
Abstract
Objective. Cryopyrin-associated periodic syndrome (CAPS) is a group of inherited autoinflammatory disorders caused by mutations in the NLRP3 gene resulting in the overproduction of interleukin 1β. NLRP3 mutations cause a broad clinical phenotype of CAPS. The aims of the study were to evaluate clinical, laboratory, and genetic features of a 5-generation family with CAPS focusing in detail on ocular symptoms.
Methods. In a retrospective observational cohort study, consecutive family members were screened for the presence of the NLRP3 mutation. Patients underwent standardized clinical, laboratory, and ophthalmological assessments. The genotype-specific risk of ophthalmological findings and other organ symptoms was determined.
Results. Twenty-nine patients were clinically affected. The A439V mutation encoded by exon 3 of the NLRP3 gene was found in 15 of 37 family members (41%). The most common clinical features were musculoskeletal symptoms, headaches, and ophthalmological symptoms. The mutation-positive patients were characterized by more frequent skin rashes, ocular symptoms, arthralgia, arthritis, and severe Muckle-Wells syndrome (MWS) Disease Activity Score. Rosacea was diagnosed in 8 patients.
Conclusion. The NLRP3 mutation A439V is associated with a heterogeneous clinical spectrum of familial cold autoinflammatory syndrome/MWS-overlap syndrome. Skin rash and eye diseases, such as conjunctivitis and uveitis, were positively correlated with this mutation.
- MUCKLE-WELLS SYNDROME
- FAMILIAL COLD AUTOINFLAMMATORY SYNDROME
- NLRP3 MUTATION
- UVEITIS
- ROSACEA
Cryopyrin-associated periodic syndrome (CAPS) represents a group of rare inherited autoinflammatory disorders characterized by recurrent attacks of fever, rash, and arthralgia. The prevalence of CAPS is estimated at about 1 per million1,2. CAPS encompasses a spectrum of diseases from the mildest form, familial cold autoinflammatory syndrome (FCAS), through Muckle-Wells syndrome (MWS), to the most severe form, neonatal-onset multisystem inflammatory disease (NOMID)/chronic infantile neurologic, cutaneous, and articular syndrome (CINCA). FCAS presents in about 95% of the patients by 6 months with cold-induced, urticaria-like rash, fever, and arthralgia. MWS begins later in life than FCAS, and attacks are usually not triggered by cold exposure. The onset of CINCA starts at or within several weeks of birth and includes high fever, aseptic meningitis, arthritis with bone overgrowth, and secondary amyloidosis that contributes to mortality3,4,5.
All 3 disorders are associated with mutations in the NLRP3 gene on chromosome 1q44, which are generally inherited autosomal-dominant6. The prevalence of NLRP3-associated diseases is estimated in 1 in 360,000 people7. The NLRP3 gene encodes the cryopyrin protein (NALP3, NLRP3), a key component of the inflammasome complex that regulates the production of interleukin 1β (IL-1β). NLRP3 forms a protein complex with ASC resulting in activation of caspase-1 that, in turn, cleaves the precursor form of IL-1β to its activated form4,5,8. Therefore, dysfunction of the NLRP3 inflammasome leads to the overproduction of IL-1β, which is responsible for the characteristic features in patients with CAPS4,5,8.
The NLRP3 mutation A439V is 1 of the most common mutations in multiplex families with CAPS7,9. The A439V mutation is not regarded as a sequent variant such as V198M or Q703K, which are observed in the normal population. Rather, A439V is considered a CAPS disease-causing mutation, although the overall clinical phenotype is rather mild. The A439V mutation was first entered into the Infevers database in 2002 by Hal Hoffman (fmf.igh.cnrs.fr/ISSAID/infevers/detail_mutation.php).
The aims of our study were to (1) characterize clinical phenotype in a large, 40-member family including 15 individuals carrying the A439V mutation in the NLRP3 gene, (2) evaluate ophthalmological involvement, and (3) investigate the difference between mutation-positive and mutation–negative patients.
MATERIALS AND METHODS
Study design
A single-center retrospective observational cohort study of 40 living members, covering 5 generations, was conducted. All 40 family members were screened by standardized questioning for CAPS-associated symptoms10. Genetic testing for the NLRP3 mutation was performed in 37 family members independent of their clinical features. Exon 3 of the NLRP3 gene was amplified using PCR. In addition, sequencing of exons 3, 4, and 6 of the NLRP3 gene, as well as exons 2, 3, 4, and 6 of the TNFRSF1A (tumor necrosis factor receptor superfamily, member 1A) gene, was performed in 3 patients without mutation in exon 3 of the NLRP3 gene. Written informed consent was obtained from all family members prior to NLRP3 mutation testing. The study was approved by the Institutional Review Board of the Faculty of Medicine of the University of Tuebingen (241/2008B01).
Patients
Family members were eligible if they met the following criteria: (1) clinical features of CAPS with NLRP3-positive mutation or (2) clinical features of CAPS with NLRP3-negative mutation.
Demographics and clinical data
Demographic data included sex, ethnicity, and age at diagnosis of CAPS. A targeted review of clinical features was conducted by an experienced rheumatologist and consisted of fever, headache, ocular symptoms (conjunctivitis, uveitis, papillary edema, rosacea), hearing loss, skin rash (cold-induced), oral ulcers, musculoskeletal symptoms (arthralgia, arthritis, myalgia), abdominal pain, and renal symptoms (proteinuria, hematuria, renal failure). All clinical data were documented using the Arthritis and Rheumatology Documentation and Information System.
MWS Disease Activity Score (MWS-DAS)
The MWS-DAS was applied as described previously11. Organ involvement (fever, headache, eye involvement, hearing impairment, oral ulcers, abdominal pain, renal disease, skin rash, and musculoskeletal symptoms) was scored as follows: 0 = the absence of symptoms, 1 = mild symptoms, and 2 = severe symptoms. The maximum score of the MWS-DAS was 20. An MWS-DAS of < 10 reflected a mild disease, whereas a score of ≥ 10 indicated a severe disease activity.
Inflammation markers and cytokine profiles
The following laboratory variables were measured: (1) erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), and (2) MWS biomarkers, including serum amyloid A (SAA), S100A12, TNF-α, and IL-6. These variables were not examined at the time of clinical exacerbation, but at the baseline visit of our study.
Immunopathological variables
An ELISA was used to analyze antinuclear antibodies, smooth muscle antibodies, antimitochondrial antibodies, anti-endothelial antibodies, antisarcolemmal antibodies, antiserotonin antibodies, antiganglioside antibodies, and anti-central nervous system antibodies. Serum antibodies such as immunoglobulin A (IgA), IgM, and IgG (IgG1, IgG2, IgG3, and IgG4) were also measured. These immunopathological variables were only investigated in mutation-positive family members.
Ophthalmologic evaluation
A complete ocular examination was performed, including best-corrected visual acuity (VA) using a Snellen chart and intraocular pressure (IOP) values measured by Goldmann applanation tonometry. In addition, the pupil was dilated for the examination of the ocular fundus.
Treatment
Thirteen mutation-positive patients were treated with canakinumab, a fully human anti-IL-1β monoclonal antibody, at a dose of 150 mg subcutaneous for ≥ 40 kg body weight or 2 mg/kg for < 40 kg body weight. All these patients had conjunctivitis (100%), and anterior uveitis was seen in 9 patients (69%)12.
Statistical analysis
Baseline demographic findings, clinical data, laboratory variables, and MWS-DAS were analyzed using descriptive statistics (mean ± SD). Clinical features of mutation-positive and mutation-negative patients were compared with the Student t test for continuous data and the chi-square test or Fisher’s exact test for categorical variables. Correlation between ophthalmologic and other organ symptoms was measured by Spearman correlation coefficient. P values < 0.05 were considered statistically significant. All statistical analyses were performed using commercial software (SPSS version 19.0, SPSS Inc.).
RESULTS
Patients
Our study screened 40 members (17 men and 23 women) by standardized questioning for CAPS-associated symptoms. Because 37 members completed the questionnaire, only the features of those patients were statistically analyzed. The A439V mutation in the NLRP3 gene was identified in 15 (41%) of 37 family members. The demographic characteristics and the pedigree are presented in Table 1 and Figure 1.

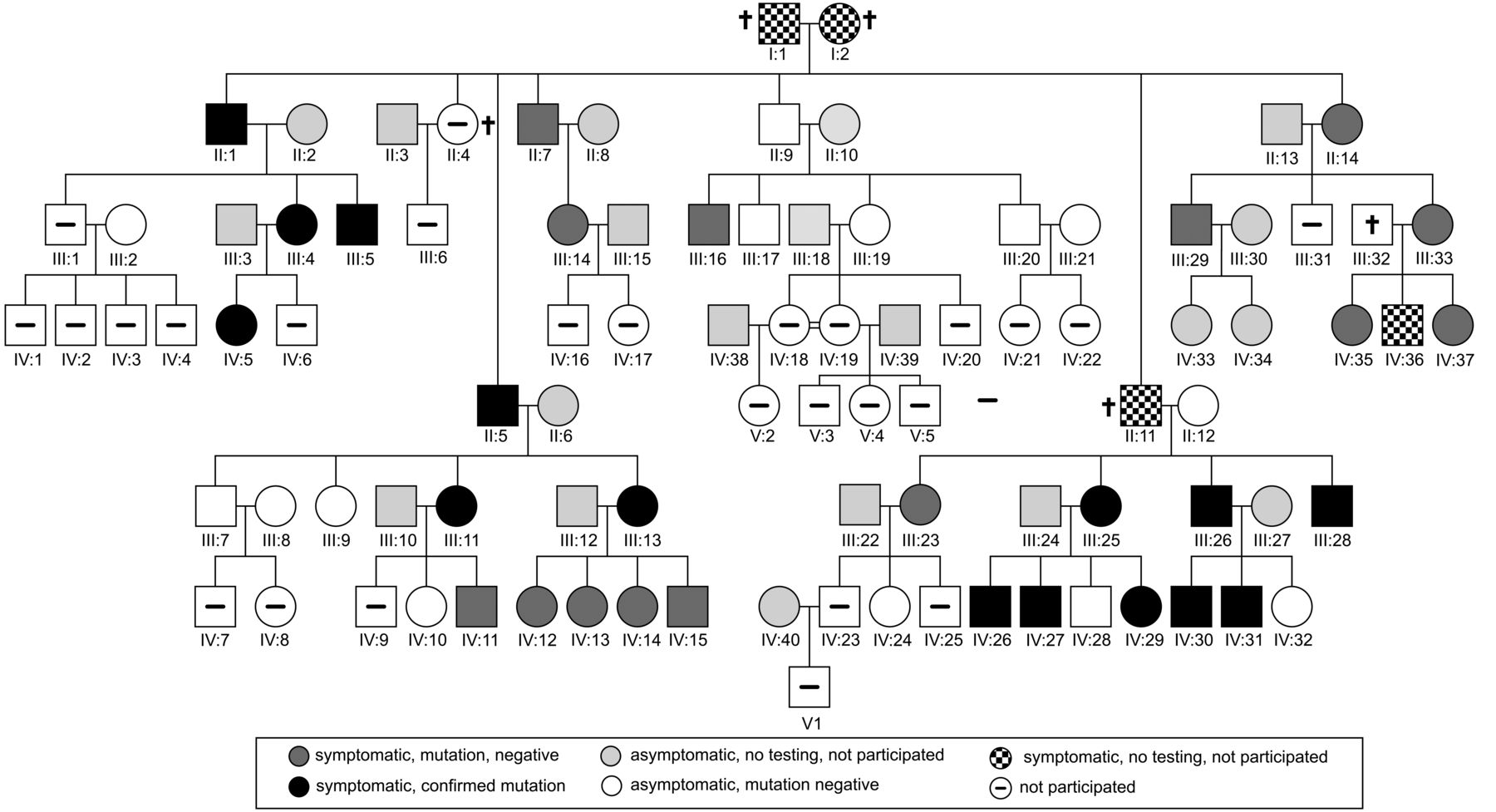{kind=link}
Forty family members were screened for symptoms of CAPS. Symptomatic mutation-positive family members are depicted in black, symptomatic mutation-negative members in grey, and asymptomatic members in white. CAPS: cryopyrin-associated periodic syndrome.
Demographic characteristics and A439V NLRP3 mutation status in a family with FCAS/MWS-overlap syndrome. Values are n (%) unless otherwise specified.
Clinical presentation
All 15 mutation-positive and 14 of the mutation-negative patients had evidence of MWS-associated symptoms. In mutation-positive patients, the most common clinical manifestations were musculoskeletal, skin, and ocular symptoms. Arthralgia was reported in all 15 (100%) and arthritis in 9 (60%). A skin rash was reported in 15 patients (100%), mostly appearing after cold exposure (80%). The ocular symptoms such as conjunctivitis, uveitis, and rosacea were described in 13 (87%), 10 (67%), and 5 patients (33%), respectively. Both cold-induced rash and conjunctivitis were more typical for FCAS, whereas fatigue, arthralgia, and arthritis were seen more often in patients with MWS.
In mutation-negative patients, fatigue (86%), arthralgia (71%), and myalgia (50%) were the most common clinical symptoms. The second most common organ manifestation was ocular involvement (64%).
Other clinical symptoms such as abdominal pain, hearing loss, and renal symptoms ranged between 21% and 40%. Oral ulcers were present in 7 patients, and fever was described only in 4 patients. Headache was familial migraine without association with MWS.
The clinical phenotypes of both mutation-positive and mutation-negative patients significantly differed for skin rash (p = 0.001), cold-induced rash (p = 0.003), arthritis (p = 0.02), and arthralgia (p = 0.04) in the A439V patients and fever episodes (p = 0.04) in the non-A439V patients (Table 2).
Clinical features and disease activity score in the mutation-positive and mutation-negative patients. Values are n (%) unless otherwise specified.
Hearing loss
The detailed data about hearing loss was only available for mutation-positive patients. There were 3 patients with mild sensorineural hearing loss and 3 patients with moderate sensorineural hearing loss. All these patients had fatigue, conjunctivitis, and arthralgia. Five of these patients (83%) showed cold-induced rash, and renal symptoms were present in 4 patients (66.6%). In 50% of the patients, arthritis, myalgia, and headache were observed.
MWS-DAS
The mean MWS-DAS was 5.62 ± 3.47. A severe MWS-DAS (≥ 10) was documented in 5 patients (17%), while 24 patients (83%) had mild MWS disease activity (Table 2).
In the mutation-positive patients, a severe MWS-DAS (≥ 10) was noted in 5 patients. However, none of mutation-negative patients had severe MWS disease activity (p = 0.04; Table 2).
Inflammation markers and cytokine profiles
Classic inflammation markers such as ESR and CRP were increased in 3 (10%, mean ± SD: 14 ± 12) and 11 patients (38%, mean ± SD: 0.53 ± 0.64), respectively. These levels were elevated: serum SAA in 10 patients (35%, mean ± SD: 9.9 ± 12.2), IL-6 in 6 of 26 patients (23%, mean ± SD: 3.85 ± 3.16), TNF-α in 24 of 26 patients (92%, mean ± SD: 14.28 ± 6.63), and S100A12 in 24 patients (83%, mean ± SD: 301 ± 228). Patients with the A439V mutation had significantly higher levels of CRP (p = 0.02) and SAA (p = 0.05). Other inflammation markers did not differ significantly between mutation-positive and mutation-negative patients.
Immunopathological variables
Hypergammaglobulinemia and nonspecific stimulation of antibodies were found in 8 patients (73%) and 7 patients (74%), respectively. Anti-serotonin antibodies and antiganglioside antibodies were observed in 4 patients and in 1 patient, respectively.
Ophthalmologic evaluation
Ocular symptoms were present in 24 patients [83%, grade 1: 18 patients (75%) and grade 2: 6 patients (25%)] and were fairly positively correlated with headache (c = 0.5, p = 0.006), skin rash (c = 0.55, p = 0.003), and abdominal pain (c = 0.37, p = 0.05). Conjunctivitis was reported in 19 patients [66%, grade 1: 14 patients (74%) and grade 2: 5 patients (26%)] and was fairly positively correlated with headache (c = 0.57, p = 0.001) and skin rash (c = 0.48, p = 0.008), and fairly negatively correlated with the age at diagnosis (c = 0.64, p = 0.001). Uveitis was described in 11 patients [38%, grade 1: 5 patients (45%) and grade 2: 6 patients (55%)] and was fairly positively correlated with headache (c = 0.37, p = 0.05) and skin rash (c = 0.61, p = 0.001), and fairly negatively correlated with the age at diagnosis (c = 0.4, p = 0.03). Rosacea was observed in 8 patients (28%), and was fairly positively correlated with hearing loss (c = 0.36, p = 0.05).
All these clinical symptoms occurred significantly more often in mutation-positive patients (Table 3). The mean recurrence number of uveitis was 3.5 in patients with positive-mutation versus 0 in negative-mutation patients. The VA and the IOP did not differ significantly between the mutation-positive and mutation-negative patients (VA 0.0 logMAR ± 0.17 vs 0.0 logMAR ± 0.19; IOP 13 ± 2 vs 14 ± 2).
Ocular symptoms in the mutation-positive and mutation-negative patients. Values are n (%) unless otherwise specified.
Glaucoma did not occur in any patient. Age-related cataract developed in 2 patients and steroid-induced cataract in 1 patient. No inflammation-related complications such as posterior synechiae were observed. No signs of posterior inflammation were found.
Effect of canakinumab on ocular involvement
During the treatment with a mean duration of 26 months (range 24–36), uveitis remained absent and moderate conjunctivitis was observed in 1 patient only12.
DISCUSSION
Our study determined the baseline ophthalmologic characteristics, the clinical phenotype, the genotype, and the associated laboratory variables in a large family covering 5 generations. In 15 family members, the A439V mutation encoded by exon 3 of the NLRP3 gene on chromosome 1 was identified. All 15 mutation-positive patients were symptomatic in accordance with the study on NLRP3 E311K mutation in 42 family members10. However, our 14 of 22 mutation-negative family members (63%) also showed mild clinical symptoms, which can be observed in patients with CAPS. Therefore, there was no clear correlation between genotype and phenotype.
To date, the A439V mutation was described by Hoffman, et al in a 4-generation family with FCAS6 and by Hentgen, et al in a French family presenting an overlapping clinical phenotype of CINCA and MWS13. Further, Shakeel and Gouws reported a case of a female patient with MWS and recurrent attacks of acute anterior uveitis associated with the A439V mutation14.
In our study, the majority presented with musculoskeletal and ocular symptoms. Cold-induced rash was the second most common organ manifestation. Renal symptoms, hearing loss, and abdominal pain were seen in < 40%, whereas fever occurred only in 4 patients. The clinical features of the mutation-positive patients mostly did not differ significantly from the mutation-negative patients. However, patients with the A439V mutation had a significantly higher frequency of conjunctivitis and cold-induced urticaria, and mutation-negative patients showed fever and fatigue significantly more often. In addition, mutation-positive patients experienced significantly more often arthralgia and arthritis. Therefore, the clinical presentation of family members presented in our study is an overlap syndrome of MWS and FCAS15,16,17,18,19,20. Such differences in the phenotype are most likely influenced by genetic and environmental factors9,21. In the cohort of patients with NOMID/CINCA syndrome from Aksentijevich, et al9, 49% of 55 patients were negative for CIAS1 mutations, which indicated genetic heterogeneity of CAPS22. The studies by Aróstegui, et al23 and Saito, et al24 concerned the involvement of low-level mosaicism in CAPS pathology. However, the somatic mosaicism seems to be an uncommon mechanism for the cryopyrinopathies25.
The classic inflammatory markers (ESR and CRP), SAA, and IL-6 were modestly elevated, but biomarkers S100A12 and TNF-α were distinctly raised in all patients in contrast to other cohorts10,11,16. The levels of the classic inflammatory markers depend on the actual disease activity. However, patients with elevated SAA levels, even among those in the second-lowest octile (4 to 9 mg/l), are associated with a risk of death, increased by a factor of 411. Further, S100A12 and TNF-α may indicate upcoming flares before they become clinically apparent26. S100A12, a neutrophil-specific protein belonging to the group of damage-associated molecular patterns, may possibly be associated with subclinical disease progression and risk of the development of amyloidosis27,28. In addition, hypergammaglobulinemia was observed in 73% of our mutation-positive patients, a sign for an acute-phase reaction in response to inflammation29,30.
Similar to other studies, the ocular symptoms were the second most common clinical features after musculoskeletal findings in our family study. The most frequent ocular symptom was conjunctivitis. Anterior uveitis was also seen in a great number of patients. However, the mutation-positive patients experienced more often anterior uveitis (67%) in contrast to other cohorts (15%)10,11,16. In patients with the A439V mutation, both conjunctivitis and anterior ocular inflammation were mild to severe in contrast with the non-A439V patients. In accordance with data of Dollfus, et al31, posterior synechiae did not develop in any patient with anterior uveitis. Similarly, none of the patients had glaucoma or severe cataract requiring surgery or posterior segment abnormalities only. In addition, a positive correlation was observed between ocular symptoms (conjunctivitis and uveitis), headache, and skin rash, which was not determined in the rheumatological studies. To date, such descriptive studies including ophthalmological features of 1 large family were not published; only an international study summarizing 31 case reports diagnosed with the CINCA/NOMID syndrome31 has been published. Except for individual cases, the association between A439V mutation and eye diseases (conjunctivitis and uveitis) has not yet been reported13,14,32. Further, in our study, a prolonged treatment with canakinumab was effective and seems to markedly reduce the recurrence rate of uveitis and prevent the recurrence rate of conjunctivitis. A good response of conjunctivitis to canakinumab was already shown in a double-blind, placebo-controlled randomized study with a treatment duration of 48 weeks33. However, to date, there are only 2 case reports on the treatment of anterior uveitis in patients with CAPS14,34. In these cases, steroid drops14 or cyclosporine34 were used successfully. Nevertheless, there is a lack of data on recurrence and complication rate of patients with CAPS-associated uveitis. Therefore, IL-1 inhibitors are recommended for patients with diagnosed CAPS who have CAPS-associated eye diseases. These inhibitors are approved by the US Food and Drug Administration as a treatment for CAPS.
In our present study, a skin rosacea with ocular involvement was observed in 8 patients, and was positively correlated with hearing loss. However, it was not significantly correlated with the A439V mutation. The current pathophysiological concept of rosacea proposes that an aberrant innate immune response, including Toll-like receptor and NLR (nucleotide-binding domain and leukine-rich repeat-containing) families signaling, has a crucial role by mediating the effects of rosacea trigger factors35. This hypothesis could explain the occurrence of rosacea in our study because these receptors activate the downstream signaling cascade of the IL-1 receptors. However, it is still unclear which part of the signaling cascade is responsible for eye involvement in CAPS.
To our knowledge, ours is the largest family study on 37 patients with FCAS/MWS-overlap syndrome with and without A439V mutation reported to date. The interdisciplinary clinical care setting and data collection process at our center reduced the risk of bias. However, the retrospective design of our study and the lack of IL-1 secretion assay, which may become part of the standard in diagnosing patients with CAPS in the future, should be taken into consideration when the results are evaluated.
Both skin rash and ocular inflammation (conjunctivitis and uveitis) were positively correlated with AV439V mutation. The conjunctivitis was the leading ocular symptom similar to data derived from published reports8,14,25. However, anterior uveitis was reported by 67% of mutation-positive patients. This positive correlation between uveitis and the A439V mutation together with effectiveness of canakinumab on CAPS-associated anterior uveitis have been reported for the first time. The occurrence of uveitis and rosacea should be validated in further studies on patients with CAPS.
- Accepted for publication February 18, 2016.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.