
Abstract
Objective. Nonadherence is currently an underrecognized and potentially modifiable obstacle to care in juvenile idiopathic arthritis (JIA). The purpose of our study was to design and implement a standardized approach to identifying adherence barriers for youth with JIA across 7 pediatric rheumatology clinics through the Pediatric Rheumatology Care and Outcomes Improvement Network (PR-COIN) and to assess the frequency of adherence barriers in patients and their caregivers across treatment modalities.
Methods. An iterative process using coproduction among parents and providers of patients with JIA was used to design the Barriers Assessment Tool to screen for adherence barriers across 4 treatment modalities (i.e., oral medications, injectable medications, infusions, and physical/occupational therapy). This tool was implemented in 7 rheumatology clinics across the United States and patient responses were collected for analysis.
Results. Data were collected from 578 parents and 99 patients (n = 44 parent-child dyads). Seventy-seven percent (n = 444) of caregivers and 70% (n = 69) of patients reported at least 1 adherence barrier across all treatment components. The most commonly reported adherence barriers included worry about future consequences of therapy, pain, forgetting, side effects, and embarrassment related to the therapy. There was no significant difference between endorsement of barriers between parents and adolescents.
Conclusion. Implementing a standardized tool assessing adherence barriers in the JIA population across multiple clinical settings is feasible. Systematic screening sheds light on the factors that make adherence difficult in JIA and identifies targets for future adherence interventions in clinical practice.
- JUVENILE ARTHRITIS
- PATIENT COMPLIANCE
- QUALITY IMPROVEMENT
Juvenile idiopathic arthritis (JIA) is the most common pediatric rheumatic condition. It is composed of 7 unique phenotypic subtypes with varied clinical course severities and spectrums of morbidity1. The treatment landscape in JIA has rapidly evolved since the advent of biologic medications. Clinical trials focused on safety and efficacy have proven favorable prognostic outcomes when medications are administered with controlled dosing2,3,4,5. However, despite treatment advances, only 16–64% of the disease course is spent in a clinically inactive state when assessed across all JIA subtypes6. Even in patients who attain inactive disease status, the risk of flare within 1 year is 40%7. Moreover, longterm outcomes into adulthood reveal sustained limitations in functioning, resulting in reduced health-related quality of life (HRQOL)8,9.
Nonadherence represents a modifiable factor that could significantly affect outcomes, including morbidity, mortality, costs, healthcare decision making, and HRQOL10. Adherence is defined as the extent to which a person’s behavior corresponds with provider health recommendations11. While adherence rates vary among general pediatric populations, average adherence is 50%12. Studies of adherence in JIA have been limited, with most focusing on self- and parent-reported adherence, which tend to be inflated relative to more objective measures (e.g., electronic monitoring). One study assessing adherence to nonsteroidal antiinflammatory medications in newly diagnosed patients with JIA classified 52% of patients as adherent13. Interestingly, even more sophisticated therapies, such as biologic medications and disease-modifying antirheumatic drugs, have suboptimal rates of adherence, with a mean medication refill possession ratio of 46.9% and 65.7% for subcutaneous methotrexate and injectable tumor necrosis factor-α inhibitors, respectively14. Factors predicting nonadherence in JIA include delayed time to therapeutic efficacy, fear of adverse effects, chronicity of disease, and complex and costly regimens15,16,17. Conversely, factors associated with higher perceived adherence included perceived helpfulness of treatment, lower disease severity, and younger age of the child18. Despite what is known about nonadherence in JIA, critical gaps remain in translating research findings into clinical practice. In fact, pediatric rheumatologists are unlikely to address adherence barriers in routine practice, especially when compared to treatment efficacy/performance16.
Identification of JIA-specific barriers is an important first step in adherence promotion, especially in clinical practice. The Health Belief Model postulates the importance of perceptions of barriers as a factor contributing to nonadherence, and served as a theoretical framework that prompted the systematic screening of barriers in our current study19. Research has demonstrated that as the number of patient-reported barriers increases, adherence to treatment decreases20. One study noted the effect of cumulative barriers, finding that each additional barrier to adherence increased the likelihood of nonadherence by about 30%21.
Further, we know from pediatric and adult literature that repeated measures of barriers to adherence are necessary because individual barriers are variable as the patient ages and disease status evolves22,23. Barriers identified in the larger pediatric literature (e.g., asthma, cystic fibrosis, solid organ transplant, inflammatory bowel disease) include forgetting, medication side effects or palatability, child oppositional behaviors, and interference in daily life24,25,26. Understanding and identifying individual barriers will allow providers to target specific areas for intervention to promote adherence and self-management. Metaanalyses have demonstrated that multicomponent interventions to address adherence can improve health outcomes and healthcare use27,28. Unfortunately, few studies have identified barriers to target for multimodal adherence interventions in JIA, especially since the advent of biologic medications.
Our current study used quality improvement methodology to design and test a Barriers Assessment Tool (BAT) specific for the JIA population, as well as to identify patient and parent-reported adherence barriers across several JIA treatments. The collaboration of a multicenter team of pediatric rheumatology providers, psychologists, and parent representatives was organized by the Pediatric Rheumatology Care and Outcomes Improvement Network (PR-COIN). This international collaborative learning network is centered on the cooperative development and implementation of management strategies to improve the outcomes and quality care for patients with JIA. PR-COIN provided formal education and hands-on training in the field of self-management across 7 of 18 PR-COIN member sites prior to the development of the adherence barriers screening tool. Our hypothesis was that this barrier assessment tool would comprehensively identify adherence barriers that would not have otherwise been discussed during a routine clinic visit. The second goal was to facilitate the systematic distribution of the barriers assessment across all 7 sites. Finally, our team aimed to assess for concordance of adherence barriers across caregiver and patient dyad respondents. Consistent with prior literature, it was hypothesized that forgetting, side effects, and interference with daily life would be the most highly endorsed barriers across various treatment components (e.g., oral medications, injections, infusions, and physical and occupational therapy).
MATERIALS AND METHODS
Design of the BAT
Seven centers (Children’s Mercy Kansas City, Cincinnati Children’s Hospital Medical Center, Cohen Children’s Medical Center, Levine Children’s Hospital, Stanford Children’s Hospital, Nationwide Children’s Hospital, and Penn State Children’s Hospital) were involved in the design and implementation of the BAT through PR-COIN. A multidisciplinary coproduction model was used, including pediatric rheumatologists, nurse practitioners, psychologists, and parents of children with JIA. Coproduction is a collaborative approach in which everyone including patients, caregivers, and providers are involved in the project initiative from conceptualization to implementation. While this exact self-report measure was newly developed for this project, design of the BAT was based on prior work in other pediatric subspecialties24,26,29,30. Validation studies have demonstrated that adherence barriers are strongly correlated with both adherence and health outcomes (e.g., organ rejection, seizures)26,29,30. An iterative process through monthly teleconferencing was used to create, modify, and individually tailor the BAT for patients with JIA. Engagement of the families in the feedback and design process was valuable in tailoring a tool that would be specific to this unique population. Important redesign feedback included reconfiguring the tool to ease usability, as well as altering the checklist to include JIA-specific barriers across various treatment components. Streamlined design was of paramount importance to the coproduction team, with emphasis on keeping the tool limited to 1 page in length. Care was taken to limit word density and check-boxes were used to further simplify the tool. An important goal of the team was to avoid contributing to “form fatigue” and to provide the most information with the least amount of patient or caregiver effort. The final BAT is a 17-item checklist spanning 4 treatment modalities: oral medications, injections, infusions, and physical/occupational therapy. Barrier themes include regimen characteristics (i.e., palatability and complexity), logistical impedances, patient oppositional behavior, social difficulties and efficacy concerns. Although the general layout remained consistent between the tools designed for other patient populations (e.g., kidney transplantation and epilepsy), specific barriers and treatment regimens were added. Examples of JIA-specific regimens included the addition of injections, infusions, and physical/occupational therapy. Worry about future side effects and concern about future child-bearing were barriers that patients and caregivers independently identified in JIA, in addition to more universal barriers (i.e., forgetting or poor taste). Two versions of the assessment were designed, 1 for caregivers and 1 for children 10 years old or older. Age 10 was chosen based on developmental ability to independently complete the forms.
Implementation of the BAT
The BAT was successfully administered to patients and/or parents at the 7 PR-COIN centers. Cincinnati Children’s Hospital Medical Center served as the central institutional review board (IRB) and the coordinating center for the study. The study protocol was first approved through the central IRB (IRB #2010-2811). Additionally, local IRB approval of the protocol was obtained for the following sites: Cohen Children’s Medical Center, Levine Children’s Hospital, Stanford Children’s Hospital, Nationwide Children’s Hospital, and Penn State Children’s Hospital. All scheduled patients with JIA during the 7-month testing period (March–September 2016) were eligible to participate. Participants represented all JIA subtypes and ages and had to be currently receiving 1 or more of the treatment modalities (oral medications, injections, infusions, or physical/occupational therapy) at the time of participation. Informed consent was not required by respective institutions because this study was undertaken as a quality improvement initiative. All parents were asked to complete a BAT, and children 10 years old or older were given their own form to collect parent-patient dyad responses. Improvement principles and tools were applied across sites to facilitate the work, including development of a Key Driver Diagram, process flow maps, iterative Plan-Do-Study-Act cycles based upon key drivers, to design reliable implementation processes. The Model for Improvement was used as the framework to guide the process and improve integration into care delivery31. The primary process measure was the percent of indicated BAT that were successfully collected. Because this was a quality improvement initiative, patient identifiers were not linked to completed questionnaires, and thus demographics (i.e., JIA subtype, age, race, disease severity) could not be obtained in the current project.
Teleconferencing was used to share data and the experience of implementation in varying busy clinic flow scenarios. The group discussed ways to improve execution. Site-specific processes of implementation varied based on local staffing resources; however, broad solutions included clearly defining staff responsibilities and linking distribution of the assessment to an already established process, such as morning clinic setup. Although there was no measurement of the visit time burden of introducing this tool, there was provider feedback that the tool allowed a swift inventory of patient or parent concerns that led to productive conversations. While repeat measurements from the same patient were possible, this was unlikely given the short testing time frame in relation to typical JIA followup appointment timing.
Statistical analysis of BAT responses
Descriptive statistics, including means, SD, and frequencies, were used to examine barriers. Each barrier was scored as either 0 (not endorsed) or 1 (endorsed). We used paired-sample t tests to assess frequency differences in barriers across treatment modalities. McNemar tests were conducted to examine differences in the endorsement and concordance between parent-child dyads. Analyses were performed with the Statistical Package for Social Sciences (SPSS), version 2432.
RESULTS
Endorsement and types of barriers
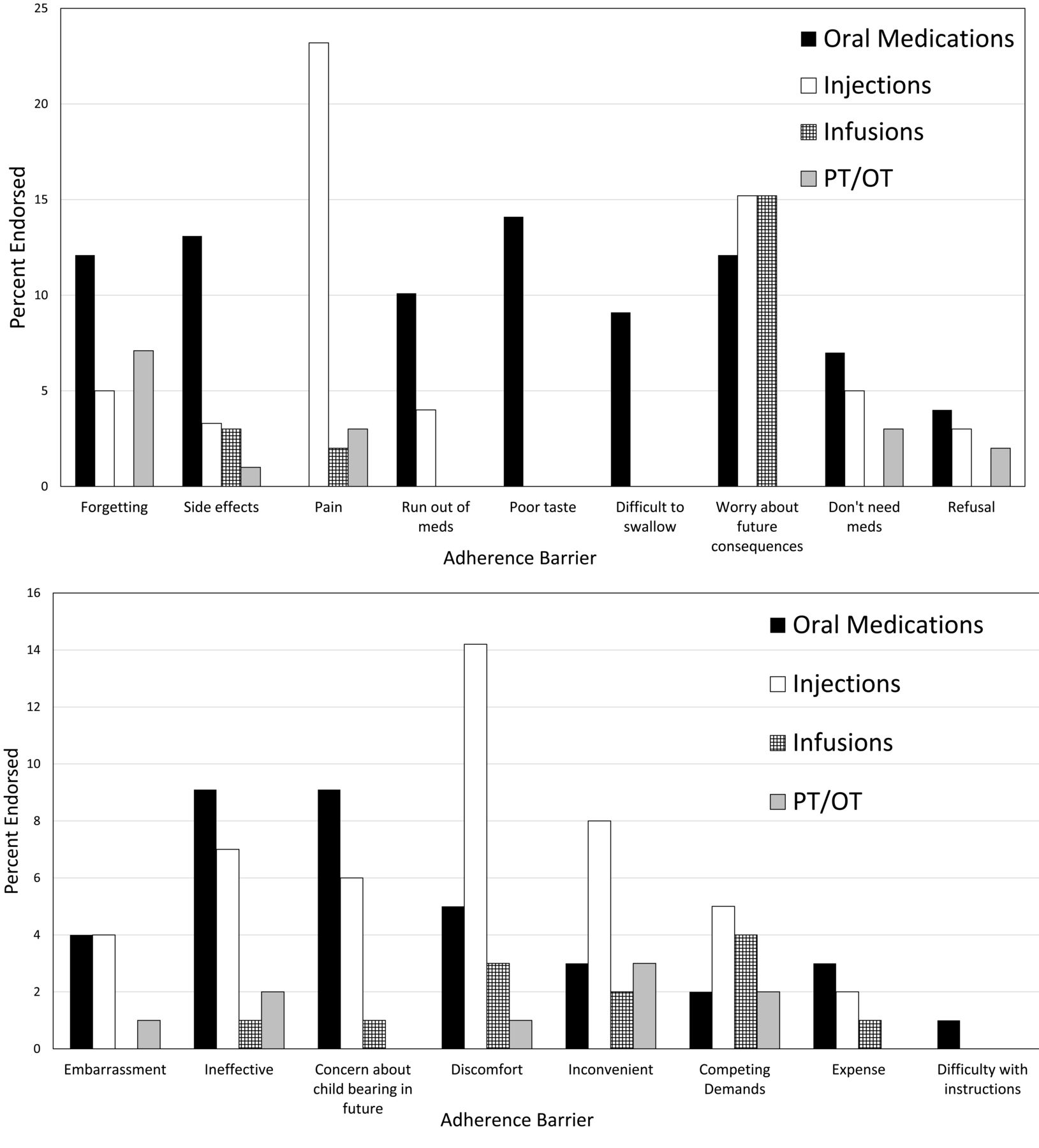
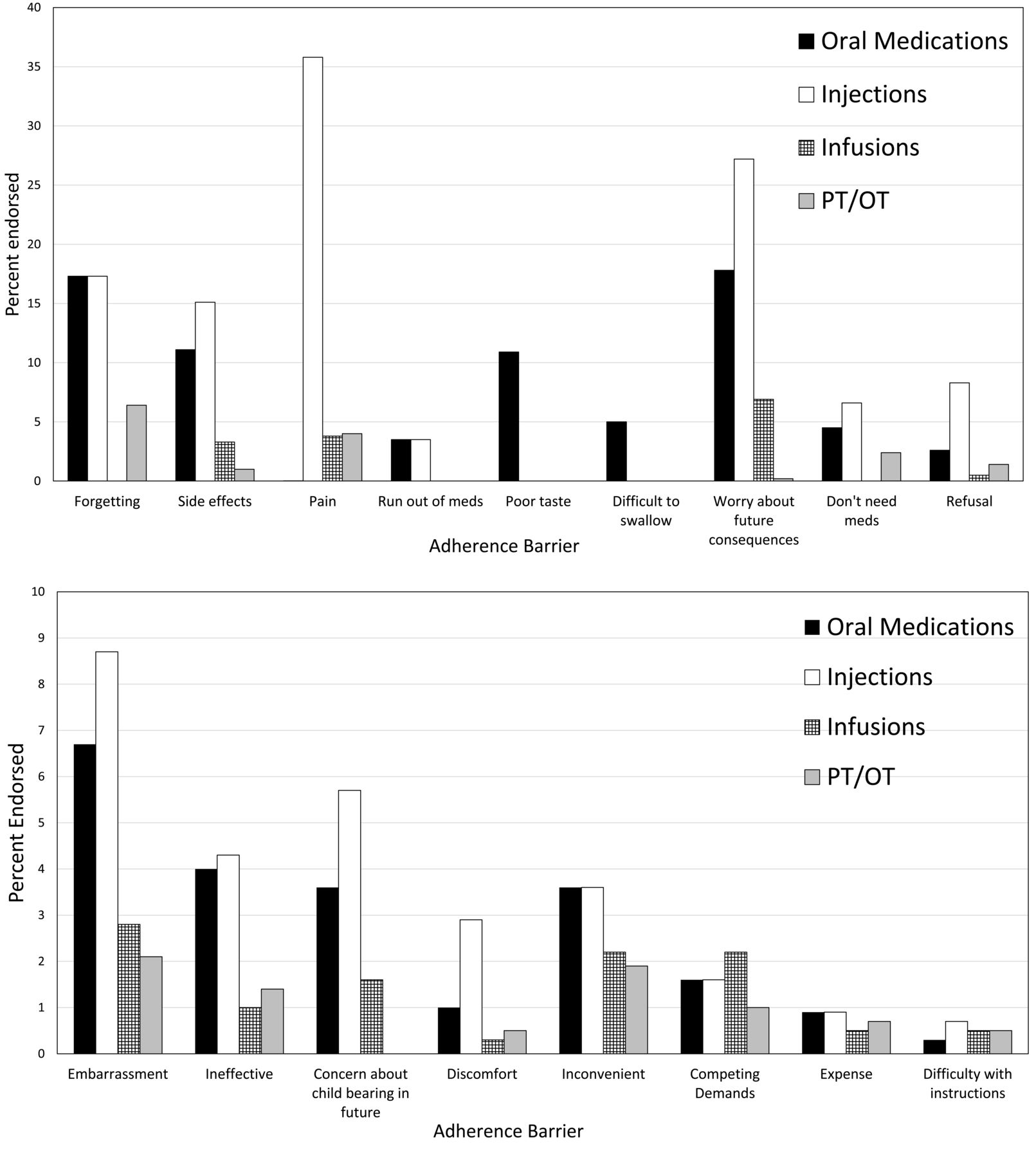
A total of 677 barrier assessments were collected out of 1148 eligible patients over the study testing period (59% completion rate). The collected assessments included 578 parent and 99 patient responses, with 44 identified parent-child dyads across the 7 participating PR-COIN sites. Of those respondents, 76.8% of parents (n = 444) and 69.7% of patients (n = 69) reported at least 1 adherence barrier across all treatment components. The most commonly endorsed barriers among patients and parents stratified by treatment modality are presented in Figure 1 and Figure 2. Notably, pain, forgetting, side effects, worry about future treatment consequences, and embarrassment were the top barriers among both parents and patients.

Frequency of parental-endorsed barriers across treatment modalities. Percentages of most common adherence barriers endorsed on the Barriers Assessment Tool by parental respondents. PT/OT: physical therapy/occupational therapy.
{kind=link}
{kind=link}
Frequency of patient-endorsed barriers across treatment modalities. Percentages of most common adherence barriers endorsed on the Barriers Assessment Tool by patient respondents. PT/OT: physical therapy/occupational therapy.
Barriers to oral medications were endorsed in 44.6% (n = 258) of parents and 47.5% (n = 47) of patients. Top oral medication barriers included worry about future consequences, forgetting, and poor taste. Barriers of any type for injectable medications were endorsed in 52.5% (n = 304) of parents and 40.4% (n = 40) of patients. Infusion barriers were endorsed in 12.7% (n = 73) and 9% (n = 9) of parents and patients, respectively. The most highly endorsed barriers for both injectable and infusion medication were worry, pain, and side effects. Barriers to physical and occupational therapy were noted in 13% (n = 75) of parents and 14% (n = 14) of patients. The top reported barriers for physical and occupational therapy were forgetting, pain, and believing the therapy is unnecessary.
Most parents (mean = 2.83 ± 3.20) and patients (mean = 2.80 ± 2.90) endorsed fewer than 3 barriers. The number of injection barriers endorsed (mean = 1.37 + 1.73) was significantly higher compared to oral medications (mean = 0.95 + 1.43; p < 0.01) in parents. No significant differences were found among treatment modalities for the frequency of patient-reported barriers.
Caregiver-patient convergence on barriers to adherence
McNemar tests were performed to examine differences in the endorsement of barriers between the 44 parent-patient dyads. Separate tests evaluated for agreement for each barrier per treatment modality. Both parents and patients tended to agree on barriers endorsed within categories of therapy. No significant differences were found between the barriers endorsed for oral medications (16% vs 19%), injections (24% vs 22%), infusions (3% vs 4%), or physical/occupational therapy (10% vs 11%) between the dyads.
DISCUSSION
Our current study sought to systematically assess parent and patient treatment barriers in JIA across individual treatment modalities through the leverage of a learning network. The majority of participants expressed at least 1 barrier to a treatment modality, which highlights the importance of such a screening tool to encourage discussion of treatment adherence in clinical care. This is a new addition to our current care framework that does not currently emphasize screening for adherence barriers as compared to addressing therapeutic performance16.
Common barriers endorsed included largely actionable concerns, such as poor taste, forgetting, pain, and difficulty managing side effects. Evidence-based treatments to address several of these barriers have been developed and have been found to be efficacious33,34,35. The provision of intervention tools to address these common barriers with patients and caregivers in clinical practice is critical to addressing the needs of the patient and improving adherence. A pilot adherence initiative in kidney transplantation has found that systematically identifying and addressing adherence barriers to immunosuppressant therapy improved population-based outcomes (i.e., late organ rejection)36.
The most commonly endorsed barrier across all treatment modalities was worry about future consequences of receiving the therapy. This is a JIA-specific barrier that has not been identified in other pediatric populations, but is quite salient with the use of biologics, which have relatively short-term data regarding adverse effect risks in children37,38. Familial assurance regarding appropriate therapeutic decisions balanced against the risk of longterm disease-related damage is largely up to individual providers, making this a variable experience overall39. One qualitative study of pediatric patients that prescribed tumor necrosis factor-α inhibitor biologics highlighted that the current education and decision-making process in rheumatology and gastroenterology clinics ultimately led to longterm worry and concern surrounding therapy40. Families acquire information about prospective therapies from multiple sources, including medical care providers, the Internet, and social contacts, making clear access to unbiased and timely information more important than ever41. Shared decision-making techniques could be beneficial in reducing concern and uncertainty and ultimately improve adherence to treatment recommendations. Systematically implementing patient-centered tools or decision aids for treatment education is one way to navigate varying patient and provider approaches42.
Interestingly, injectable medications, which are most often given in the home by either the patient or parent, had the highest endorsement of barriers, even when compared to hospital infusion therapy. These findings suggest that home-based injections may create a more burdensome experience for families when compared to hospital infusions. This may be counterintuitive because hospital infusions require additional transportation and time for families. While common injection barriers include pain, discomfort, and refusal, worry about future consequences was also markedly higher in families receiving injectable medications compared to infusion therapy. It is possible that the actual act of caregivers or patients administering injections, rather than hospital staff, amplifies these concerns despite the added convenience that an in-home injection could provide. While this is the first time a comparison of perceived worry between injectable and infusion therapy has been attempted, the effect of the general care of patients with JIA on psychological health and quality of life for caregivers has been established in our population43. This finding could suggest that increased training initiatives and education surrounding injection administration may be helpful to prevent such barriers.
Although no differences were found between parents and patients in either number or type of barriers expressed, we still believe it is important to gather both perspectives. It has been described that adolescents with JIA and their parents exhibit meaningful differences in their responses regarding treatment helpfulness and adherence44,45. Formal screening and discussion of potential discrepancies may help to facilitate communication between provider, patient, and caregiver to better understand differing goals of therapy. While there is variability in the age at which adolescents transition to assuming more responsibility for their medication and exercise regimens, this is an important time to foster interest in their own care and to build the needed skills. In a study involving initiation of biologic therapy in JIA and Crohn disease, most adolescents valued the involvement of their physician or parent in treatment decisions, but given the chance would have preferred more active participation and dedicated education46.
There are some notable limitations to our study that deserve consideration. While our BAT was newly designed for this project without formal validation, the themes depicted in our tool have been systematically and rigorously validated in other pediatric chronic illness populations26,29,30. A correlation of our tool with quantitative measurement of adherence would have been optimal to translate endorsed barriers with actual behavior. Self- or parental-reported adherence would have also added to the richness of these data. Additionally, participant demographics were not collected in keeping with restrictions of a multicenter quality improvement project design; thus, we were unable to examine differences in barriers by patient age, disease duration, disease severity, and treatment regimen complexity. Moreover, while our sample size was large, there were a small number of parent-patient dyads to assess for comparisons. Regardless, the multicenter design and unique coproduction model that was used for this study make it novel and innovative in the field of JIA adherence research.
By harnessing the collective coordination of a learning network, PR-COIN was able to lead the design and implementation effort of this BAT as part of a large, multicenter self-management initiative. Tracking introduction of the tool across sites allowed us to ensure feasibility in delivery of the tool across 7 clinical settings. Both parent and provider feedback of the tool’s usability during both the design and delivery stages indicated that it can be successfully used to screen for and facilitate discussions surrounding nonadherence in any pediatric rheumatology clinic. Since its development, the BAT has been distributed for use among all 18 PR-COIN sites as part of a larger self-management optimization package. Access to this tool for research or clinical purposes is available through the authors.
Future directions of this work will include design and testing of complementary adherence promotion tools to contribute to a larger systems-level adherence initiative. For example, multiple ways to improve taste or to prevent forgetting medications have been used to improve adherence47,48. Increasing dialogue between pediatric rheumatology providers and patients/families to identify and test various solutions based on individual needs (e.g., text messages to remind people to take medications if they like technology, or pairing medications with routines such as brushing teeth) could be beneficial. Further, use of a standard set of adherence tools by clinical providers would systematize adherence solutions across patients. As with other chronic pediatric illnesses, formalizing adherence screening as a part of clinical care in JIA would likely continue to improve outcomes of this population. In JIA specifically, patient-perceived adherence was related to better HRQOL, particularly with gross motor and psychosocial functioning44. Better adherence has also been linked to improvements in short-term outcomes in JIA including lower joint counts, improved physical functioning scores, and parental perception of global improvement49. These findings continue to support the investigation and clinical emphasis in addressing adherence barriers in JIA. It is our intention to facilitate and ease discussions surrounding adherence behaviors and provide a usable system that will translate to more effective care in the JIA population.
Footnotes
A copy of the Barriers Assessment Tool is available from Dr. E.M. Morgan (Esi.Morgan_DeWitt{at}cchmc.org) or J. Taylor (janalee.taylor{at}cchmc.org)
Supported in part by grant funding from the Center for Education and Research on Therapeutics (CERTs), AHRQ, Grant #419HS021114 (PI: Carol Lannon).
- Accepted for publication November 23, 2017.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.