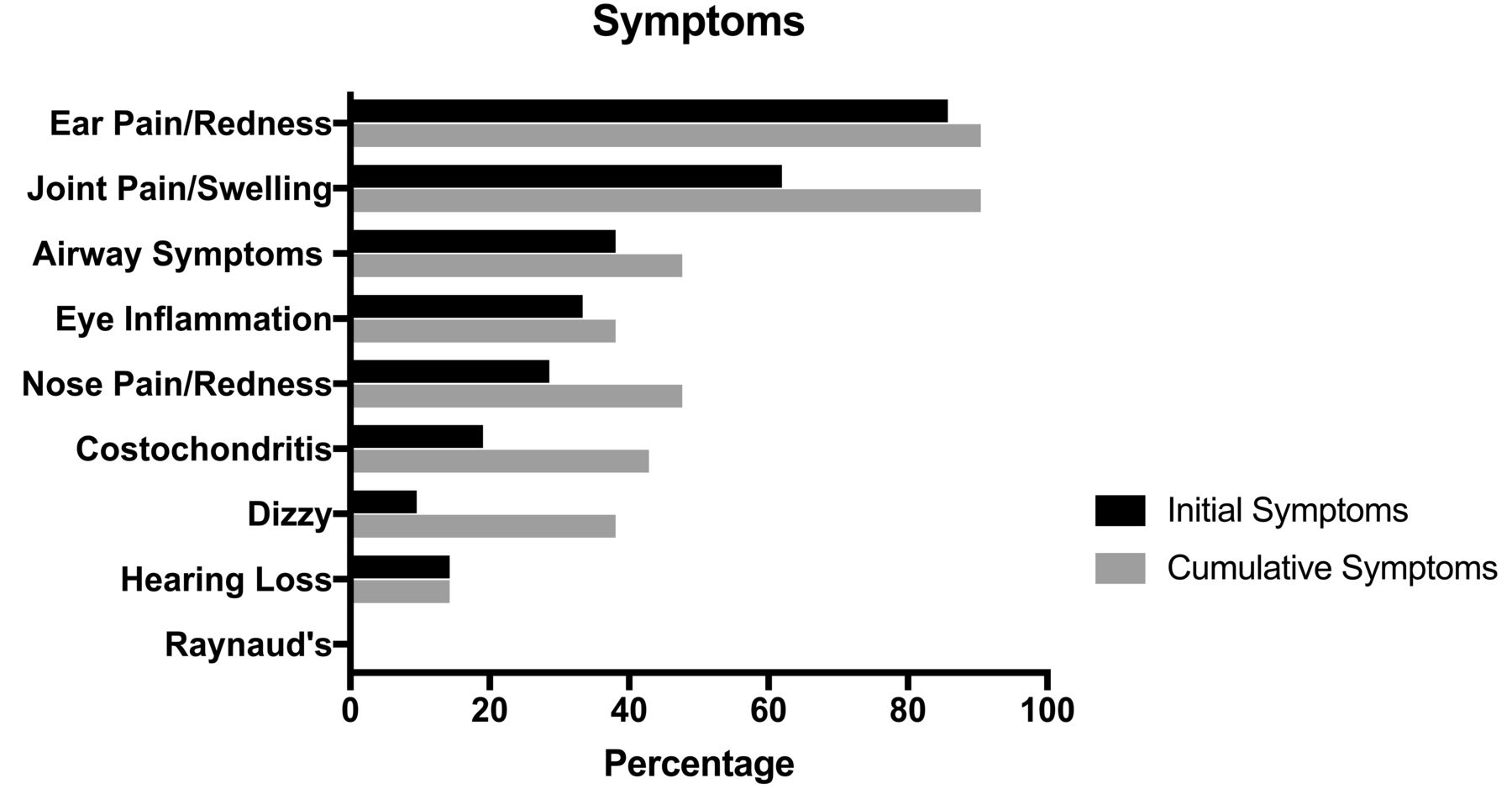
Symptoms reported by 21 patients with a pediatric diagnosis of relapsing polychondritis (RP). Symptoms reported prior to diagnosis with RP or cumulatively experienced by pediatric patients with RP.
Symptom triggers
Pediatric patients with RP endorsed several triggers of symptom worsening. Change in weather was the most frequently reported trigger (47.6%, n = 10). Other triggers included sun exposure (33.3%, n = 7), emotional stress (33.3%, n = 7), physical activity/exercise (28.6%, n = 6), lack of sleep (19%, n = 4), plane travel (9.5%, n = 2), physical injury (9.5%, n = 2), piercings (4.8%, n = 1), and surgery (4.8%, n = 1). Many patients also reported worsening of RP-related symptoms in relation to dietary factors (52.6%, n = 10 out of 19 respondents who answered the question), including gluten (21.1%, n = 4 out of 19 respondents who answered the question) and excessive sugar (26.3%, n = 5 out of 19 respondents who answered the question). Additionally, 66.7% (n = 4 out of 6 respondents who answered the question) of female patients endorsed worsening of symptoms with menses (1 female patient did not answer the question, and 1 was below the age of menarche).
Pathway to diagnosis
Before being diagnosed with RP, the majority of pediatric patients were evaluated by > 3 physicians (57.1%, n = 12). Nine patients received a diagnosis within 1–5 years (42.8%). Two patients (12.5%) were not diagnosed for > 10 years. Many patients (61.9%; n = 13) were evaluated in the emergency room (ER) because of RP symptoms prior to diagnosis, with 46.2% of these (n = 6 out of 13) going to the ER 4 or more times. The top reasons for going to the ER were shortness of breath/difficulty breathing (53.8%, n = 7 out of 13), ear pain/swelling (46.2%, n = 6 out of 13), or throat pain (30.8%, n = 4 out of 13). Patients were most commonly diagnosed by either a rheumatologist (47.6%, n = 10) or an otolaryngologist (28.6%, n = 6). However, in some cases other specialists established the diagnosis (including — one each — allergist, immunologist, nephrologist, pulmonologist, and infectious disease physicians). Nine patients (42.9%) had a biopsy to establish the diagnosis. Of those who underwent biopsy, 66.7% (n = 6 out of 9 respondents) could recall what site was biopsied. The most common biopsy sites were ear (66.7%, n = 4 out of 6), trachea (33.3%, n = 2 out of 6), and kidney (16.7%, n = 1 out of 6). Patients often received other diagnoses prior to RP: 42.9% (n = 9) of the patients were diagnosed with an ear infection, 42.9% (n = 9) were diagnosed with asthma, and 33.3% (n = 7) were diagnosed with sinusitis. Several patients (28.6%, n = 6) reported being diagnosed with another autoimmune disease after receiving a diagnosis of RP. These included arthritis (66.7%, n = 4 out of 6) and vasculitis/ Behçet disease (33.3%, n = 2 out of 6). Additionally, 1 patient (4.8%) reported being diagnosed with fibromyalgia after receiving a diagnosis of RP. Characteristics of the diagnosis process are detailed in Table 2.
Characteristics of the diagnostic process reported by 21 patients with a pediatric diagnosis of relapsing polychondritis.
Patient-reported treatment modalities
The most commonly reported treatment modality was glucocorticoids. Most patients (71.4%, n = 15) used prednisone at some point in their disease process. Of those treated with prednisone, 69.2% (n = 9 out of 13 respondents) recalled receiving high-dose therapy (≥ 60 mg). Patients were also frequently treated with disease-modifying antirheumatic drugs (DMARD; 71.4%, n = 15), the most common being methotrexate (80%, n = 12 out of 15). Additionally, 42.9% (n = 9) of patients were treated with some form of biologic therapy, with the most common class represented by anti–tumor necrosis factor agents (88.9%, n = 8 out of 9). Other biologic therapies included anakinra (33.3%, n = 3 out of 9), abatacept (22.2%, n = 2 out of 9), and tocilizumab (11.1%, n = 1 out of 9). Treatments reported by patients are shown in Figure 2 and Table 3.

{kind=link}
{kind=link}
Treatments reported by 21 patients with a pediatric diagnosis of relapsing polychondritis. The medications were being taken currently at the time of the survey or were taken in the past. TNF: tumor necrosis factor; NSAID: nonsteroidal antiinflammatory drug.
Cumulative treatment modalities reported by 21 patients with a pediatric diagnosis of relapsing polychondritis.
Complications and burden of disease
A severe complication of RP is tracheomalacia. Four patients (19%) reported developing tracheomalacia and all of them required a tracheotomy. Additionally, hospitalizations were frequent in this cohort with 55.6% (n = 10 of 18 respondents) of patients who answered the question reporting hospitalization owing to RP. These patients were hospitalized a median of 5 times (IQR 1–11.9). Patients also frequently missed school because of their disease (71.4%, n = 15). Of those patients, 33.3% (n = 5 out of 15) missed school for a period ranging between 1 week and 1 month; 66.7% (n = 10 out of 15) missed school for more than 1 month. Patients also reported disability as a result of their disease, including the need to use a hearing aid (9.5%, n = 2). Several patients required the use of assistive devices such as wheelchairs or canes (14.3%, n = 3).
Comparison of pediatric and adult patients with RP
Data from 290 patients with an adult diagnosis of RP were compared to the 21 patients with a pediatric diagnosis of RP. The adult patients were predominantly female (87.8%, n = 253) and white (89.2%, n = 257). The median age of the adult patients at the time of answering the survey was 49 years (IQR 41.8–56). The median age of diagnosis with RP was 45 years (IQR 35.7–51.3).
Overall, the majority of disease characteristics and symptoms were similar between the 2 cohorts, such as the rates of ear/nose involvement, joint pain/swelling, costochondritis, eye involvement, and dizziness (p > 0.05; Table 4). Pediatric and adult patients also did not differ significantly in the localization of joint pain/swelling (Supplementary Table 1, available with the online version of this article). Adult patients were significantly more likely to be female (87.8% adults vs 28.6% pediatric; p < 0.01) and white (89.2% adults vs 66.7% pediatric; p < 0.01) than pediatric patients. Surprisingly, a significantly higher percentage of adult patients reported symptoms suggestive of airway involvement (77.9% adults vs 47.6% pediatric; p = 0.01). Only adult patients reported Raynaud symptoms (23.1% adults vs 0% pediatric; p = 0.01).
Comparison of patient-reported characteristics of disease between patients with an adult or a pediatric diagnosis of relapsing polychondritis.
The diagnostic process experienced by pediatric and adult patients with RP was largely similar, with both cohorts visiting the ER, seeing > 3 physicians prior to diagnosis, experiencing diagnostic delays > 5 years, and being diagnosed with asthma, ear infections, or sinusitis prior to diagnosis with RP (p > 0.05). On the other hand, pediatric patients were significantly more likely to undergo a biopsy to establish the diagnosis compared to adult patients (42.9% pediatric vs 17.4% adults; p < 0.01). Pediatric patients were also more likely to be treated with a biologic agent (42.9% pediatric vs 19% adults; p = 0.02). No differences for prednisone or DMARD therapy were observed between adult and pediatric patients. Lastly, no significant differences in disease complications such as tracheomalacia, hearing loss, pneumonia, or intubation were found between the 2 cohorts (p > 0.05).
DISCUSSION
Here we report the results of the largest international survey to date, to our knowledge, of children with RP. We leveraged the resources of an international support group and an international referral center to characterize the experiences of individuals with a rare and poorly understood disease. In this cohort, we found that pediatric RP is associated with frequent hospitalizations and ER visits, missed school, and disability. We learned that significant barriers to diagnosis are experienced by pediatric patients with RP, similar to what has previously been reported in adult patients15. These barriers consist of a lengthy time to diagnosis, misclassification of disease (e.g., sinusitis, asthma, or ear infection), and the need to see a number of providers to establish the diagnosis. Insight into potential disease triggers was derived by our survey. Among other environmental determinants, change in weather, sun exposure, exercise, and menstruation were all highlighted by our respondents. Disease-related damage was identified in terms of a 19% tracheotomy rate along with a high usage rate for assistive devices. Finally, the design of our study enabled a preliminary analysis comparing and contrasting patients with a pediatric or adult diagnosis of RP.
There are no available studies that rigorously compare cohorts of pediatric patients to adult patients with RP. Important differences, such as the propensity for more severe airway disease in pediatric patients, have been inconsistently observed13,14. Our own group recently reported the results from adult patients with RP who completed a survey nearly identical to that reported here15. We were thus able to compare the self-reported data from patients with a pediatric versus an adult diagnosis of RP. Of note, we found that pediatric patients were more likely to undergo biopsy and be treated with a biologic agent. This suggests that physicians may be targeting pediatric patients with RP more aggressively for diagnosis and treatment than adults. Alternatively, it is also possible that pediatric patients present with more symptomatic disease, leading to these more aggressive approaches. However, this is less likely, given that the pattern of organ involvement and disease complications reported by children and adults in this study was similar, and in the case of airway symptoms, was actually worse in adult patients.
A case series of 3 pediatric patients, which also incorporated a review of 44 published case reports, found that pediatric-onset RP may have a higher rate of severe airway disease, higher rate of costochondritis, and more severe arthritis, and that children are less likely to have other associated autoimmune diseases than adult patients14. However, that study did not perform any statistical comparisons between the 2 cohorts. In our cohort, rates of costochondritis and joint pain/swelling were not significantly different between adult and pediatric patients. Likewise, adult patients did not have significantly higher rates of other autoimmune diseases than did pediatric patients. Further, we observed that pediatric patients had significantly less airway involvement as compared to adult patients, and a similar rate of tracheomalacia. Nevertheless, airway involvement in children was still considerable in the survey respondents (47.6%). Our results seem to be more in line with a second case series of 10 pediatric patients, which reported airway involvement incidence of 40%13.
Our current study, taken alongside our previous work with adult patients15, continues to emphasize the need to develop classification criteria for RP to facilitate clinical research in this disease. Current diagnostic criteria, such as those by McAdam, et al16, Damiani and Levine17, and Michet, et al18 are likely inadequate to serve as classification criteria in RP. Those diagnostic criteria were developed in single centers, with a low number of patients, and have never been validated in an independent patient cohort. Additionally, our results demonstrate that a wide degree of clinical heterogeneity exists in RP and patients may present with isolated (i.e., auricular chondritis only) or systemic forms of disease that would not always be identified by current diagnostic criteria. Future classification criteria will need to take this into account to facilitate appropriate clinical trial recruitment. Importantly, the results of our study suggest that it is reasonable to develop a single set of classification criteria to be used in both adult and pediatric RP. The frequency of reported symptoms was largely similar in both patient cohorts, as were longterm complications of the disease.
One limitation of our study was that we were not able to perform a chart audit to confirm the medical diagnoses, and our design does not allow control for potential study participant selection bias. An additional limitation is that although the surveys administered to pediatric and adult participants were similar, there were still minor differences in survey items that may confound results. In particular, this is true for the questions about treatment approaches, where the pediatric survey included additional close-ended response choices relating to biologic treatments than were included in the adult survey. Ultimately, the psychometric requirements for targeting children (or their parents) versus adult respondents were not addressed, and hence this may pose challenges for rendering comparisons between the populations. The possibility of recall bias is also inherent in this type of instrument. A strength of the study is the relatively large and geographically diverse population that we were able to gather for this rare disease.
We have used an international survey to glean new insights into a pediatric diagnosis of RP. These insights may pave the way for future research aimed at achieving earlier identification of common ER or acute care presentations of patients with RP, preventing a rare disorder from being misclassified as asthma, ear infection, or sinusitis.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
We thank the patients and families of patients with RP for their participation and the Relapsing Polychondritis Awareness and Support Foundation for its help in completing this project.
Footnotes
This research was supported by the Division of Intramural Research of NIAMS.
- Accepted for publication April 9, 2019.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.