
Abstract
Objective. Infliximab (IFX) is a monoclonal tumor necrosis factor-α–inhibiting antibody used in children with refractory arthritis and uveitis. Immunogenicity is associated with a lack of clinical response and infusion reactions in adults; data on immunogenicity in children treated with IFX for rheumatic diseases are scarce. We aimed to describe the prevalence of anti-IFX antibodies and determine co-factors associated with anti-IFX antibodies in children with inflammatory rheumatic and ocular diseases.
Methods. Consecutive children treated between August 2009 and August 2012 with IFX at our department were included. Blood samples were collected every 6 months before IFX infusion and tested for anti-IFX antibodies by radioimmunoassay. Patients’ charts were retrospectively reviewed for clinical features and analyzed for associations with anti-IFX antibodies.
Results. Anti-IFX antibodies occurred in 14/62 children (23%) and 32/253 blood samples (12.6%) after a mean treatment time of 1084 days (range 73–3498). Infusion reactions occurred in 10/62 (16%) children during the treatment period. With continuation of IFX, anti-IFX antibodies disappeared in 7/14 children. In the bivariate analysis, the occurrence of anti-IFX antibodies was associated with younger age at IFX treatment start (mean age 7.01 vs 9.88 yrs, p = 0.003) and infusion reactions (OR 15.0), while uveitis as treatment indication was protective against development of anti-IFX antibodies (OR 0.17), likely because of higher IFX doses. In the multivariate logistic regression, all 3 covariates remained highly significant.
Conclusion. Anti-IFX antibodies occurred commonly at any time during IFX treatment. Anti-IFX antibodies were associated with younger age at IFX start, infusion reactions, and arthritis as treatment indication.
- INFLIXIMAB
- ANTICHIMERIC ANTIBODIES
- UVEITIS
- JUVENILE IDIOPATHIC ARTHRITIS
- INFUSION REACTIONS
In pediatric rheumatology, tumor necrosis factor–α (TNF-α) inhibitors are indicated when juvenile idiopathic arthritis (JIA), uveitis, and other inflammatory diseases are refractory to standard treatment [e.g., disease-modifying antirheumatic drugs (DMARD)]1,2,3,4. Although infliximab (IFX) has not officially been approved for the treatment of JIA or uveitis, it is commonly used1,2,3,5.
IFX is a TNF-α–inhibiting agent consisting of a mouse-human chimeric IgG antibody6. Acute infusion reactions are the most frequent therapy-limiting adverse event, with an incidence of 6%–23% in adults with rheumatoid arthritis (RA) depending on the study period7,8,9. In children with JIA, the incidence ranges between 9%–35%10,11,12,13. Acute infusion reactions are defined as any adverse event occurring during the infusion or within 1 h of its termination12. Anti-IFX antibodies, also referred to as human antichimeric antibodies or antidrug antibodies, occur in 8%–43% of patients with RA depending on the IFX dose, the co-medication, and the method used for antibody detection14,15. They often appear during the first year of treatment15,16. In our initial study, 14/82 children treated with IFX experienced an infusion reaction17. However, serum anti-IFX antibodies were not determined.
The occurrence of anti-IFX antibodies is a major issue because their presence has been shown to increase the risk of infusion reactions and has been linked with subtherapeutic serum drug levels and lack of clinical response in patients with RA6,15,18,19. Bendtzen showed that in patients with RA treated with IFX the development of antibodies was preceded by low serum IFX levels and was associated with an increased risk of infusion reactions and subsequent treatment failure18. Imaging studies by van der Laken suggested the formation of IFX–anti-IFX complexes and their faster clearance from the body in patients with RA not responding to the treatment19. Further, a high level of anti-IFX antibodies and formation of large antibody complexes were associated with a more severe infusion reaction19. The balance between IFX and the antibody response regulates the effectiveness of the drug and its side effects20. As long as antibody production does not exceed the IFX serum trough level, the drug can provide clinical benefits20. When the level of antibodies is higher than the drug level, IFX is cleared from the circulation, and free antibodies can be measured in the blood. This ultimately leads to loss of drug efficacy. Immunogenicity can be influenced by treatment factors such as the IFX dose and use of concomitant immunomodulators as evidenced in different studies of adults with RA and inflammatory bowel disease (IBD)21,22.
Studies of the immunogenicity of IFX have been conducted mainly in adults with RA and IBD8,15,18,20,22. Data on immunogenicity of IFX in children with inflammatory rheumatic and ocular diseases are scarce10,12,13. Therefore, the first purpose of our study was to determine the prevalence of anti-IFX antibodies in children treated with IFX for inflammatory rheumatic and ocular diseases during a treatment observation period. The second aim was to search for and characterize various co-factors that are associated with the occurrence of IFX antibodies and may have implications for immunogenicity and management of the disease.
MATERIALS AND METHODS
Patients
All consecutive patients previously diagnosed with JIA or inflammatory ocular disease, followed and treated with IFX at the Rheumatology Department of the University Children’s Hospital Zurich, Switzerland, between August 2009 and August 2012, were included into the study. Inclusion criteria were a diagnosis of JIA, JIA-associated uveitis, or idiopathic noninfectious uveitis, and a disease course refractory to standard treatment such as disease-modifying antirheumatic drugs [mostly methotrexate (MTX) or leflunomide (LEF)] or corticosteroids, which led to treatment with biologic agents. All children included in our study received IFX. IFX was preferred over other TNF-α inhibitors for various reasons17. Until 2014, etanercept (ETN) was the only TNF-α inhibitor officially registered for pediatric use in Switzerland. There was no legal difference in the use of any other TNF-α inhibitor [e.g., IFX or adalimumab (ADA)] and the choice of TNF-α inhibitor was at the discretion of the treating physician. Because IFX was available years before ETN and ADA, it was used more frequently in the earlier era of anti–TNF-α therapy. The majority of the patients were receiving maintenance treatment with IFX, but patients starting IFX during the study period were also included. Patients who discontinued IFX before August 2009 were not included. The patient’s observation time ended with either the discontinuation of IFX or the end of the study period (April 2013). The treatment period was independent from the study observation period. The treatment period and observation period did not necessarily overlap and were independent from other important variables assessed in the study. JIA was diagnosed based on the International League of Associations for Rheumatology classification criteria23,24. Contraindications for IFX treatment included acute or recurrent infections, heart failure, and a history of lymphoma in a first-degree relative. All patients were screened for tuberculosis by history and skin testing prior to treatment start.
Intervention
IFX was administered at the Outpatient Day Clinic according to the manufacturers’ instructions with an initial dose of usually 5–7 mg/kg. To reduce the risk of antidrug antibody formation, all patients were taking concomitant immunosuppressive medication, usually MTX19,21,22. During an infusion reaction, the patients were assessed by a pediatric rheumatologist and the symptoms were classified as mild, moderate, or severe. A detailed description of the IFX administration protocol, infusion reactions, and their management has been published by our group17.
Data sampling
Patient’s charts were retrospectively reviewed for demographic data, and disease and treatment characteristics (such as treatment indication, age at IFX start, IFX dose, infusion interval, type and dose of co-medication, number of active joints, and infusion reaction). A flare was defined as recurrence of arthritis or uveitis (in turn defined by recurrence or increase of inflammatory cells) in a patient with inactive disease. The outcome measure was the occurrence of detectable anti-IFX antibodies during the study period.
Anti-IFX antibody detection
Blood was sampled biannually between August 2009 and April 2013 in all patients before IFX infusion and stored at −20°C. Anti-IFX antibody testing was performed at the Sanquin Laboratory for Biologicals in the Netherlands using a radioimmunoassay (RIA) developed in-house (www.sanquin.nl). One microliter of serum diluted in freeze buffer was incubated with 1 mg protein A sepharose in 800 μl of total volume. The samples were incubated overnight and washed, thereafter 125I radioactive-labeled IFX F (ab’)2 fragments were added. Again the samples were incubated overnight, unbound radiolabel was washed out, and sepharose-bound radioactivity measured. The results are expressed as arbitrary units (AE)/ml with 1 AE/ml equaling about 10 mcg/l. The lower limit of quantification is 12 AE/ml25. RIA is less sensitive to drug interference than other antibody detection techniques and is therefore able to detect low anti-IFX antibody concentrations in the presence of the drug25. RIA was chosen because it was commercially available and has been shown to correlate with clinical outcome6.
Analysis
Descriptive data including the prevalence of anti-IFX antibodies and the titer distribution were determined. Occurrence of anti-IFX antibodies at any time during the observation period defined the patient as anti-IFX antibody– positive. Distributions of continuous variables were compared by the Wilcoxon U-test for independent samples26. Between the groups with and without anti-IFX antibodies, categorical co-factors were compared by bivariate OR providing proportions or the relative frequencies (odds) including the 95% CI27. Associations were further examined by multivariate stepwise logistic regression, with occurrence of IFX antibodies as dependent variable and all covariates of the bivariate analysis to obtain adjusted multivariate OR. We hypothesized that the following covariates were putatively associated with the occurrence of anti-IFX antibodies: age at IFX start, sex, treatment indication, IFX dose at treatment start, MTX dose (mean dose per patient over the observation period), systemic corticosteroids, and infusion reaction. SPSS 22.0 for windows (SPSS Inc.) and Excel 14.5.0 for Mac were used for the statistical analysis. The study was approved by the institutional ethics review board of the University Children’s Hospital, Zurich.
RESULTS
Patients
During the 3 years of inclusion (August 2009–August 2012), medical records of all children treated with IFX were collected. The observation period ended in April 2013 because anti-IFX antibody level determination had become commercially available.
A summary of the patient’s characteristics is shown in Table 1. Seventeen patients were treated by other biologic agents before IFX treatment start. One patient with JIA had previously discontinued IFX in 2004 following disease remission. The arthritis flared a few months later and ETN was started. ETN was discontinued in 2012 owing to treatment failure and the patient restarted IFX. The IFX dose at treatment start did not differ between treatment indications [mean (SD) IFX dose: 6.00 (1.50) mg/kg for arthritis, 6.33 (1.27) mg/kg for uveitis, and 5.78 (1.70) for arthritis and uveitis; p = 0.598].
Characteristics of children with and without anti-IFX antibodies. Data are n (%) or means with SD.
Prevalence of IFX antibodies
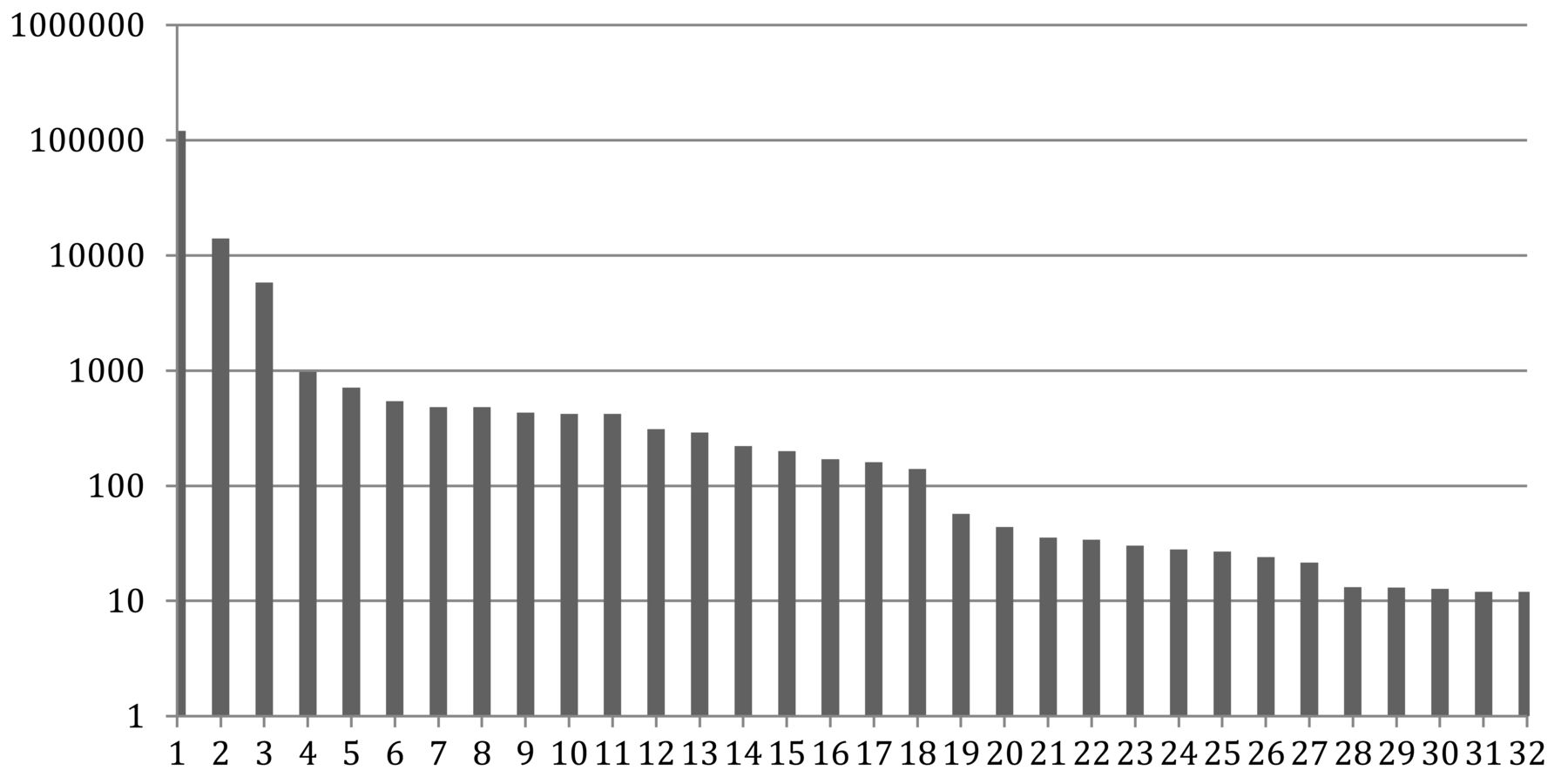
Detectable anti-IFX antibodies occurred in 14/62 patients (23%, 95% CI: 12–34). Out of a total of 253 blood samples (1–6 per patient), 32 were positive (12.6%, 95% CI: 8.5%–16.7%). Anti-IFX antibodies occurred after a mean treatment time of 1084 days (range 73–3498). The distribution of the anti-IFX antibody titers is shown in Figure 1. The median anti-IFX antibody titers were higher in patients with infusion reactions (355 AU/ml, range 13–120,000) compared to patients without infusion reactions (88 AU/ml, range 12–430), but the difference was statistically not significant (p = 0.234).

{kind=link}
Anti-IFX antibody titers detected in 32 blood samples. The X axis depicts the 32 blood samples with anti-IFX antibodies. The Y axis gives the antibody titer in arbitrary units/ml. IFX: infliximab.
Infusion reactions occurred in 10/62 patients (16%) during the treatment period, in 7 during, and in 3 before the observation period. In 7/14 patients (50%), the occurrence of anti-IFX antibodies was associated with a disease flare. Simultaneously, 3 of them had an infusion reaction. Because disease flares were retrospectively determined but not defined according to the American College of Rheumatology Pediatric Criteria core set measures28, we did not further include this variable in the analyses. All patients received a co-medication: MTX (n = 53), or LEF (n = 7), or azathioprine (AZA; n = 2). Most patients were taking low-dose MTX [mean 6.2 (SD 1.8) mg/m2/week]; LEF was prescribed based on weight between 10 mg every other day and 20 mg per day; AZA was prescribed between 1.5 and 2.5 mg/kg/day. Neither the type of co-medication (Table 1), nor the MTX dose (Table 2) were associated with the occurrence of anti-IFX antibodies. None of the patients with anti-IFX antibodies had received systemic corticosteroids. An OR and the 95% CI could not be determined (division by 0). With continuation of IFX treatment, anti-IFX antibodies disappeared in half of the patients (7/14). In 5 out of the 7 patients in whom anti-IFX antibodies were present and eventually disappeared, the IFX dose had been escalated: 2 patients underwent both dose increase and interval shortening, 2 a dose increase, and 1 an interval shortening. Two out of 7 children in whom anti-IFX antibodies were temporarily present had infusion reactions during the study period. In both children, anti-IFX antibodies were detectable in the blood sample drawn within the closest temporary relationship to the infusion reaction.
Bivariate and multivariate analysis (stepwise logistic regression) in the 62 children.
Co-factors associated to IFX antibodies
Table 1 reveals that children with anti-IFX antibodies were significantly younger at IFX treatment start (mean age 7.01 yrs vs 9.88, p = 0.003). Table 2 (bivariate analysis) shows that patients with anti-IFX antibodies had a 15-fold increased risk to experience an infusion reaction compared to those without anti-IFX antibodies, as shown by the statistically significant OR. In contrast, the relative frequency of occurrence of anti-IFX antibodies was significantly lower (OR 0.17) for patients who were treated for uveitis, compared to those having arthritis as a treatment indication. This corresponds to an 83% risk reduction to develop anti-IFX antibodies for those treated because of their uveitis. Significant OR was not shown in sex, IFX treatment start dose, MTX dose, or systemic corticosteroids.
Multivariate logistic regression confirmed the statistically significant associations of these 3 covariates: age at IFX treatment start, occurrence of infusion reaction, and uveitis as treatment indication. This was the case even if adjusted for the other covariates (sex, IFX start dose, MTX dose, systemic corticosteroids, and uveitis in the model; Table 2).
DISCUSSION
In this pilot study, we retrospectively examined the prevalence and associations of anti-IFX antibodies in children treated with IFX for JIA and/or uveitis. Although generalizability of our study results is limited by the small number of patients and the short study period, some of the results demonstrated impressive levels that can help to direct future studies. The prevalence of detectable anti-IFX antibodies was 23% in this cohort. The occurrence of anti-IFX antibodies was significantly associated with younger age at IFX treatment start (+23% risk increase per yr), and very highly with infusion reactions (OR 15.00). In contrast, children with uveitis as treatment indication developed anti-IFX antibodies less frequently, likely because of higher IFX doses. Despite the small patient number, the results were statistically significant in the bivariate analysis and remained consistently significant in the multivariate analysis.
Several factors limited our analyses: Occurrence of anti-IFX antibodies may be caused and influenced by different mechanisms, of which many are unknown. The exact dose-response relationship between IFX level and anti-IFX antibody level remains to be determined6. Besides treatment-related factors such as IFX doses and co-medication, patient-related factors such as disease activity, drug-related factors such as size of immune-complex formation (IFX–anti-IFX antibody complex) and differences in the pharmacokinetics of individual patients have been shown to influence immunogenicity15,18,19,29. In addition, the clinical effect of immunogenicity is difficult to predict on the basis of anti-IFX antibody measurement alone6. To statistically reflect a large spectrum of anti-IFX antibody levels, a huge sample size (much larger than ours) would be necessary. Moreover, quantification of anti-IFX antibody levels by RIA has several limitations, especially that predominantly free anti-IFX antibodies are detected by this method, but not those bound to serum IFX (IFX–anti-IFX antibody complex)6.
The prevalence of antibodies to IFX in 23% of the children in our study was slightly lower compared to other pediatric rheumatologic studies, in which anti-IFX antibodies were detected in 37%–43% of patients10,12,13. However, compared to those studies, our study had a different design, i.e., patient inclusion at IFX treatment start and during treatment with variable followup. Moreover, other methods such as ELISA have been used to detect antidrug antibodies. The question of which is the optimal method to measure antibodies is not yet answered in the literature25,30. In our study, anti-IFX antibodies were measured by RIA. RIA has been shown to exceed ELISA measurements in different aspects (e.g., fewer false-positive results), possibly explaining the differences in prevalence of detectable anti-IFX antibodies30. Further, antidrug antibodies measured by the RIA method used in our study have been shown to correlate with loss of efficacy6. The use of a drug-tolerant assay may result in the detection of antidrug antibodies that do not have a clinical effect, and may therefore not necessarily constitute a better option31.
Interestingly, and consistent with previous studies, patients who developed anti-IFX antibodies were significantly younger at IFX start. Studies on immunogenicity of factor VIII treatment in hemophilia patients have shown that older age at treatment start was associated with lower rates of antidrug antibodies32,33. This age-dependent effect of antidrug antibody development has previously been described in patients treated with IFX34. Steenholdt, et al investigated the immunogenicity of IFX in adults treated for IBD and demonstrated that patients with infusion reactions were significantly younger at time of diagnosis (19 vs 26 yrs) and at first IFX infusion (28 vs 35 yrs). Further, infusion reactions were strongly associated with anti-IFX antibody occurrence34. A Finnish study analyzed 65 children taking IFX (49 patients with rheumatologic diseases and 16 with IBD) and observed more infusion reactions in younger children, but anti-IFX antibodies were not determined11. However, another large study comparing immunogenicity of IFX treatment in children and adults with IBD did not confirm these results: while antibodies to IFX were detected in 11% of adults, they occurred in only 2.7% of children35. The current available literature suggests a possible influence of the developing immune system on immunogenicity of IFX, and further studies are needed for clarification. In addition, higher disease activity in younger patients could explain the higher prevalence of anti-IFX antibodies, because higher disease activity has been associated with immunogenicity to IFX18.
We observed a 15-fold higher incidence of infusion reactions in children with detectable anti-IFX antibodies. These results are in line with previous studies in adults with RA15,18. In our cohort, only 6% of the children without anti-IFX antibodies had a history of infusion reaction, and the interval between infusion reaction and first blood sample collected for detection of anti-IFX antibodies was more than 2 years. We hypothesize that antibodies to IFX were present at the time of the infusion reaction but disappeared subsequently. In fact, antibodies disappeared in half of our patients during the study period upon continuation and eventual IFX dose escalation. This has been described by other groups15,36. However, in contrast to studies in adults with RA, where anti-IFX antibodies occurred mainly during the first year of treatment15,16, antibodies occurred at a later time in our patients. Our observations suggest that development of immunogenicity is gradual and can change over time. Once treatment is continued, the patient’s immune system may induce tolerance or stimulate further antibody production.
The association of uveitis with lower frequency of detectable anti-IFX antibodies may be confounded by the IFX dose. Though the IFX starting dose was not significantly higher for children with uveitis compared to children with arthritis, children with uveitis may have received higher IFX doses over the observation period. The IFX dose at treatment start was not associated with anti-IFX antibody occurrence. However, the IFX start dose may not be a sufficient surrogate variable to assess the risk to develop anti-IFX antibodies. The total IFX dose during treatment, peaks of IFX doses, individual variability of immune response to IFX, interactions with co-medications and other individual disease- and response-modifying factors may also contribute to that risk. The study design and high variability of individual IFX treatment regimens in our patients preclude a more sophisticated analysis. However, high IFX doses have been associated with low anti-IFX antibody levels12,13,15,37. An IFX dose increase might be considered in children with detectable anti-IFX antibodies to reduce immunogenicity and risk of infusion reactions. This needs to be examined in future controlled prospective studies.
Children treated with systemic corticosteroids at any time during IFX treatment did not develop anti-IFX antibodies. Premedication with corticosteroids is widely used in patients with IBD treated with IFX, and premedication as well as concomitant treatment with corticosteroids have been associated with fewer infusion reactions in patients with IBD and RA38,39,40. A pre-medication or short-term therapy with systemic corticosteroids might be considered to reduce the risk of anti-IFX antibody development.
There are several limitations to our study. The sample size was small, leading to large 95% CI. Data collection was retrospective even if the blood was sampled prospectively. Assessment of disease severity was not routinely performed and disease activity scores were not routinely used in the therapeutic management at our institution. Serum IFX levels were not measured; however, detection of anti-IFX antibodies has been shown to depend on the relative level of produced anti-IFX antibodies and the level of administered IFX20. Further, presence of detectable anti-IFX antibodies was determined every 6 months, and the time of blood sampling did not always coincide with the occurrence of clinical factors such as infusion reactions18,19. Dose-response relationship between IFX levels and anti-IFX antibodies could not be determined for the above-mentioned reasons. However, our results are comparable to observations in adults in which an association of anti-IFX antibody development and loss of efficacy and infusion reactions have been described20. The study duration was limited by the available resources and the majority of patients were included while receiving maintenance treatment with IFX. Therefore, temporary and early immunogenicity may not have been recognized. More frequent anti-IFX antibody measurement from IFX treatment start would strengthen our observations. Finally, various biologic agents are now available to treat uveitis and JIA-associated uveitis. Other therapeutic agents may be preferred over IFX41. Some studies have shown beneficial effects of ADA and a possibly better efficacy in the treatment of uveitis and JIA-associated uveitis compared to IFX, but direct comparison was rarely done and the results are still being debated42,43,44.
We showed that anti-IFX antibodies may occur frequently and at any time during IFX treatment in children with JIA and/or uveitis. The risk to develop anti-IFX antibodies is increased in children with younger age at IFX treatment start and in children with arthritis as treatment indication, which is likely associated with a lower IFX dose. The occurrence of anti-IFX antibodies is highly associated with infusion reactions. However, antibodies to IFX may disappear with ongoing treatment and therefore do not necessarily constitute an indication for a medication change.
Acknowledgment
The authors thank Monika Straub for valuable and active support with the blood sampling.
Footnotes
Laboratory testing was funded by miscellaneous donations collected in the research fund of the rheumatology department, University Children’s Hospital, Zurich. T. Rispens received a research grant from Genmab.
- Accepted for publication November 24, 2016.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.