
Abstract
Objective. Antibodies that recognize the phosphatidylserine/prothrombin complex (antiphosphatidylserine/prothrombin antibodies; aPS/PT) might reveal enhanced thrombotic risk in patients with systemic lupus erythematosus. Little is known about their association with pregnancy complications in the antiphospholipid syndrome (APS).
Methods. We enrolled 55 patients with APS who were seeking pregnancy in 2 Italian hospitals. Antiphospholipid antibodies (aPL), including anticardiolipin antibodies, anti-β2-glycoprotein I antibodies, lupus-like anticoagulant, and aPS/PT antibodies were assessed, and the patients were prospectively followed for 24 months.
Results. There were 65% (36/55) of the APS patients who had aPS/PT antibodies. Forty-seven pregnancies were followed, including 33 of aPS/PT+ patients. Forty-one of the 47 patients (87%) who initiated a pregnancy eventually gave birth to a child. The pregnancy duration and the mean newborn weight at delivery were significantly lower in aPS/PT+ than in aPS/PT− patients (33.1 ± 4.7 vs 36.2 ± 3.4 wks of gestation, respectively, and 2058 ± 964 g vs 2784 ± 746 g, respectively, p < 0.05). Late pregnancy complications, including intrauterine fetal death, preterm delivery, preeclampsia, and intrauterine growth restriction (IUGR), were more frequent in aPS/PT+ patients, independent of the therapy. Titers of aPS/PT IgG were significantly inversely correlated with the neonatal weight at delivery. Vascular injury, as reflected by thrombosis, fibrinoid necrosis, ischemic and hemorrhagic areas, and presence of chorangiomas characterized the IUGR placentas in the presence of aPS/PT.
Conclusion. The aPS/PT antibodies might represent markers of aPL-related pregnancy complications, IUGR/preeclampsia in particular, and could help identify beforehand patients who may require additional treatment.
- PREGNANCY OUTCOMES
- ANTIPHOSPHOLIPID SYNDROME
- ANTIPHOSPHATIDYLSERINE/PROTHROMBIN ANTIBODIES
- INTRAUTERINE GROWTH RESTRICTION
- PREECLAMPSIA
Antiphospholipid antibodies (aPL), in association with arterial and/or venous thromboses or with pregnancy complications, define the antiphospholipid syndrome (APS)1,2. Pregnancy morbidity in APS comprises fetal and maternal complications3,4, and the obstetric APS might represent a nosologically independent entity5,6. Pregnancies of patients with obstetric APS, when treated, have generally satisfactory fetal and maternal outcomes. Moreover, thrombosis and progression of associated autoimmune diseases in obstetric APS patients are less frequent. Mechanisms underlying aPL-mediated damage could differ in obstetric APS and APS5 with thrombosis. The most frequent fetal complication is recurrent pregnancy loss7,8. Preeclampsia and placental insufficiency may appear as prematurity, intrauterine growth restriction (IUGR), and intrauterine fetal death (IFD)9.
The mechanisms through which aPL contribute to pregnancy complications are being actively investigated. Intraplacental thrombosis was initially suggested as responsible for the obstetric outcome. However, additional events clearly contribute10 and various inflammatory pathways are implicated in deleterious effect of aPL on the human placentation, including complement activation and deposition11,12,13, neutrophil infiltration, and local deposition of vessel-damaging neutrophil extracellular traps14. Infarctions, impaired remodeling of spiral arteries, inflammation of the decidua, increased syncytial knots, and the deposition of complement split products are indeed hallmarks of the aPL-mediated damage of the placentas15. Their diversity suggests that multiple pathological processes occur during pregnancy in these patients11.
Treatment during pregnancy is based on the association of low-dose aspirin (LDA) and low molecular weight heparin (LMWH). Indeed, heparins are known to have antiinflammatory activities, which may contribute to their protective actions at prophylactic doses11,16. The likelihood of a satisfactory pregnancy outcome in treated APS women is around 75–80%. However, a consistent fraction of women does not respond to the treatment and still experiences miscarriages and various pregnancy complications3.
A substantial effort has been carried out in the past decades to identify biomarkers that can predict the failure of conventional treatments in pregnant patients. Placental trophoblast exposes anionic phospholipids such as phosphatidylserine on the outer leaflet of the plasma membrane, possibly providing a preferential template for the assembly of the antigenic target recognized by aPL3,9,17,18. Indeed, patients whose autoantibodies recognize multiple epitopes of the anionic phospholipid-associated antigenic target, such as those triple-positive for anticardiolipin antibodies (aCL), anti-β2-glycoprotein I (anti-β2-GPI) antibodies, and lupus-like anticoagulant (LLAC) have a higher risk of severe pregnancy morbidity and recurrent thromboembolic events. Patients with triple aPL positivity and history of thrombosis with or without systemic lupus erythematosus (SLE) are more likely to experience treatment failure19,20,21.
Antibodies targeting other anionic phospholipid-associated antigenic moieties have been extensively investigated, including antiprothrombin antibodies (aPT), antiphosphatidylserine antibodies, and antibodies directed against the phosphatidylserine-prothrombin complex (aPS/PT)22,23,24,25.
Positivity for aPS/PT has been strongly associated with severe aPL-associated manifestations, mainly thrombotic events irrespective of the site and type of thrombosis22,26,27 and may be useful for explaining an LLAC presence when classifying negative aPL patients21,28,29,30. Previously, retrospective studies have suggested an association of aPS/PT antibodies with adverse pregnancy outcomes, irrespective of the presence of other aPL31. The multicentric Nîmes Obstetricians and Hematologists (NOHA) case-control study has previously confirmed that aPS/PT represents a promising biomarker, in particular when LLAC results are difficult to interpret25.
IUGR reflects the disruption of the interaction among the maternal, placental, and fetal environments32. Its persistence despite treatment in patients with APS suggests that additional factors, not yet identified and possibly including unconventional aPL, might contribute to its pathophysiology. Our present study aimed at investigating whether aPS/PT might associate with complications in prospectively followed treated patients. We have analyzed the possibility that aPS/PT antibodies might represent biomarkers to identify high-risk patients with APS who might benefit from additional treatments and intensive clinical monitoring during pregnancy.
MATERIALS AND METHODS
Patients
Two rheumatology units participated in our study. Inclusion criteria comprised the following: (1) APS diagnosis according to the criteria1,2; (2) patients trying to get pregnant; (3) a counseling visit within 3 months before the beginning of pregnancy; and (4) signed informed consent.
Patients with identifiable causes for miscarriages, including those with uterine or chromosomal abnormalities in either partner, dysthyroidism, or diabetes, were excluded. Approval was obtained from the Comitato Etico Ospedale San Raffaele, Milan, Italy (protocol “Autoimmunomol”, PI Angelo Manfredi, no. 2/2013INT). This study was conducted in accordance with the Declaration of Helsinki. Fifty-five APS women who were seeking pregnancy were recruited (27 in the University Hospital of Padua and 28 in the San Raffaele University Hospital, Milan) and followed by a multidisciplinary team including rheumatologists and gynecologists. In their medical history, 25 patients had thromboembolic events, 15 had late pregnancy complications such as IUGR or preeclampsia before 34 weeks of gestation (wg) associated or not with ≥ 1 early miscarriages, 6 had pregnancy losses between 10 and 25 wg + 5 days, 6 had IFD defined according to the Health Ministry in accordance with the Italian law, and 7 had ≥ 3 early miscarriages. Two patients were included in the study even though they had only 2 early miscarriages. Thirty-six patients had primary APS, 19 patients had APS associated to systemic autoimmune diseases (11 SLE, 8 undifferentiated connective tissue disease). All patients had, at the time of conception, a stable and well-controlled disease. A summary of treatments is depicted in Supplementary Table 1 (available with the online version of this article). We recorded all relevant demographic and anamnestic data at the first visit. All patients had been evaluated for congenital thrombophilia (factor II, factor V Leiden, protein C, protein S, antithrombin III, and homocysteinemia).
Autoantibodies
Each recruited patient was characterized for the presence of aPL2. LLAC was detected according to international guidelines33. IgG and IgM antibodies, aCL, aPS/PT, and aβ2GPI IgG and IgM antibodies were assessed by ELISA (QUANTA Lite ACA IgG and IgM, and β2-GPI IgG and IgM). INOVA Diagnostic Inc. provided aPS/PT IgG and IgM and they were assessed on serum samples obtained at the first visit, immediately before or at the beginning of pregnancy. The cutoff levels were previously established at 20 IgG phospholipid units or SGU (standard G unit) for IgG and 20 IgM phospholipid units or SMU (standard M unit) for IgM, according to the manufacturer’s instructions, and at 30 U/ml for aPS/PT. Clinicians were blinded to the results of the aPS/PT assay only.
Study design
Gestational age was calculated from the last menstrual cycle confirmed by ultrasound during the first trimester. Treatment was started as soon as possible with LDA (100 mg) and prophylactic LMWH (4000 U daily) starting from the detection of fetal heartbeat. In patients with previous thromboembolic events, therapeutic dosage of LMWH was considered. Plasmapheresis and/or intravenous immunoglobulin (IVIG) were added in 18 patients during pregnancy. In 94% (44/47), LDA was started preconceptionally. Ultrasonography was performed at 6–8 wg, 12 wg, 20 wg, 24 wg, 32 wg, 35–36 wg, and when fetal and/or maternal conditions required it. Patients were carefully monitored for the onset of arterial hypertension (HTN), preeclampsia, and/or the Hemolysis, Elevated Liver enzymes, and Low Platelet count (HELLP) syndrome. Preeclampsia was defined according to the criteria of the International Society for the Study of Hypertension in Pregnancy as a de novo rise in systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg in the second half of pregnancy, and proteinuria ≥ 300 mg/24 h. Preeclampsia onset has occurred in all patients before 34 wg.
HELLP syndrome was diagnosed according to previously published criteria based on the following laboratory abnormalities: aspartate aminotransferase > 50 U/l or alanine aminotransferase > 50 U/l, lactate dehydrogenase > 600 U/l, platelet count < 100 × 109/l, and evidence of hemolysis. IUGR was defined according to the World Health Organization classification as a child with weight at delivery < 10° growth centile compared to the standard weight for sex and gestational age34. Clinical Doppler ultrasound data (Pulsatility Index) were collected during ultrasonography examination at 20 and 24 wg.
Histology
Placentas were collected after cesarean birth or vaginal delivery and immediately fixed in 4% neutral buffered formalin from APS patients with aPS/PT (Group A) or without aPS/PT (Group B), with previous history of unexplained IUGR and IFD (Group C), and with previous unexplained recurrent miscarriages (Group D). Placenta from healthy women served as controls (Group E). All placentas were examined macroscopically and microscopically. Formalin-fixed placental weight and the percentage of macroscopic lesions on the surface were determined. Subsequently, 2 samples of the umbilical cord, fetal and placental membranes, and at least 2 samples of macroscopically normal placental tissue were taken from a central part of a placental cotyledon and from a peripheral area. Additional samples of lesions were also taken. Samples were processed and embedded in paraffin wax for histology.
Statistical analysis
Comparisons between groups that were defined based on the presence or absence of aPS/PT and on the presence or absence of concomitant presence of aCL, anti-β2-GPI, and aPS/PT IgM and/or IgG were performed using chi-square test and ANOVA, as appropriate. When indicated, Eulero-Venn diagram and scatter histograms were used. We considered differences to be statistically significant at p < 0.05.
RESULTS
Higher frequency of late pregnancy complications in aPS/PT+ patients
There were 55 patients included in our study (Supplementary Figure 1, available with the online version of this article). Thirty-six patients (65%) were aPS/PT+ and 19 (34%) aPS/PT−. Demographic data and obstetrical history are reported in Table 1A and Table 1B, respectively. aPS/PT+ and aPS/PT− patients did not significantly differ for most epidemiological features. Although the median age was similar, aPS/PT+ patients were younger at diagnosis and had a significantly higher incidence of HTN and of previous thromboembolic events (Table 1A).
Baseline characteristics of the study population. Values are mean ± SD or n (%) unless otherwise specified.
Previous pregnancy outcomes of aPL-positive patients. Values are n (%) unless otherwise specified.
Thirty-three aPS/PT+ and 14 aPS/PT- patients during the period of the study had a new pregnancy (Supplementary Figure 1, available with the online version of this article). The rate of complications during pregnancy was higher in aPS/PT+ (79%) than in aPS/PT- patients (57%), but the difference was not statistically significant. In contrast, the duration of the pregnancy (as assessed by the mean number of wg) and the mean newborn weight at delivery were both significantly lower in aPS/PT+ patients (pregnancy duration 33.1 ± 4.7 vs 36.2 ± 3.4 wg and newborn weight 2058 ± 964 vs 2784 ± 746 g in aPS/PT+ than in aPS/PT- patients, respectively, p < 0.05; Table 2). All patients had been treated with LMWH (prophylactic or therapeutic dosage depending on previous thromboembolic events), either alone or in association to LDA. There were 11/47 patients (23%) who received corticosteroids (mean 7.5 mg/d), 6 (13%) hydroxychloroquine, 2 (4%) IVIG, 18 (38%) plasmapheresis and/or IVIG. There was no significant difference in the treatment of patients with primary APS and of patients with APS associated to systemic autoimmune diseases (not shown) or of aPS/PT+ and aPS/PT- patients, except for plasmapheresis and/or IVIG that were more frequently used in pregnancies of aPS/PT+ patients (Table 2).
Outcomes of 47 pregnancies followed during this study. Values are mean ± SD or n (%) unless otherwise specified.
Possibly because of the treatment, complications were less frequent in the pregnancies followed during the study compared to those in the patients’ obstetrical history (compare Table 1B and Table 2; e.g., rate of miscarriages was 4% in prospectively followed pregnancies vs 53% in prior pregnancies of the same patients). The difference was striking both in aPS/PT+ and in aPS/PT− patients. In contrast, the rate of late pregnancy complications, preeclampsia, and/or HELLP-treated aPS/PT+ patients remained unexpectedly high. Twelve of 33 (36%) aPS/PT+ versus 0 of 14 aPS/PT-patients had preeclampsia (p < 0.006), even if treated with LMWH, and in 10 of 12 (83%) with LMWH plus LDA. There were 5/12 (42%) who also received plasmapheresis (3/5 in association with IVIG).
Twelve patients of 33 (36%) versus 1 of 14 (7%) had IUGR (p < 0.05), and 4 of the 13 had preeclampsia as well. Eight of the patients who experienced IUGR had a previous IUGR in their obstetrical history, and all of them were aPS/PT+. The titer of aPS/PT IgG antibodies was inversely correlated with the neonatal weight at delivery (Figure 1, p < 0.005, r = −0.46).
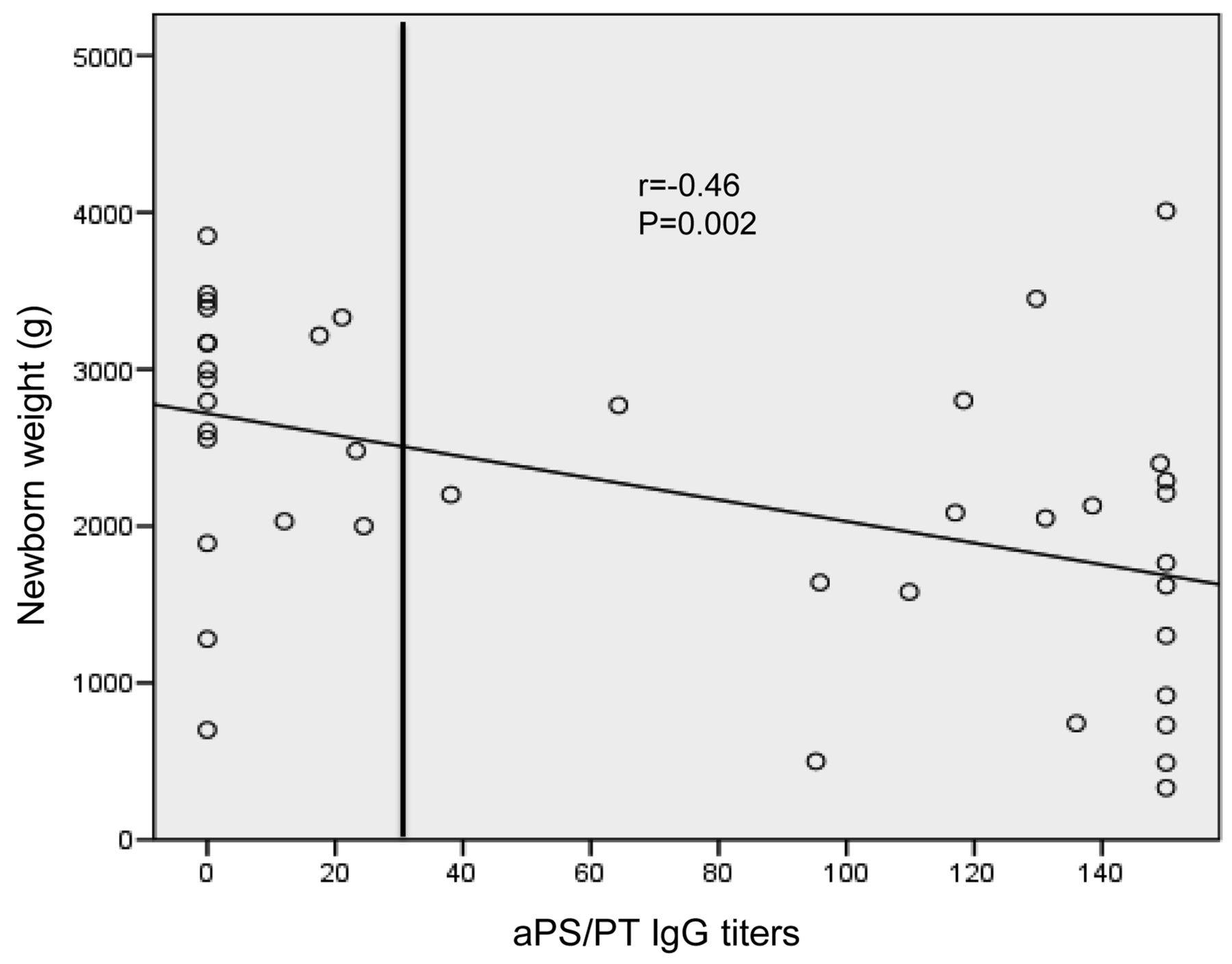
Scattergram representing the correlation of aPS/PT IgG titers (X axis) and the newborn weight at birth (Y axis). aPS/PT: antiphosphatidylserine/prothrombin antibodies.
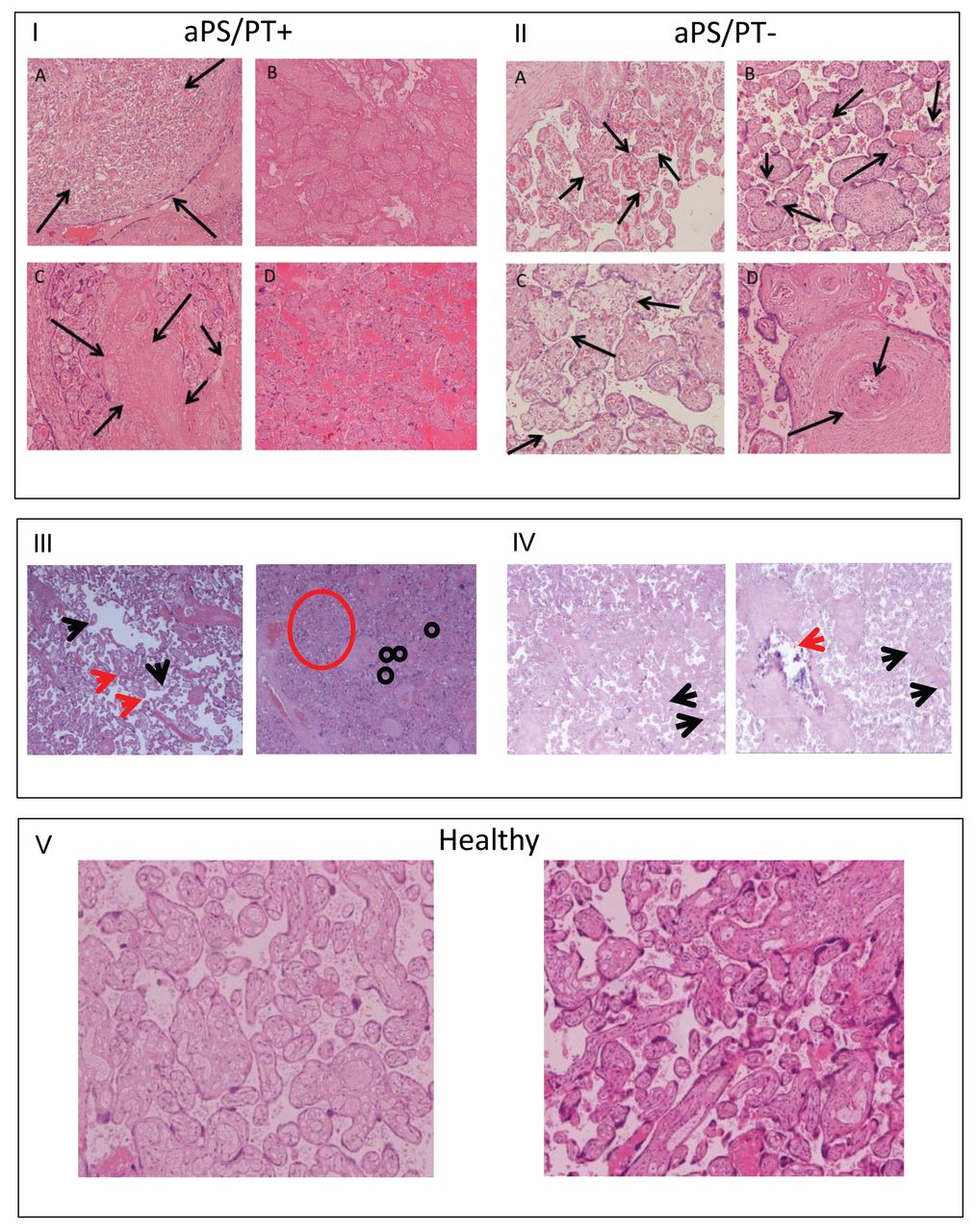
Thrombosis, hemorrhages, and ischemic areas and features revealing rather severe hypoxia such as chorangiomas were consistent features of placental samples of aPT/PS+ patients. Chorangiosys (i.e., the increased number of the capillaries of the villus that reflects low-grade hypoxia, atherosis, immature chorionic villi, and polar proliferation) was, in contrast, prominent in the placentas of aPT/PS− patients (Figure 2). Tissues of patients with unexplained IUGR or recurrent miscarriages are shown for reference. All the patients received therapy with LDA + LMWH during the followed pregnancy. Healthy placental tissue is also shown (Figure 2).

Representative tissues showing characteristics of the placenta of patients with APS. I. aPS/PT+ patients at delivery (37 wg). IA. Chorangiomas. IB. Placental infarcts, villous necrosis secondary to local obstruction of maternal uteroplacental circulation. IC. Fibrinoid necrosis associated to placental hypoperfusion. ID. Features associated with hemorrhagic spreading. Panel II. aPS/PT− patients at delivery (37 wg). IIA. Prevalent chorangiosis. IIB. Increased syncytial knotting. IIC. Some features of parenchymal dysmaturity. IID. Hypertrophic vessel wall with focal atherosis. III. Patient with previous unexplained IUGR and IFD, delivery at 32 wg. During pregnancy, the patient had been treated with LDA + LMWH. Note the intermediate and immature placental villi corresponding to the gestational week and increased syncytial knotting and villous agglutination. IV. Patient with previous unexplained recurrent miscarriages, delivery at 40 wg. During pregnancy, the patient had been treated with LDA + LMWH. Note the normal parenchymal features and low-grade ischemic damage with areas of fibrinoid necrosis and villous calcification. V. Normal features of full-term placentas. APS: antiphospholipid syndrome; aPS/PT: antiphosphatidylserine/prothrombin antibodies; wg: weeks of gestation; IUGR: intrauterine growth restriction; IFD: intrauterine fetal death; LDA: low-dose aspirin; LMWH: low molecular weight heparin.
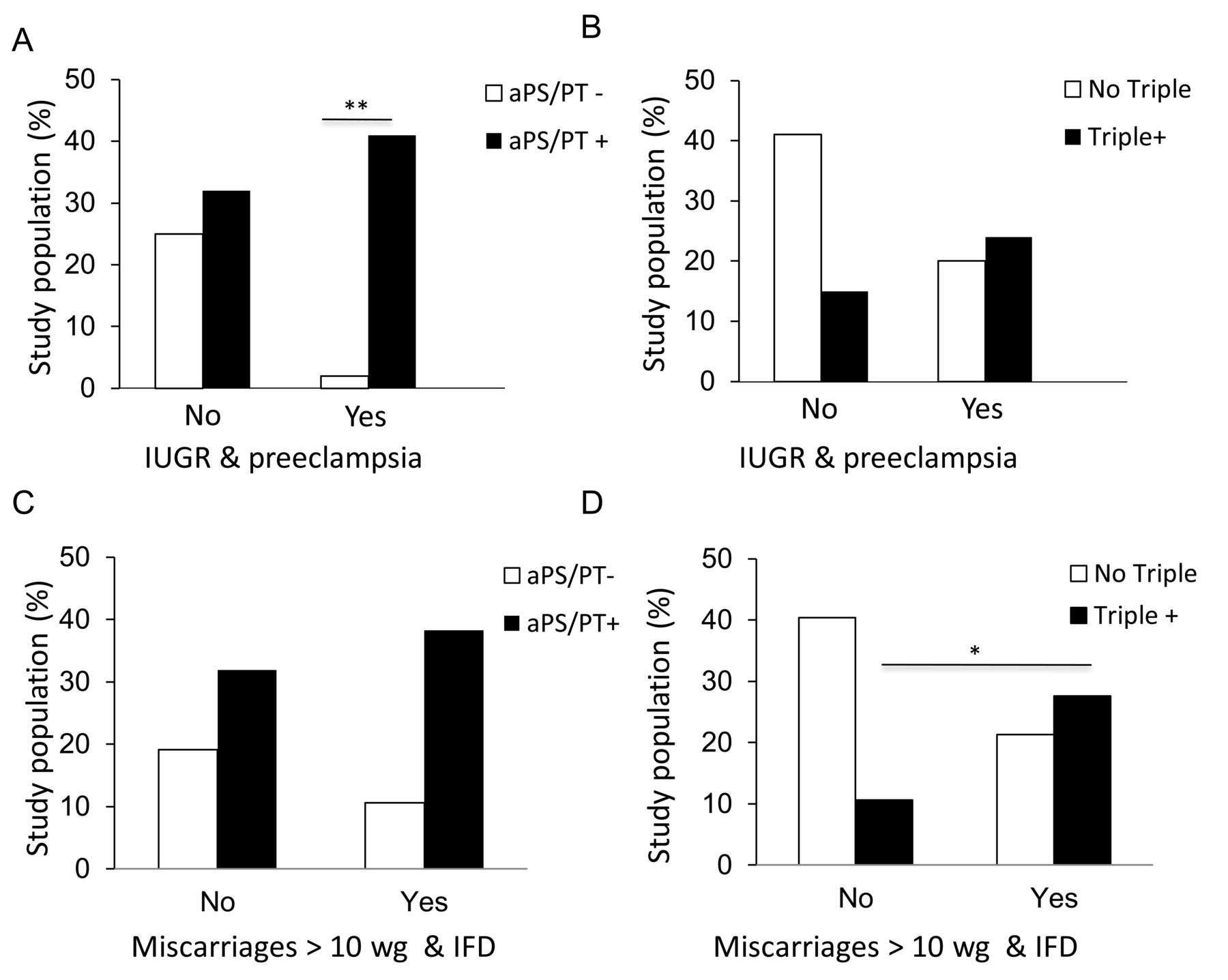
Among biomarkers associated with pregnancy complications, the simultaneous triple positivity of aCL, anti-β2-GPI, and LLAC, which was present in 20 of 55 patients (36%), was significantly correlated with the occurrence of miscarriages after 10 wg and/or with IFD (Figure 3C and Figure 3D). The presence of aPS/PT might further contribute to the identification of patients at higher risk of IUGR and/or preeclampsia (Figure 3A and 3B).

{kind=link}
{kind=link}
{kind=link}
Panel A and B: aPS/PT and late complications of pregnancy. IUGR and/or preeclampsia were significantly more frequent in aPS/PT+ (filled columns) than in aPS/PT− patients (**p < 0.007). Panel C and D: Triple positivity and fetal death. Miscarriages > 10 wg and/or IFD were significantly more frequent in patients with the simultaneous presence of aCL, anti-β2-GPI, and LLAC (triple positivity, filled columns) than in patients without triple positivity (*p < 0.05). aPS/PT: antiphosphatidylserine/prothrombin antibodies; IUGR: intrauterine growth restriction; wg: weeks of gestation; IFD: intrauterine fetal death; aCL: anticardiolipin antibodies; anti-β2-GPI: anti-β2-glycoprotein I antibodies; LLAC: lupus-like anticoagulant.
Higher IUGR frequency in prior pregnancies of aPS/PT+ patients
Forty-seven of the 55 recruited patients (85%) had previous pregnancies, for a total of 114 pregnancies. Pregnancy complications were more frequent in aPS/PT+ than aPS/PT- patients. The late pregnancy complications, IUGR in particular, were significantly higher in prior pregnancies of aPS/PT+ patients (Table 1B). This was not associated with the simultaneous presence of various aPL with different specificity: 17/47 (36%) patients had an extended aPL repertoire and 30/47 (64%) had a limited aPL repertoire (patients with 1, 2, or 3 autoantibodies specificity). The frequency of late pregnancy complications, and in particular of IUGR, did not differ between patients with extended or limited autoantibodies repertoires (Table 3). For example, 8 of 17 patients (47%) with extended aPL repertoire and 12/30 patients (40%) with limited repertoire had IUGR. In the prospectively followed pregnancies, the rate also did not differ (data not shown).
Obstetrical history in patients who had a previous pregnancy with extended or limited aPL repertoire. Values are n (%) unless otherwise specified.
DISCUSSION
Our study provided an evaluation of the clinical effects of the presence of aPS/PT in women with APS seeking conception and who were prospectively followed during pregnancy. Unconventional aPL are attracting increasing attention as biomarkers and possibly as clues to the pathogenesis of APS. However, not many studies had prospectively followed pregnancies in patients with APS and the informative potential of most unconventional aPL about the patient prognosis or the need for additional treatments has been so far unclear. To our knowledge, this is the largest prospective study that evaluated the presence of aPS/PT, and the maternal and fetal outcomes in women with well-characterized APS, both clinically and in the laboratory, carried out in 2 Italian hospitals. Our study included a representative group of patients with APS looking for counseling, who experienced in their history the most common thrombotic and obstetric complications associated with the presence of the autoimmune disease35,36, and a well-balanced group of patients with potential confounding factors, such as arterial HTN37. This composition was fit for assessing the effect of the presence of aPS/PT antibodies on a subsequent pregnancy. We included 2 patients who had 2 early miscarriages only and who were willing to participate. Their inclusion did not influence the statistical treatment of the data or the results.
In our cohort, aPT/PT were the prevailing aPL. As expected38, there was a significant association of aPS/PT positivity with the presence of LLAC. The aPS/PT are significantly more frequent, show higher levels in subjects with multiple aPL specificities, and are often found associated with “triple positivities”30. This condition is possibly the best-characterized indicator of the risk associated to the presence of aPL39. In our study cohort, 17 of 33 aPS/PT+ patients (51%) also had triple positivity and 25 (76%) were LLAC-positive.
The relative abundance of autoantibodies targeting various epitopes of a complex autoantigen might reflect epitope spreading, a well-characterized event in sustained human autoimmunity40,41 and in APS in particular42. An ample and diversified array of autoantibodies might represent an additional risk factor, increasing the probability that pathogenic autoantibodies are generated. In our patients, however, the number of aPL was not per se associated to pregnancy complications; neither was the triple positivity sufficient to identify patients at higher risk. In contrast, the presence of aPS/PT antibodies was significantly associated with late pregnancy complications, IUGR, and preeclampsia.
Patients followed in our study have been carefully monitored by multidisciplinary teams of experts and treated both periconceptionally and during the pregnancy according to the available gold standards and recommendations43. The pregnancy outcome was, as expected35,36, substantially better compared to the outcome of prior pregnancies in the same patients. Despite the improvement, where early complications of pregnancy are concerned (Table 2), IUGR and preeclampsia rates remained high. The aPS/PT might represent a valuable biomarker for the risk of complications appearing late in pregnancy, possibly because these antibodies reflect and are involved in pathogenic events that are less sensitive to the available treatments.
The aPS/PT might be able to interfere at various levels with regulatory networks involved in microvascular homeostasis14,44,45,46. Further studies will thus be necessary to identify the molecular constraints underlying the association between aPS/PT and treatment-resistant pregnancy complications.
Histological assessment of the placental tissues is consistent with more evident features associated to hypoxic damage in patients with aPS/PT, possibly as a result of a more prominent involvement of the microvasculature47. Thus additional treatments might be considered in patients presenting with aPS/PT antibodies before conception, including hydroxychloroquine, which might be safe and effective at reducing the deleterious effects of complement activation in the placental tissue13,48,49.
Our findings suggest that aPS/PT antibodies may be promising aPL-related pregnancy complication markers, for IUGR/preeclampsia in particular, and could help identify patients who may require additional treatment in advance. However, our findings should be verified in larger patient groups. In addition, the mechanisms by which they interfere with pregnancy need to be further studied.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
We thank INOVA Diagnostic Inc., San Diego, California, USA, for the generous gift of the aPS/PT IgG and IgM assays.
Footnotes
This work has been supported by the Ministero dell’Istruzione, dell’Università e della Ricerca and the Ministero della Salute (programma per la ricerca finalizzata).
- Accepted for publication February 16, 2018.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.