
Abstract
Objective. Several aspects of rituximab (RTX) retreatment in rheumatoid arthritis (RA) need to be further elucidated. The aim of this study was to describe the effect of repeated courses of RTX on disease activity and to compare 2 retreatment strategies, fixed-interval versus on-flare retreatment, in a large international, observational, collaborative study.
Methods. In the first analysis, patients with RA who received at least 4 cycles with RTX were included. In the second analysis, patients who received at least 1 RTX retreatment and for whom information about the strategy for retreatment was available were identified. Two retreatment strategies (fixed-interval vs on-flare) were compared by fitting-adjusted, mixed-effects models of 28-joint Disease Activity Score (DAS28) over time for first and second retreatment.
Results. A total of 1530 patients met the eligibility criteria for the first analysis. Significant reductions of mean DAS28 between the starts of subsequent treatment cycles were observed (at start of first treatment cycle: 5.5; second: 4.3; third: 3.8; and fourth: 3.5), suggesting improved response after each additional cycle (p < 0.0001 for all pairwise comparisons). A total of 800 patients qualified for the second analysis: 616 were retreated on flare and 184 at fixed interval. For the first retreatment, the fixed-interval retreatment group yielded significantly better results than the on-flare group (estimated marginal mean DAS28 = 3.8, 95% CI 3.6–4.1 vs 4.6, 95% CI 4.5–4.7, p < 0.0001). Similar results were found for the second retreatment.
Conclusion. Repeated treatment with RTX leads to further clinical improvement after the first course of RTX. A fixed-interval retreatment strategy seems to be more effective than on-flare retreatment.
- RHEUMATOID ARTHRITIS
- RITUXIMAB
- RETREATMENT
Rituximab (RTX) is an anti-CD20 chimeric monoclonal antibody approved for the treatment of active rheumatoid arthritis (RA). Its efficacy and acceptable safety profile have been demonstrated in large randomized controlled trials1,2,3,4. A course of RTX usually consists of 2 infusions of 1000 mg each, administered with a 2-week interval. It is common clinical practice to re-treat patients who respond to the first cycle of RTX, but there is still no clear consensus about retreatment strategy.
Initially, it was shown that clinical response did not correlate with B cell depletion because B cells were depleted in all patients after RTX treatment, but only a proportion of patients responded to therapy5. This would suggest that patients who did not respond to therapy with RTX might have a more B cell-independent disease. However, more studies have shown a correlation between the depth of B cell depletion, both in the circulation and in the synovium, and clinical response6,7. Persistence of B cells is associated with poorer prognosis8, which would suggest that retreatment with RTX even in those patients who do not exhibit a response after the first cycle could yield improved results. While a study by Thurlings, et al6 showed that patients who did not exhibit clinical improvement after the first course of RTX also failed to improve after retreatment with RTX, later studies showed enhanced clinical response after retreatment even in nonresponders9.
Regarding time to retreatment, there are 2 main strategies: to re-treat on flare and to re-treat on a fixed interval before the patient flares. Some data have suggested that the latter strategy would be preferable10. More data are needed to further elucidate several aspects of retreatment with RTX in a clinical setting.
The aims of this study were (1) to evaluate the effect of repeated courses of RTX on disease activity, and (2) to compare on-flare and fixed-interval retreatment with RTX in a large real-life cohort of patients with RA.
MATERIALS AND METHODS
Patient population and selection
The European Collaborative Registries for the Evaluation of RTX in Rheumatoid Arthritis (CERERRA) is an investigator-led, industry-supported initiative with the aim of evaluating the clinical aspects of RTX use in patients with RA11,12. It is a prospective cohort study. The following participating European registries submitted fully anonymized datasets of patients with a diagnosis of RA who had started treatment with RTX: Czech Republic, Denmark, Finland, Norway, Portugal, Romania, Russia, Slovenia, Sweden, and Switzerland. Data were pooled and analyzed. Ethical approval for the use of data from each registry was obtained by the local authorities of each country. The Regional Ethical Review Board in Stockholm approved the collection and analysis of anonymized data from the participating registries (ethics approval number: 2010/822-31/3). Informed consent was obtained from each patient before inclusion in each registry according to local regulations.
The following information was collected at baseline (time of first RTX treatment cycle): demographic data (age, sex), RA disease duration in years (from the time of diagnosis), rheumatoid factor (RF; positive/negative), anticyclic citrullinated peptide antibodies (anti-CCP; positive/negative), number of prior conventional synthetic disease-modifying antirheumatic drugs (csDMARD), number of prior biologic DMARD (bDMARD), Disease Activity Score at 28 joints (DAS28) and its components (swollen joint count, tender joint count, visual analog scale general health, and erythrocyte sedimentation rate, except for Danish patients in whom C-reactive protein was used), functional status based on the Health Assessment Questionnaire (HAQ), and concomitant corticosteroid and csDMARD use. DAS28 and HAQ, as well as information on concomitant corticosteroid and csDMARD use, were reported in every followup visit. Information about the retreatment was also collected, such as the number of retreatments, date, and retreatment strategy. The retreatment strategy, as reported by the treating rheumatologist, was either retreatment on flare (deterioration of the disease) or fixed-interval retreatment. Information about retreatment strategy was available in only some of the collaborating registries.
From the cohort of patients, we excluded those who had no followup visit (n = 619). These were mostly patients who were lost to followup or patients who started treatment with RTX close to the time of the data pooling and therefore had not yet had a followup visit. Patients who received RTX retreatment more than 1 month before or 3 months after baseline visit for the particular treatment cycle were excluded. This discrepancy between actual date of retreatment and baseline visit date for each retreatment was observed for a minority of patients (around 10% for the second, third, and fourth treatment cycle).
For the first analysis, we identified and selected patients who received at least 4 treatment cycles with RTX. A potential observed improvement in disease activity with repeated RTX cycles in the whole cohort of patients could appear because it was mainly responders who continued treatment. By selecting only patients who had received at least 3 retreatments (4 cycles), we were able to examine whether those patients who continued with RTX could further improve their disease activity with repeated retreatments. Four subgroups were formed: first, second, third, and fourth treatment cycle. We defined baseline visit as the first visit within each cycle.
In the second analysis, patients who received at least 1 retreatment (2 courses) with RTX and for whom information about retreatment strategy was available were identified.
Statistical analysis
The different subgroups of patients were characterized by means of descriptive statistics. The normality of variables was tested by skewness. Normally distributed continuous variables were presented as mean ± SD while those with non-normal distribution were presented as median [interquartile range (IQR)]. The Student t test and Mann-Whitney U test were used to compare continuous variables, while the chi-square test was used for nominal variables. The level of statistical significance was set at 5%.
Disease activity was assessed by DAS28 and disease activity state (proportion of patients with low disease activity or in remission) at the start of each treatment cycle. Functional status based on HAQ was also assessed. Additionally, improvements in disease activity from the start of RTX treatment (baseline of first treatment cycle) to the start of subsequent treatment cycles (baseline) was evaluated in terms of DAS28 (δDAS28), proportion of patients with δDAS28 of > 1.2, and European League Against Rheumatism (EULAR) response.
The mean ± SD DAS28, mean ± SD δDAS28, mean ± SD HAQ, and EULAR response were compared between the treatment cycles by ANOVA. Bonferroni was used as a posthoc test. EULAR response rates at the start (baseline = visit 1) of each treatment cycle were calculated with δDAS28 (improvement from the start of first RTX cycle) as a measure of treatment response.
The number of measurements (followup visits) was not the same for all patients and visits were not performed at fixed intervals, as expected in a real-life setting. For these reasons, mixed-model analysis for longitudinal data was used because it can handle uneven spacing of repeated measurements and even missing data (as long as missing data are missing at random). Two mixed-effects models, 1 with DAS28 and a second with δDAS28 as dependent variables and treatment cycle as fixed effect, were performed to assess the effect of each treatment cycle on disease activity. Time was also fitted in the models as time, time2, and time3. Interactions treatment cycle and time (cycle*time), treatment cycle*time2, and treatment cycle*time3 were also included in the model. Country and individual patient were included in the model as random variables. Different association models for the covariance structure between the repeated measures of the primary outcomes were performed and compared using the Akaike information criterion.
In the second analysis, the 2 retreatment strategies were compared by fitting an adjusted mixed-effects model of the longitudinal DAS28 for patients with complete covariate information. The 2 retreatment strategies were compared separately for first and second retreatment. For the first retreatment, the model was adjusted for concomitant corticosteroids and concomitant csDMARD. The first 12 months from the start of each retreatment were taken into consideration. Time as well as interactions between time and treatment strategy were fitted in the model (as in the first analysis). The 2 different retreatment strategies were compared by applying an adjusted–mixed model analysis with DAS28 as the dependent variable as well as by estimated marginal means.
As mentioned, there were some patients for whom there was a discrepancy between actual date of retreatment and baseline visit date for each retreatment and who were excluded from the main analysis. Sensitivity analysis including these patients yielded similar results (data not shown).
RESULTS
A total of 5459 patients with RA in the cohort started treatment with RTX. Of these, 4840 patients had at least 1 followup visit, and 1530 patients had received at least 4 cycles of RTX. The numbers of patients from each participating register were 136 from the Czech Republic, 144 from Denmark, 37 from Finland, 6 from Norway, 58 from Portugal, 769 from Romania, 80 from Russia, 60 from Slovenia, 160 from Sweden, and 80 from Switzerland. Of these 1530 patients, 84.1% were women, 72.4% were RF–positive, and 78.0% were anti–CCP-positive. The mean ± SD age was 57.1 ± 11.8 years and median disease duration was 11 (IQR 6–18) years. Patients had not responded to a mean of 2.9 ± 1.6 prior csDMARD and a median of 1 (IQR 1–2) prior bDMARD. Mean baseline (i.e., at the time of the first RTX cycle) DAS28 and HAQ were 5.5 ± 1.5 and 1.5 ± 0.7, respectively. The majority (80.3%) of all patients received concomitant csDMARD treatment, while 66.8% received concomitant oral corticosteroids. Significant heterogeneity across countries was observed for several baseline characteristics, as was expected (data not shown) and as we have seen in a previous analysis11.
Effect of repeated retreatment on disease activity and functional status
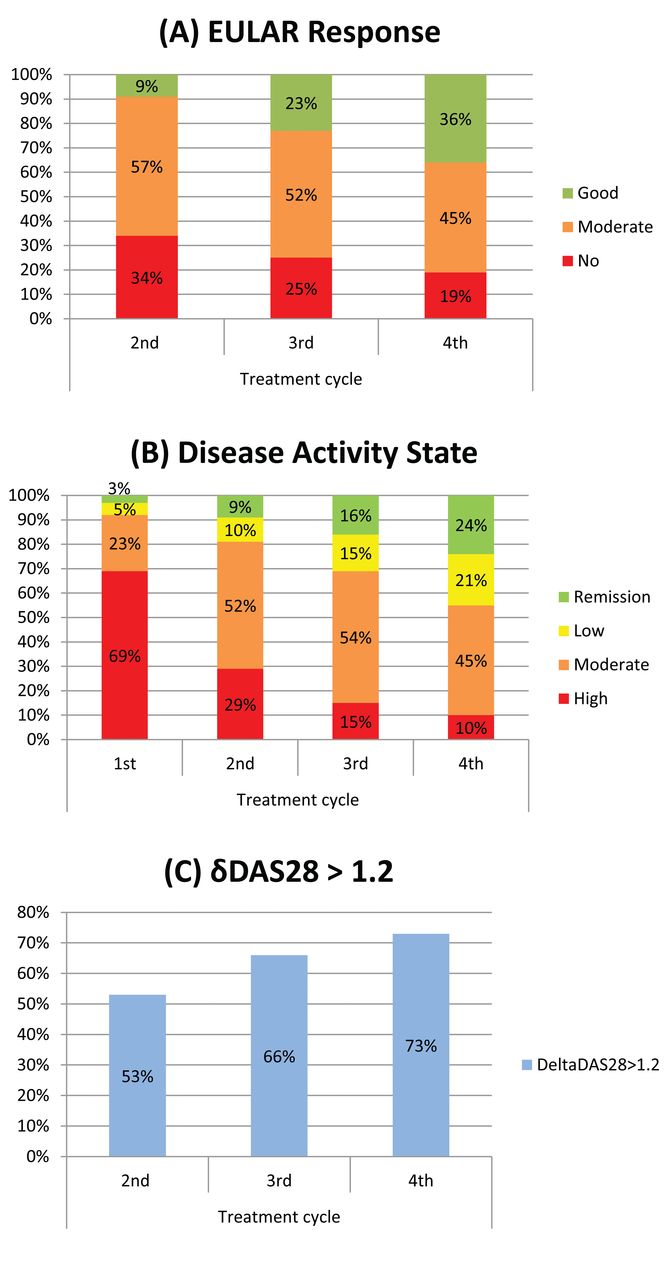
In the 1530 patients, the total number of visits during the first 12 months from the beginning of the first, second, third, and fourth cycle was 4815, 3874, 3814, and 3389, respectively. The median (IQR) time from the time of the first RTX cycle was 0 (0–0), 8 (6.5–9.5), 14.7 (13.2–17.8), and 21.6 (19.7–26) months, respectively. The mean ± SD DAS28, HAQ, and δDAS28 at the beginning of each cycle (visit 1 at each treatment) are summarized in Table 1. Significant improvement of DAS28 and δDAS28 was observed at the start of each treatment cycle, suggesting an overall further improvement of disease activity with repeated retreatment. On the contrary, HAQ improved significantly from first to second treatment start, but remained stable thereafter. Figure 1 shows the percentage of patients in different (A) EULAR responses, (B) disease activity states, and a (C) δDAS28 > 1.2 at baseline (start) of each treatment cycle.

(A) EULAR response rates at start (baseline = visit 1) of each treatment cycle for 1530 patients who received at least 4 RTX treatment cycles. A significant reduction in the proportion of nonresponders was observed parallel to an increase in the proportion of EULAR good and moderate responders. (B) Disease activity state based on DAS28 at baseline of each treatment cycle for 1530 patients who received at least 4 RTX treatment cycles. A significant reduction of the proportion of patients in high disease activity is observed parallel to an increase of the proportion of patients in low disease activity and remission. (C) Proportion of patients at baseline of second, third, and fourth treatment cycle who have a δDAS28 > 1.2 compared with baseline of first treatment cycle. EULAR: European League Against Rheumatism; RTX: rituximab; DAS28: Disease Activity Score at 28 joints.
Clinical and functional status at the beginning (visit 1) of each treatment cycle as assessed by DAS28, HAQ, and δDAS28. δDAS28 was defined as the reduction of DAS28 since the start of the first treatment cycle. Values are mean ± SD unless otherwise specified.
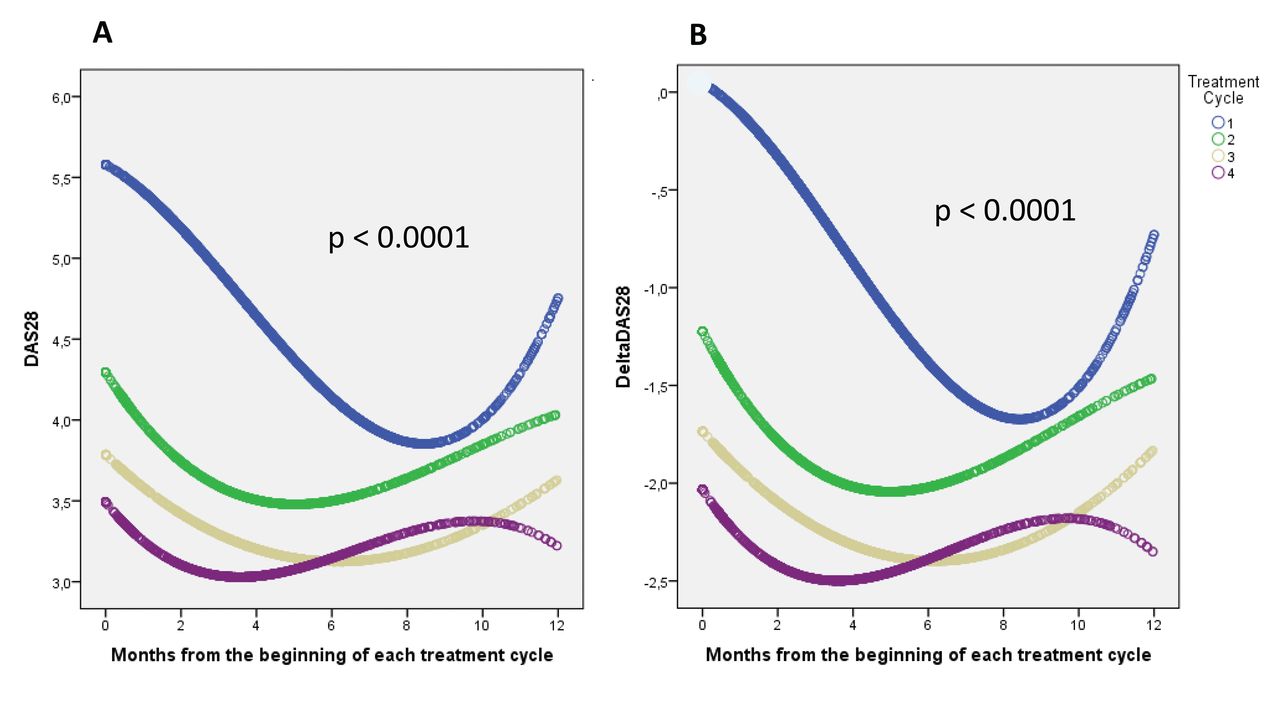
In the mixed-model analyses with DAS28 and δDAS28 as the dependent variables (in separate models), with time and treatment cycle as fixed factors and with country and individual patient as random factors, each treatment course was associated with significant improvements in δDAS28 (p < 0.0001). Comparison between curves revealed significant difference between all cycles. In Figure 2A and Figure 2B, the predicted DAS28 and δDAS28 during the first 12 months from the beginning of each treatment cycle (first, second, third, and fourth RTX cycle) is shown.

Progression of (A) DAS28 and (B) δDAS28 during the first 12 months of the first, second, third, and fourth treatment cycle for patients who received at least 4 RTX treatment cycles. The values are predicted values from the mixed-model analyses. Treatment cycle affected the model significantly (p < 0.0001 for all pairwise comparisons). DAS28: Disease Activity Score at 28 joints; RTX: rituximab.
On-flare versus fixed-interval retreatment
Three registries (Portugal, Russian Federation, and Slovenia) identified the reason for retreatment (fixed interval or on flare). A total of 800 patients were re-treated at least once (minimum 2 cycles of RTX) and the retreatment strategy was reported by the treating physician. The strategy was on-flare retreatment in 616 cases (442 at first and 174 at second retreatment) and fixed-interval retreatment in 184 cases (128 at first and 56 at second retreatment). Baseline (start of each retreatment) characteristics of patients in the 2 retreatment groups at first and second retreatment are summarized and compared in Table 2A and Table 2B, respectively. Patients receiving fixed-interval retreatment had a significantly lower DAS28 (p < 0.0001) at the start of each cycle (baseline = visit 1 of each treatment cycle) compared with those re-treated on flare, as expected (Table 2A and Table 2B).
Characteristics of patients at start of second cycle (first retreatment) who were re-treated on flare or at a fixed interval. No. patients with available information is shown in square brackets. Values are mean ± SD unless otherwise specified.
Characteristics of patients at start of third cycle (second retreatment) who were re-treated on flare or at a fixed interval. No. patients with available information is shown in square brackets. Values are mean ± SD unless otherwise specified.
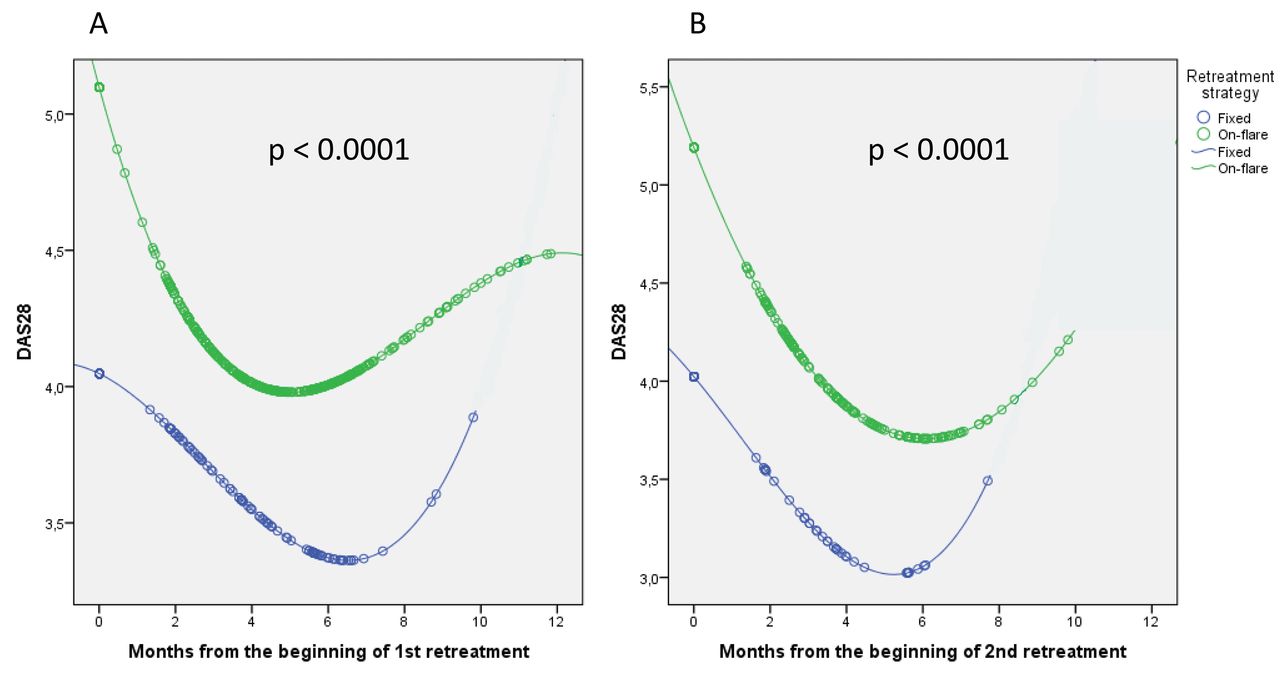
The total number of visits during the first 12 months from the beginning of the first and second retreatment was 1171 and 480, respectively. In the adjusted mixed-model analysis, we compared the 2 retreatment groups for the first and the second retreatment separately using estimated marginal means. For the first retreatment, a fixed-interval retreatment group yielded significantly better results than the on-flare group (estimated marginal mean DAS28 = 3.8, 95% CI 3.6–4.1 vs 4.6, 95% CI 4.5–4.7, p < 0.0001). Similar results were found for the second retreatment (estimated marginal mean DAS28 = −3.7, 95% CI 3.3–4.0 vs 4.6, 95% CI 4.4–4.8, p < 0.0001). The evolution of the predicted DAS28 according to retreatment strategy that resulted from the adjusted mixed-model analyses for the first and second retreatment is shown in Figure 3A and Figure 3B, respectively. The retreatment strategy had a significant effect on the model in both the first and second retreatment (p < 0.0001).

{kind=link}
{kind=link}
{kind=link}
Progression of DAS28 during the first 12 months from the beginning of each retreatment according to retreatment strategy based on adjusted mixed-model analyses for the (A) first and (B) second retreatment. The retreatment strategy had a significant effect on the model. DAS28: Disease Activity Score at 28 joints.
DISCUSSION
The results of our large, observational, international, collaborative study support the effect of repeated treatment cycles with RTX on RA disease activity. Disease activity in patients who continue with RTX is likely to further decrease with repeated RTX treatment cycles. This is a clinically relevant and important observation, which partly confirms some previous clinical trials and observational studies10,13. In our study, the opportunity of further improvement was demonstrated both by DAS28 reduction during the first 12 months from the beginning of each treatment (Figure 2) and the proportion of patients in low disease activity/remission and EULAR good response at the start of each treatment (Figure 1). By selecting patients with at least 4 treatment cycles, we minimized the risk for selection bias and could assess the magnitude of further improvement of disease activity with repeated cycles of RTX. The fact that we assessed remission or low disease activity rate as well as EULAR good response rate at the beginning of each following cycle might lead to an understatement of the effect of repeated treatments on disease activity, because many patients have flared at the time of the second, third, or fourth treatment cycles. This further supports our findings and acts in favor of retreatment.
The optimal retreatment strategy is still a matter for discussion. In the most recent consensus statement on the use of RTX in RA, repeated treatment with RTX should be considered, especially in patients who have not achieved remission or low disease activity in line with the treat-to-target and EULAR RA management recommendations14. However, the optimal treatment paradigm for RTX has not been definitively determined. In this study, the majority of patients were re-treated on flare, but we also had data on a considerable number of patients who were re-treated at a fixed interval. The results of the mixed-model regression analysis suggested that a fixed retreatment approach, before a flare occurs, might lead to more favorable results. One might argue that the results are expected, because the on-flare retreated patients had higher DAS28. However, as is obvious from Figure 3A and Figure 3B, during the first months after the first and second retreatment, patients re-treated on a fixed interval constantly have lower DAS28 than those re-treated on flare, and this is clinically relevant and closer to the treat-to-target approach.
This finding is in agreement with previous findings from the MabThera In Rheumatoid Arthritis registry, where patients who were re-treated before they flared achieved significantly lower disease activity compared with those re-treated after they flared10. Similar results were also found in an observational study from Finland, where repeated courses of RTX produced sustained effectiveness in patients with RA who had responded to the first treatment course15. In the same study, the approach of re-treating on flare led to delayed RTX retreatment and disease flare in a significant proportion of patients. A regular retreatment every 6 months in patients who were not in remission allowed better control of disease activity15. In a retrospective analysis of patients with RA receiving multiple courses of RTX, a retreatment regimen based on 24-week evaluations and a treat-to-target approach was associated with better effectiveness and tighter control of disease activity compared with treatment as needed16. The optimal dose of RTX remains insufficiently defined, both at first cycle and in repeated treatment cycles, although the approved dose is 1000 mg × 2. However, data suggest an overall equivalence of 2 × 500 mg with the licensed dose of 2 × 1000 mg for clinical efficacy outcomes and medium-term maintenance of radiographic nonprogression14,17. Further, a noninferiority randomized controlled trial showed that following a clinical response to a first course of RTX in RA at the licensed dose of 1000 mg × 2, retreatment with RTX at 1000 mg × 1 results in efficacy outcomes that are noninferior to those achieved with retreatment at 1000 mg × 218. A limitation to our current study is that we were unable to examine the retreatment doses in detail.
Our study has also some limitations. Significant heterogeneity between countries was observed. Country was therefore included as a random factor in the mixed-model analysis. On the other hand, the differences in patient population and treatment protocols could also be regarded as a strength. Patients were not randomized to the 2 retreatment strategy groups; therefore, the 2 groups were not completely balanced regarding baseline characteristics. We tried to partially overcome this problem by adjusting for baseline differences. Not all countries had information about the reason for retreatment, which limited the number of patients in the second analysis. Significant differences between the on-flare and the fixed retreatment groups were observed regarding some treatment characteristics, such as concomitant csDMARD and corticosteroid use. The percentage of patients treated with concomitant corticosteroids and csDMARD at the time of first retreatment was significantly different (Table 2A). This could mean a lower dependence by corticosteroids in the fixed retreatment group, while the higher prevalence of csDMARD in this group could signify an increase in maintenance of the clinical response. Unpredictably, at the time of the second retreatment, the percentage of concomitant corticosteroids and csDMARD was the same in the 2 groups, with a significant increase in patients treated with corticosteroids in both groups and a decrease in patients in csDMARD co-therapy compared with the time of the first retreatment (Table 2B). This discrepancy is quite difficult to interpret; it could represent a therapeutic choice, but it could also be random because the number of patients in this subanalysis was significantly lower. In the adjusted analysis, both concomitant corticosteroids and csDMARD were included as potential confounders. Another limitation was that on flare and fixed interval were defined according to the treating physician. This might explain why the time from first cycle to the second and third varied among individuals treated on fixed interval (Table 2A and Table 2B).
Because patients who are re-treated at a fixed interval receive more treatment cycles, it would be interesting and important to know whether these patients are at higher risk for adverse events, such as infections. Systematic collection of high-quality safety data was not possible in our real-life study, and data on adverse events are therefore not reported. Previous studies have not shown any significant effect of repeated treatment cycles on safety16,19. However, the incidence of hypogammaglobulinemia [immunoglobulin (Ig) M and IgG] may increase with higher doses of RTX in patients with RA. In an observational study, an association was found between low IgG levels and serious infections20, while others could not show any significant correlation to the serious infections rate3. There is indeed increasing concern about higher cumulative doses and occurrence of persistent hypogammaglobulinemia21. More evidence is needed regarding the safety of repeated retreatment. No cost-effective analysis could be performed in our study. Other studies have shown that the cost-effectiveness of RTX retreatment on flare is at least equivalent to that of a more intensive regimen, such as every 6 months22.
Significant strengths of the study include the large number of patients, the generalizability of the results, the possibility of examining different treatment strategies in different countries, the possibility of analyzing multiple courses of RTX in a real-life population of patients with RA, and the long followup.
Repeated retreatment with RTX can lead to further clinical improvement after the first course of RTX. A fixed retreatment strategy with RTX in RA seems to be more effective than the strategy of re-treating on flare.
- Accepted for publication November 4, 2016.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.