
Abstract
Objective. Rebound may occur in patients with psoriatic arthritis (PsA) who discontinue TNF inhibitor (TNFi) therapy in low disease activity (LDA).
Methods. Using physician and patient reports, we quantified rebound following TNFi discontinuation [defined as Clinical Disease Activity Index (CDAI) score > 10 or TNFi restart] and time to rebound in adults with PsA in LDA (CDAI score ≤ 10) at TNFi discontinuation.
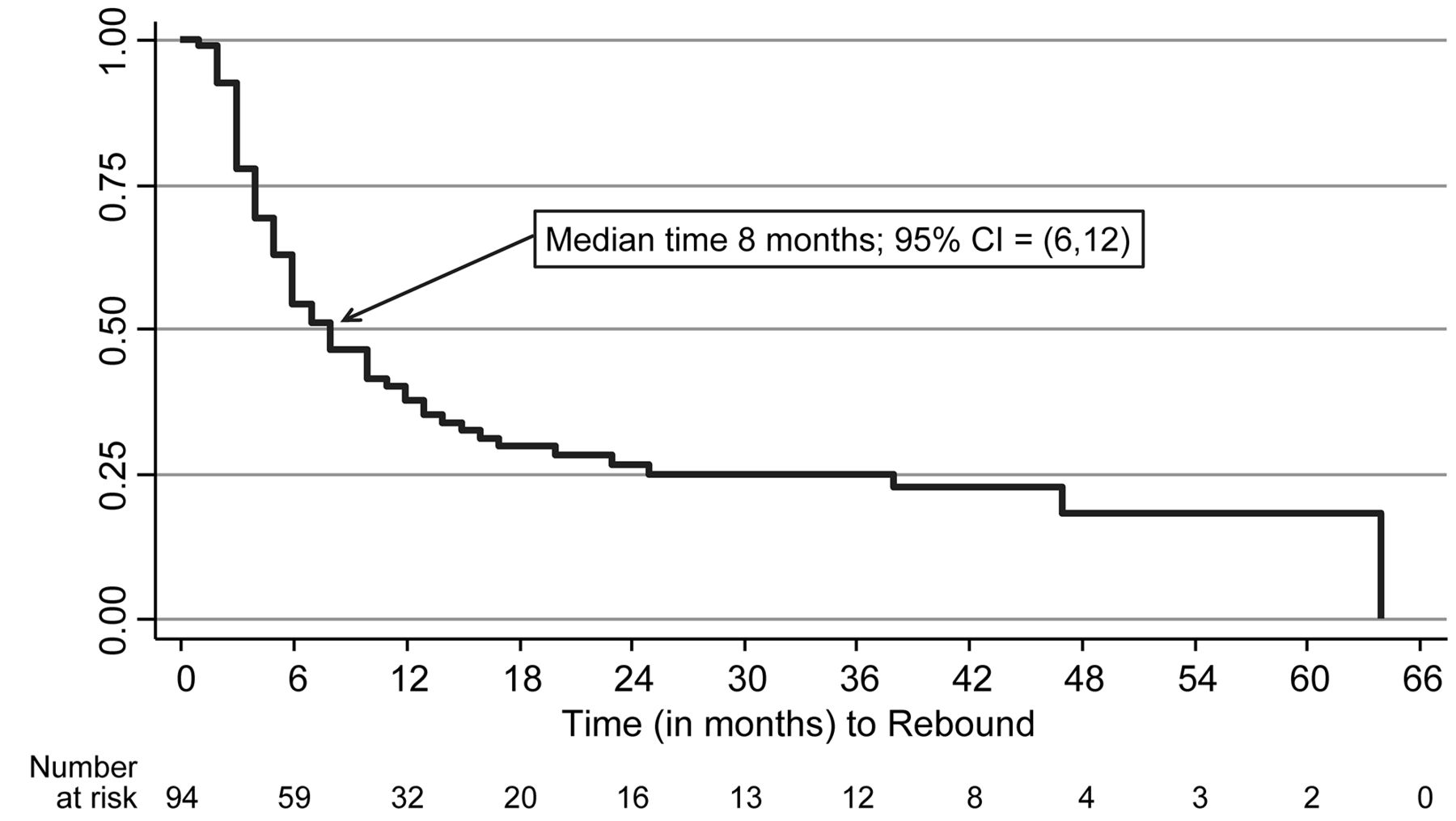
Results. Rebound occurred in 73% (69/94) of patients soon after discontinuation (median time to rebound 8.0 mos, 95% CI 6.0–12.0).
Conclusion. Rebound occurred frequently in patients with PsA after TNFi discontinuation. TNFi discontinuation after achieving LDA should be carefully considered.
- PSORIATIC ARTHRITIS
- ANTIRHEUMATIC AGENTS
- TUMOR NECROSIS FACTOR-α
Psoriatic arthritis (PsA) is a chronic, systemic, inflammatory disease affecting both the joints and skin1. Up to 40% of patients with psoriasis develop PsA; in the United States, PsA prevalence is estimated between 0.02% and 0.25% in the overall population2,3,4. Patients with PsA typically have arthritis, dactylitis, enthesitis, nail disease, and/or psoriasis, and have an increased risk for comorbid conditions, including metabolic syndrome and other conditions that contribute to cardiovascular disease risk (hypertension, hyperlipidemia, diabetes, obesity)3,5. The pain, functional and cosmetic impairments, and treatment side effects experienced by patients with PsA have been linked to increased direct costs, and decreased health-related quality of life, longterm work disability, and productivity losses6,7,8.
Symptoms and their severity may vary among patients with PsA over time2. PsA has a diverse clinical manifestation, and the primary treatment goals are to help patients reach low/minimal disease activity or remission to preserve or improve functionality, prevent irreversible structural joint damage, and to minimize the effect of comorbidities9,10. Treatment options for PsA include nonsteroidal antiinflammatory drugs as first-line therapies, and nonbiologic (nbDMARD) and biologic disease-modifying antirheumatic drugs (bDMARD), including tumor necrosis factor inhibitors (TNFi), interleukin (IL)-17 and IL-12/23, and small molecules (e.g., phosphodiesterase, Janus kinase inhibitors) as second-line therapies9. TNFi [adalimumab (ADA), etanercept (ETN), golimumab (GOL), infliximab (IFX)] are the first recommended bDMARD and these agents have long demonstrated effectiveness in reducing disease activity and controlling joint damage in patients with PsA, and more recently have been associated with lower risk of cardiovascular events in both psoriasis and PsA patients9,11. Little is known about clinical outcomes following treatment discontinuation after attaining low disease activity (LDA) or symptom remission. Therefore, our current study evaluated the rebound in disease activity (i.e., loss of initially attained LDA) and time to rebound in patients with PsA who discontinued TNFi therapy after achieving LDA.
MATERIALS AND METHODS
We analyzed retrospective data for patients with PsA who participated in the Corrona registry. Corrona is a large, US-based, independent, prospective, observational, disease-based registry with about 500 rheumatologists and 6000 patients with PsA participating since 2001. Patients are enrolled in the registry by their rheumatologists. Institutional review board (IRB) approvals for this study were obtained from local IRB of participating academic sites and from a central IRB (New England IRB, IRB#: 120160610) for private practice sites.
We included patients with a PsA diagnosis who were age 18 years or older, initiating a TNFi between October 1, 2002, and March 21, 2013, had achieved symptom remission/LDA [i.e., Clinical Disease Activity Index (CDAI) score ≤ 10], discontinued their TNFi agent while in LDA, and did not immediately switch to a different bDMARD. For patients with multiple eligible treatment courses, we used the first one. Study patients also had at least 1 followup visit after TNFi discontinuation, and physician- and patient-reported outcomes obtained at this first post-discontinuation visit were compared with those obtained at the TNFi discontinuation visit.
Rebound was defined as CDAI > 10, restart of the discontinued TNFi or initiation of another bDMARD with or without a qualifying CDAI score. We included re-initiation of the discontinued TNFi or initiation of another bDMARD as part of the definition of rebound because patients are evaluated only every 6 months for CDAI. Any drug changes that occur between 2 visits are reported at the following visit where the physician reports type of change and the date that change occurred. Thus, flares that occurred between those regular visits may have been associated with a change in medication management without a corresponding documented disease activity measure.
Other study outcomes evaluated between the TNFi discontinuation and the subsequent followup visit included patient-reported functioning on the modified Health Assessment Questionnaire (mHAQ, scores 0–3), patient’s global assessment of disease severity [visual analog scale (VAS) scores 0–100] and pain (VAS scores 0–100), as well as the physician’s global assessment of disease severity (VAS scores 0–100). For all outcomes, higher scores indicate higher levels of disease activity/severity. CDAI and bDMARD use were also determined for patients at the first post-rebound followup visit.
Patient characteristics at TNFi initiation were summarized [means (SD), ranges, percentages]. Patient- and physician-reported outcomes from the first post-discontinuation followup visit were compared with those recorded at TNFi discontinuation. Kaplan-Meier curves determined time from discontinuation to rebound with followup censored at last available visit for patients without rebound.
RESULTS
We identified 94 patients [57% women, 92% white, mean [SD] age 51.0 (12.4) yrs, 90% privately insured, 16% Medicare-insured] who discontinued TNFi (ADA: 51%, ETN: 21%, IFX: 19%, GOL: 9%) during LDA and had a post-discontinuation visit (Table 1). At TNFi initiation, the mean (SD) disease duration was 8.4 (7.0) years, mean (SD) CDAI was 10.1 (9.3), and 63.7% of patients were in LDA. The majority of patients had prior bDMARD and methotrexate (MTX) use.
Patient characteristics at TNFi Initiation.
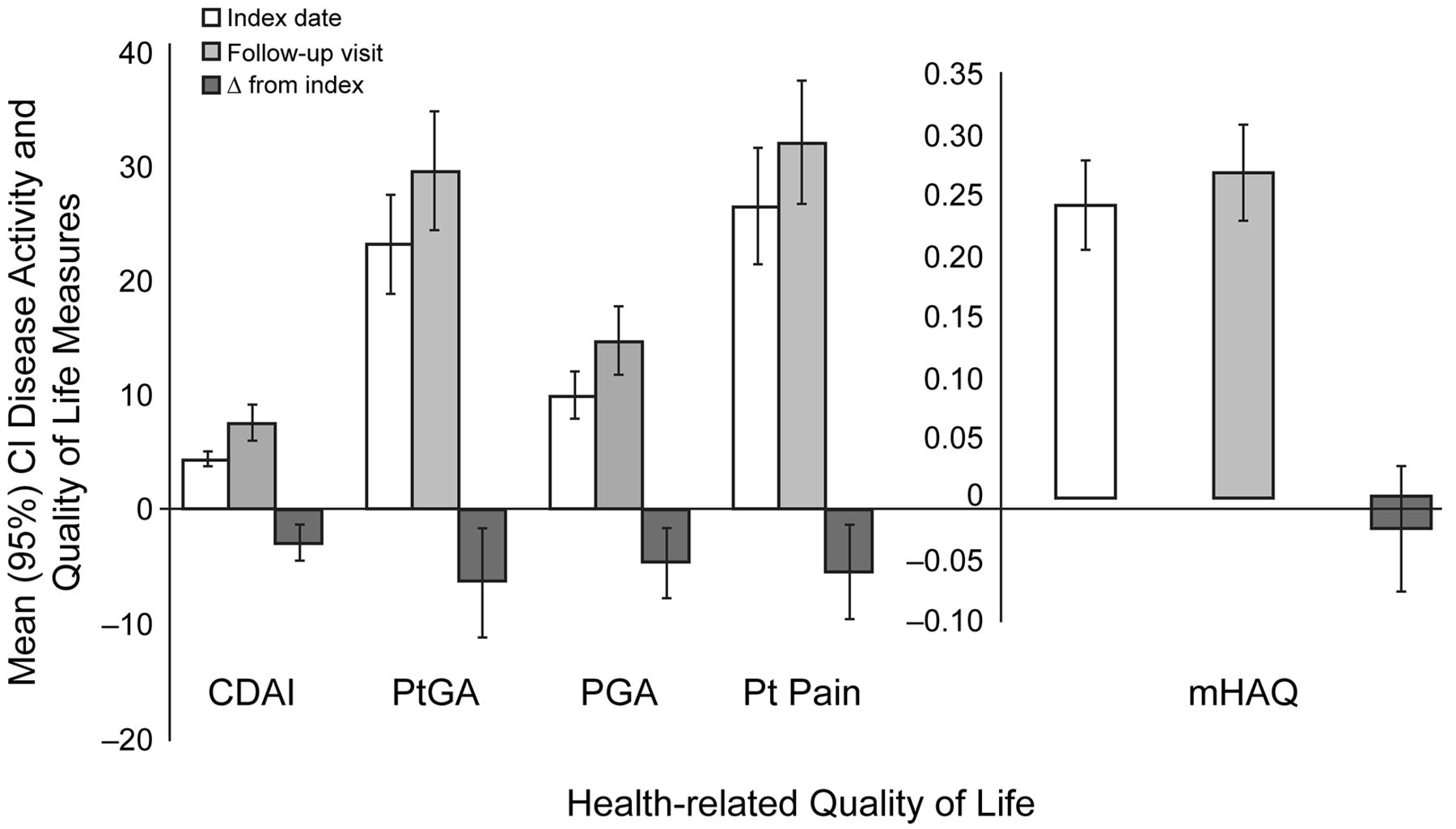
The median (interquartile range) time from TNFi discontinuation to first post-discontinuation visit was 6.8 (5.2–8.1) months. Increases in patient- and physician-reported disease activity/symptoms after discontinuation were statistically significant at p ≤ 0.01, except mHAQ (Figure 1). Most patients (n = 69, 73%) experienced a rebound event (n = 15 CDAI > 10, n = 24 with biologic initiation with nonelevated CDAI, n = 30 both elevated CDAI and biologic initiation) with a median time (95% CI) to rebound of 8.0 months (6.0–12.0; Figure 2). Among patients with a post-rebound visit (59/69), 73% were in remission/LDA at that visit. Overall, 27 of the 59 rebounders resumed use of their original TNFi by the post-rebound visit.

Change in disease activity measures from TNFi discontinuation to first post-discontinuation followup visit. Among the 59 rebounders, the CDAI at rebound was 13.5 ± 10.1 with a mean CDAI at first followup visit of 8.2 ± 8.1. TNFi: tumor necrosis factor inhibitor; CDAI: Clinical Disease Activity Index; PtGA: patient’s global assessment; PGA: physician’s global assessment; mHAQ: modified Health Assessment Questionnaire.
{kind=link}
{kind=link}
Time to rebound following TNFi discontinuation. Median time from rebound to the first followup visit was 10 months for all 59 rebounders (8.5 mos where rebound was identified by CDAI only, 9.5 mos in those identified by a drug initiation, and 10 mos in those with a drug initiation and an available CDAI). TNFi: tumor necrosis factor inhibitor; CDAI: Clinical Disease Activity Index.
DISCUSSION
The majority (73%) of the 94 patients with PsA whom we studied experienced symptom rebound after discontinuing TNFi therapy following LDA (CDAI ≤ 10) or symptom remission, with half of these patients experiencing rebound within 8 months after treatment discontinuation. Our results are also consistent with those reported in studies of TNFi dose reduction/discontinuation in patients with RA12,13,14,15, and also in a study of disease recurrence in patients with PsA who discontinued conventional or bDMARD after at least 6 months in remission (i.e., no musculoskeletal symptoms and minimal skin disease; mean Psoriasis Area Severity Index: 0.21). In that study (n = 26, 14 MTX monotherapy, 12 TNFi), 77% of patients experienced post-discontinuation recurrence, with a mean time to recurrence of 74.5 ± 72 days16. The authors concluded from this “extraordinary high” rate of recurrence that DMARD discontinuation may not be feasible even in patients who have experienced sustained remission. In a study to assess the feasibility of a treatment withdrawal trial, 11 of 17 patients with minimal PsA disease activity were randomized to treatment withdrawal, and 6 (55%) of these patients experienced a symptom flare, including 2 patients who had been receiving MTX only17. The 4 remaining patients, who had been treated with MTX and a biologic, experienced flare only after the biologic was withdrawn. None of the 6 patients randomized to continue therapy experienced flare. Interestingly, in a study of ADA dose reduction in patients with PsA, mean time to relapse was also 8 months in the minority (11%) who flared18.
The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) and the European League Against Rheumatism PsA criteria note that the evidence is too limited to recommend discontinuation, dose reduction, or tapering of bDMARD for patients with PsA who have achieved remission/LDA9,19, and the American College of Rheumatology will likely address this issue in its forthcoming 2018 PsA guideline. The significant risk of rebound that we observed offers an important perspective for physicians who are considering TNFi discontinuation for patients who have achieved remission/LDA, and may provide a key piece of data in discussing the most likely potential outcome with their patients who are considering TNFi discontinuation.
Our study provides unique real-world data on the incidence of rebound after patients with PsA who discontinued TNFi therapy after achieving remission/LDA. The study population included patients from across the United States, and represents experience in the routine care setting. As an observational cohort, patient followup was based on routine care rather than mandatory visit schedules. The registry was created prior to the development of the current validated PsA measures; instead it collected the CDAI. Thus, patients may have initiated TNFi therapy while in LDA because of nonarticular symptoms such as skin disease and enthesitis. Of note, we characterized rebounding of symptoms based on an evaluation at the time of a clinical visit. It is possible that patients may have had flare symptoms for some time before presenting to the provider, in which case we have overestimated time to flare. Additionally, mild flares not requiring use of biologics would have been missed. Also, reasons for discontinuation and initiation of medications were unavailable. Finally, while this is the largest cohort studied to date, our sample size is modest, which may limit the stability of our findings. Our results cannot be considered definitive, but they indicate that the true risk of rebound following TNFi discontinuation is likely substantial, and that continuation of bDMARD therapy may well play a key role in helping patients with PsA remain in remission/LDA.
Footnotes
Sponsored by Corrona LLC. Corrona LLC has been supported through contracted subscriptions in the last 2 years by AbbVie, Amgen, BMS, Crescendo, Eli Lilly and Company, Genentech, GSK, Horizon Pharma USA, Janssen, Momenta Pharmaceuticals, Novartis, Pfizer, Roche, and UCB. LRH is an employee and shareholder of Corrona LLC, and has a research grant to the University of Massachusetts Medical School from Pfizer. BSS, DHC, and AM are employees and shareholders of Amgen Inc. SR and WM are employees of Corrona LLC. SWW is a consultant of Amgen Inc. JDG is an employee and shareholder of Corrona LLC, and a consultant of Eli Lilly, Genentech, Janssen, Novartis, and Pfizer. CJE is an employee of Corrona LLC and an advisory board member for Merck.
- Accepted for publication July 19, 2017.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.