
Abstract
Objective. This study aimed to test fecal calprotectin (FC) as a screening tool to identify inflammatory bowel disease (IBD) among patients with juvenile idiopathic arthritis (JIA).
Methods. FC level < 100 g/kg was considered normal. Patients with 2 consecutive FC dosage ≥ 100 g/kg underwent endoscopic evaluation.
Results. There were 113 patients with JIA enrolled. FC was raised in 7 patients out of 113. All patients had IBD. In 3/7 patients, high FC levels were the only sign consistent with IBD.
Conclusion. FC is a useful, economical, and noninvasive diagnostic tool to identify JIA patients with underlying IBD.
- JUVENILE IDIOPATHIC ARTHRITIS
- INFLAMMATORY BOWEL DISEASE
- FECAL CALPROTECTIN
- CHRONIC ARTHRITIS
- CROHN DISEASE
Juvenile idiopathic arthritis (JIA) is the most common rheumatic disease of childhood1. Inflammatory bowel disease (IBD) may present in childhood in 20% of cases2 and extraintestinal symptoms are common in patients with IBD3; in particular, arthritis can be the first sign of IBD4. Calprotectin is mostly found in the cytoplasm of neutrophils, macrophages, and activated monocytes. Fecal calprotectin (FC) reflects inflammation of intestinal mucosa. During gut inflammation, FC is released from activated inflammatory cells into intestinal lumen5. FC has already been tested as a screening tool to identify IBD among patients with gastrointestinal (GI) symptoms6. It has been demonstrated that FC has a high sensitivity for the diagnosis of pediatric IBD and it is more specific and sensitive than inflammatory blood markers7. However, no data exist about the use of FC in detecting IBD among patients with JIA. Our study aimed to test FC as a screening tool for early detection of IBD among patients with JIA. Secondary outcomes were to assess the range of FC in subjects with confirmed IBD and to compare the clinical features of JIA patients with proven IBD versus those without IBD.
MATERIALS AND METHODS
This is a retrospective study and according to Italian law, research ethics board (REB) approval was not required; a notification was provided to the local REB.
All patients with JIA diagnosed according to International League of Associations for Rheumatology criteria8 and admitted to the Rheumatology Service of the Institute for Research and Health Care Burlo Garofolo from January 2015 to August 2016 were enrolled. Patients with systemic JIA were excluded. FC evaluation in our clinic is normal clinical practice. At each visit, the following data were collected: age at JIA onset, presence of antinuclear antibodies at onset, presence/absence of uveitis, sex, JIA type, arthritis activity [measured with Juvenile Arthritis Disease Activity Score (JADAS) 27 score]9 time from JIA onset, age, presence of GI symptoms, family history of IBD, weight loss, growth retardation, viral infection in the last 3 weeks, concomitant and previous treatment, dosage of cell blood count, inflammatory markers, and serum immunoglobulins.
The stool samples were stored at −20°C. The technique used was a quantitative enzyme immunoassay (Thermo Phadia EliA with a cutoff ≥ 100 g/kg). FC levels < 100 g/kg were considered negative. Patients with FC ≥ 100 g/kg were asked to repeat the test to confirm. Patients with a second positive test underwent abdominal ultrasound and intestinal endoscopy.
Statistical analysis was performed with R-3.3.1 software. Pearson linear correlation test and nonparametric Kruskal-Wallis tests with related p values were calculated. A p value < 0.05 was considered statistically significant.
RESULTS
There were 113 patients with JIA enrolled. Seven out of 113 (6%) were found affected by IBD (Table 1). After the first FC dosage, 90 patients presented calprotectin levels < 100 g/kg. Twenty-three patients presented FC levels > 100 g/kg and the test was repeated. Sixteen patients presented a normal value and were considered healthy, while the other 7 patients’ FC dosage was again positive; in all these patients, abdominal ultrasound, endoscopy, and histology confirmed IBD diagnosis. All patients presented with Crohn disease. Four out of 7 were initially classified as affected by enthesitis-related arthritis (ERA), 2 as oligoarticular JIA, and 1 patient as undifferentiated arthritis (Table 2). ERA was found to be a significant risk factor for IBD (OR 69.33, 95% CI 8–538, p < 0.0001). Only 3 patients (43%) presented diarrhea, fecal blood positivity, or abdominal pain. Among them, only 1 patient was receiving treatment with etanercept (ETN); the other 2 were receiving no therapy. One patient had growth retardation without other intestinal symptoms and without treatment. Three patients (43%) were completely asymptomatic. Among these latest patients, 1 had active arthritis (ERA) irrespective from treatment. Two patients were receiving intraarticular corticosteroid injections while the last one was treated with infliximab. Evaluating all patients receiving ETN (n = 21), we found no correlation between this drug and IBD onset (OR 0.83, 95% CI 0.1–7.3; p = 1.00).
Clinical characteristics of patients with JIA and underlying IBD.
Clinical characteristics of JIA patients with or without underlying IBD. Values are n (%) or mean (SD, range).
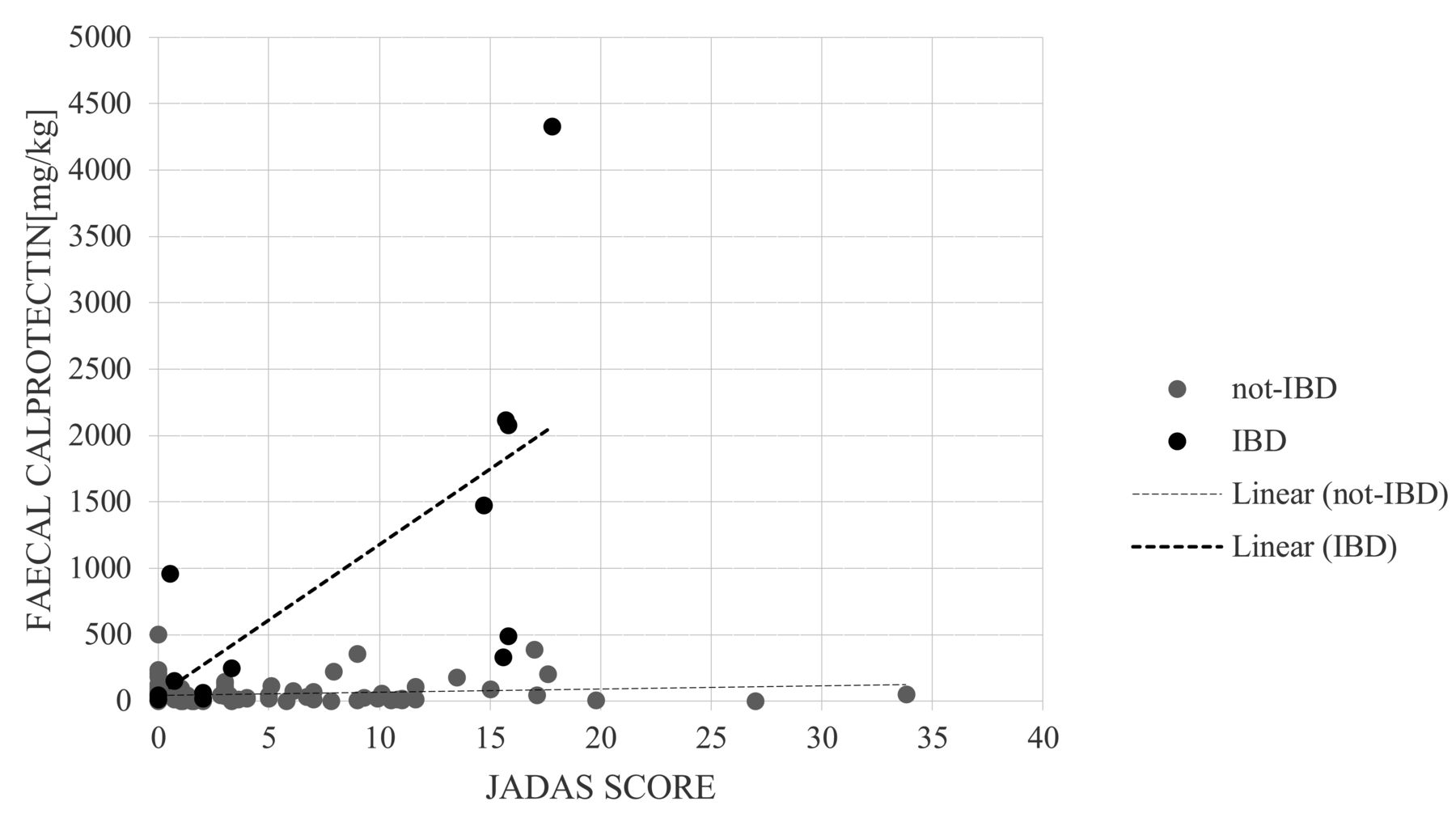
All IBD patients presented FC value ≥ 250 g/kg; in 4 patients FC value was > 1000 g/kg (median 1500 g/kg, range 250-4334 g/kg; Table 1). FC was found to be associated with disease activity valued with JADAS score (correlation index 0.69%, 95% CI 0.22–0.90, p = 0.009; Figure 1). Other laboratory variables taken into account demonstrate that patients with IBD generally had higher systemic inflammation compared to those without IBD (Table 2).

{kind=link}
Relationship between FC and JADAS score among a population of patients with JIA, showing an association between FC values and JIA activity (correlation index 0.69%, 95% CI 0.22–0.90; p = 0.009). FC: fecal calprotectin; JADAS: Juvenile Arthritis Disease Activity Score; JIA: juvenile idiopathic arthritis; IBD: inflammatory bowel disease.
DISCUSSION
Arthritis is one of the most common extraintestinal complications of IBD, and it may precede the onset of GI symptoms. Although peripheral oligoarthritis and ERA10 are the most common chronic arthritis patterns associated with IBD, other arthropathies have been associated with IBD as well11. For this reason, and because JIA is a diagnosis of exclusion, IBD should always be excluded at JIA onset. However, data on FC levels in the assessment of intestinal inflammation among patients with JIA are limited. Although Biskou, et al12 found that FC levels are not raised in children with JIA, it has been demonstrated that FC levels could be higher in JIA patients because of their use of nonsteroidal antiinflammatory drugs; however, levels returned to normal values after drug withdrawal13. Stoll, et al found that FC levels were higher in children with ERA if compared to patients with nonspondyloarthritis subtype and unrelated connective tissue diseases, and noninflammatory control subjects14. These findings were also found in our study where ERA pattern showed the higher association with IBD. However, Stoll, et al did not confirm IBD diagnosis. On the contrary, to our knowledge, our data are the first to associate high FC levels with histological IBD in patients previously diagnosed as JIA. It is also important to underline that only 3 patients complained of intestinal symptoms such as abdominal pain, fecal blood, or diarrhea. One patient had only growth retardation without any other clinical complaints, and 3 patients were completely asymptomatic. One among these last patients had uncontrolled arthritis. These findings indicate that IBD may be completely asymptomatic among patients with JIA, suggesting that a screening test for these patients may be useful. Interestingly, the patients with underlying IBD presented higher erythrocyte sedimentation rate, C-reactive protein, and IgA levels, as well as lower hemoglobin levels and higher platelet count if compared with patients without IBD, suggesting a systemic underlying inflammation. Moreover, JADAS score was also higher in JIA patients with IBD, showing that the clinical control of chronic arthritis is more difficult if IBD is present.
Because we did not evaluate with endoscopy those patients with at least 1 normal FC, we cannot discuss the sensitivity of FC. However, many authors have found that FC has a sensitivity of 100%15,16,17, while a metaanalysis has previously shown that sensitivity for the diagnostic utility of FC during the investigation of suspected pediatric IBD was 97.8% if FC cutoff value is > 100 mcg/g7. Moreover, Van de Vijver, et al has previously demonstrated that among patients with GI complaints, FC could be safely used to rule out IBD in children without referring to endoscopy; in particular, they found that “a normal calprotectin level reduces the probability of IBD to zero”18. It is important to stress that in our study, all patients with FC levels > 250 g/kg presented IBD. On the other hand, FC levels were always < 250 g/kg in the 16 patients with FC positivity at the first dosage only.
FC is routinely used among patients with JIA in our institute, and all patients with JIA are constantly clinically followed for the appearance of symptoms attributable to IBD. At 16 months after the end of the study, all the 106 patients who did not have IBD had not shown any clinical symptom consistent with IBD nor a rise in FC levels.
Our study has some limitations. The number of patients is small, and JIA patients with normal FC values did not undergo IBD diagnostic evaluation. It is important to underline, however, that it could not be considered ethical to perform such invasive procedures on patients with no GI complaint and with normal FC levels. FC has a very wide specificity and the possibility that chronic bowel inflammation may have normal FC is extremely low18. Our results need to be confirmed with larger prospective cohorts.
Detecting IBD-related arthritis is important. Its treatment is different from JIA. ETN is an anti-tumor necrosis factor-α inhibitor that is very successful in the treatment of JIA, but it does not act on bowel inflammation19; so far, for IBD-related arthritis, infliximab or adalimumab are the treatments of choice. Further, IBD-related arthritis is often linked to gut inflammation activity, and it is mandatory to treat GI symptoms to control joint inflammation20. Because most JIA patients with underlying IBD may not present with GI complaints, we suggest that FC screening should be performed at onset and then periodically.
With our study, we proved how FC is a useful, economical, and noninvasive diagnostic tool to identify patients with JIA to refer for further GI investigations. FC ≥ 250 g/kg was specific for IBD; all 7 of such patients had IBD.
- Accepted for publication March 7, 2018.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.