
Abstract
Objective. To evaluate the risk of cerebrovascular disease and cardiovascular disease (CVD) in patients with giant cell arteritis (GCA), and to identify predictors.
Methods. The UK Clinical Practice Research Datalink 1991–2010 was used for a parallel cohort study of 5827 patients with GCA and 37,090 age-, sex-, and location-matched controls. A multivariable competing risk model (non-cerebrovascular/CV-related death as the competing risk) determined the relative risk [subhazard ratio (SHR)] between patients with GCA compared with background controls for cerebrovascular disease, CVD, or either. Each cohort (GCA and controls) was then analyzed individually using the same multivariable model, with age and sex now present, to identify predictors of CVD or cerebrovascular disease.
Results. Patients with GCA, compared with controls, had an increased risk SHR (95% CI) of cerebrovascular disease (1.45, 1.31–1.60), CVD (1.49, 1.37–1.62), or either (1.47, 1.37–1.57). In the GCA cohort, predictors of “cerebrovascular disease or CVD” included increasing age, > 80 years versus < 65 years (1.98, 1.62–2.42), male sex (1.20, 1.05–1.38), and socioeconomic status, most deprived quintile versus least deprived (1.34, 1.01–1.78). These predictors were also present within the non-GCA cohort.
Conclusion. Patients with GCA are more likely to develop cerebrovascular disease or CVD than age-, sex-, and location-matched controls. In common with the non-GCA cohort, patients who are older, male, and from the most deprived compared with least deprived areas have a higher risk of cerebrovascular disease or CVD. Further work is needed to understand how this risk may be mediated by specific behavioral, social, and economic factors.
- GIANT CELL ARTERITIS
- CARDIOVASCULAR DISEASES
- EPIDEMIOLOGY
- HYPERTENSION
- CEREBROVASCULAR DISORDERS
Giant cell arteritis (GCA) is the most common form of vasculitis, with the highest incidence of 7.4 per 10,000 person-years in women aged 70–791. Cardiovascular disease (CVD) and cerebrovascular disease are both increased in patients with GCA2,3,4, with an HR of 2.06 (95% CI 1.72–2.46) for myocardial infarction (MI) and HR 1.28 (95% CI 1.06–1.54) for cerebrovascular accidents in patients versus controls2. The risk of events is highest in the first year2,4, potentially implicating high-dose glucocorticoid use5,6 or increased levels of inflammation, as seen in the general population7 and other rheumatic diseases8,9.
Conventional CV risk factors such as hypertension (HTN), hyperlipidemia, and smoking10 may be implicated in subsequent CVD and cerebrovascular disease in GCA, but this has yet to be proven2. Smoking is known to increase the likelihood of developing GCA11. An association between baseline CV risk factors and severe ischemic events at the time of diagnosis could provide clues as to the development of later CVD or cerebrovascular disease, but this link is debated12. A study of 210 Spanish patients with GCA found an increased risk of a severe ischemic event (defined as a composite endpoint including visual manifestations, claudication of the tongue and jaw, and cerebrovascular accidents) with every conventional CV risk factor (1 of HTN, hyperlipidemia, smoking, or diabetes), with an OR of 1.79 (95% CI 1.03–3.11)13. These results were supported by an Italian study of 180 patients that found that a previous history of HTN and ischemic heart disease was associated with severe ischemic events at diagnosis14. In contrast, a study of 245 GCA and non-GCA subjects from Minnesota, USA, reported no increase in acute coronary syndrome and a lower frequency of CV risk factors at diagnosis in patients with GCA15. In addition, a study of 271 patients from the United Kingdom demonstrated no associations with preexisting HTN or atherosclerosis, but did find an association with social deprivation, with an OR of 4.2 (95% CI 1.3–13.6) for a severe ischemic manifestation between the most and least deprived quintiles12. Social deprivation is an emerging risk factor for CVD and cerebrovascular disease in the general population16, probably mediated by neighborhood deprivation, smoking, physical inactivity, and obesity17,18 or inequalities in pharmacotherapy19. There appears to be a geographical variation in the incidence of GCA20 with higher rates in more affluent areas; whether this affects the development of CVD and cerebrovascular disease in these patients is not known.
The Clinical Practice Research Datalink (CPRD), previously known as the General Practice Research Database, covers a population of 14 million patients from 500 general practices in the United Kingdom21. The available anonymized data21 include consultation records, such as information on diagnoses and clinical outcomes, and prescription records stored as computerized Read codes (standardized clinical codes used in general practice in the United Kingdom). The aim of our study was to evaluate the risk and identify predictors of cerebrovascular disease and CVD in patients with GCA.
MATERIALS AND METHODS
Study design using the CPRD
A 20-year parallel cohort (patients with GCA and matched controls) was observed from January 1, 1991, to December 31, 2010, for the outcomes of cerebrovascular disease and CVD. Non-GCA controls were matched to patients with GCA (6:1) based on the year of birth, sex, and general practice. Ethical approval was given by the CPRD Independent Scientific Advisory Committee.
Outcome measures
We defined 3 binary outcomes using the CPRD Read codes. The first was “cerebrovascular disease,” which was compiled using the Read codes for stroke or transient ischemic attack or cerebrovascular disease. The second was “CVD” and was compiled using the Read codes for ischemic heart disease or MI or CVD. The third, “cerebrovascular disease or CVD” identified patients with either the first outcome or second outcome.
Definition of GCA and controls
Patients with GCA had an incident GCA Read code between January 1, 1991, and December 31, 2010, and ≥ 2 prescriptions for oral glucocorticoids, as per previous validated methods of confirming the diagnosis of GCA within the CPRD20. Patients were aged ≥ 4020 with at least 12 months of CPRD defined up to standard (UTS) data prior to their index diagnosis; patients were excluded if they had a previous diagnosis of cerebrovascular disease or CVD. Controls did not have a diagnosis of GCA or polymyalgia ever recorded in the CPRD, and they had at least 12 months of UTS followup recorded prior to the date of diagnosis of the matched patient with GCA; controls were excluded if they had a previous diagnosis of cerebrovascular disease or CVD.
CV risk factors
Read codes were used to identify a history of hyperlipidemia and HTN. Prescriptions for at least 75% of the year, in any year out of the previous 5 prior to diagnosis of GCA or the matched timepoint in controls, were needed to confirm previous lipid-lowering, antihypertensive, or diabetic treatment. Previous diabetes was flagged by medical Read codes: a prescription of oral diabetic medications for at least 75% of the year, or 2 or more prescriptions of injectable insulin or insulin needles in any year out of the previous 5. All patients diagnosed with GCA were routinely treated with glucocorticoids; therefore their use was not included as a covariate. Smoking and alcohol variables were categorized as “current,” “ex,” and “never.” The body mass index (BMI) variable was the closest recorded before the start of the exposed-to-risk period. The Index of Multiple Deprivation (IMD) combines information from 7 domains of deprivation (income; employment; education, skills, and training; health deprivation and disability; crime; barriers to housing and services; and living environment) to provide a set of relative measures of deprivation for small areas or neighborhoods (known as Lower-layer Super Output Areas) across England22. IMD data were provided in quintiles, from quintile 1 (least deprived) to quintile 5 (most deprived).
Analysis
Descriptive statistics were used to compare patient characteristics of the GCA and control cohorts. The Student t test was used for normal continuous data, the rank sum test for non-normal data, and the chi-square test for categorical data.
The (crude) risk of incident CVD or cerebrovascular disease with GCA compared with non-GCA cohorts was then calculated. Patients with GCA were “exposed to risk” of cerebrovascular disease or CVD from the date of diagnosis to the earliest of the endpoints: date of death, transfer out (left the study), end of study date, or date of cerebrovascular disease or CVD diagnosis (the earlier date was used for the combined outcome CVD). Non-GCA controls were exposed to risk from the same date as their corresponding matched patient with GCA, with the same endpoints.
Cumulative incidence function plots stratified by GCA status, sex, smoking status, and socioeconomic status were used to describe the probability of combined CVD events over time and were tested using the log-rank test.
For each outcome, the relative risk [subhazard ratio (SHR)] between patients with GCA and non-GCA controls was determined by means of a competing risk model using noncerebrovascular/CV death as the competing risk. Univariable models were described, then a full multivariable model adjusting for risk factors (BMI, smoking, alcohol, deprivation, hyperlipidemia, HTN, antihypertensives, diabetes, and lipid-lowering medications) was completed; age and sex were excluded because the cohorts were matched. Two-way interaction effects between GCA status and the vascular risk factors (and each other) were also investigated. Each interaction term was individually tested in the initial multivariable model; significant terms (p < 0.1) were then used to build the final multivariable model. A subgroup analysis for each of the 13 geographical regions was also performed to investigate variations in the relative risk of CVD or cerebrovascular disease.
Competing risk of variables in GCA and non-GCA cohorts
Each cohort was then analyzed individually using the same multivariable model, with age and sex now present in the model to identify predictors. All multivariable survival models were tested for the proportional hazards assumption using Schoenfeld residuals. All statistical analyses were performed using Stata SE v12.0 (StatCorp).
RESULTS
Participants
There were 5827 patients with GCA and 37,090 matched non-GCA controls who met our inclusion/exclusion criteria and were used in our analysis (Figure 1).
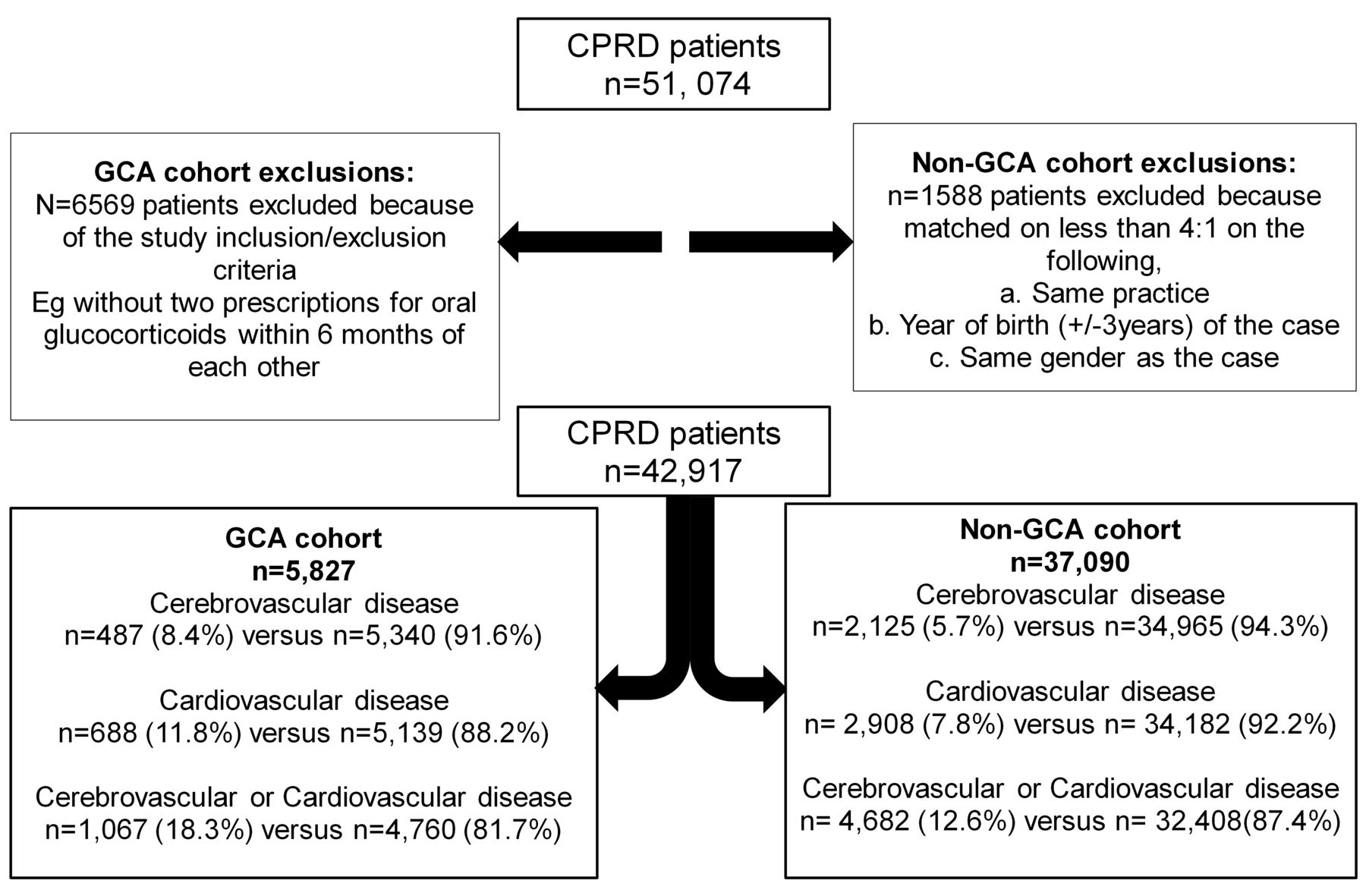
Flow chart. CPRD: Clinical Practice Research Datalink; GCA: giant cell arteritis.
Descriptive statistics
In both cohorts, the mean (SD) age was 71 years (10.7), around 73% were women, and 1 in 9 women were from the most deprived areas (11% IMD quintile 5; Table 1). Patients from the GCA cohort, compared with those from the non-GCA cohort, were more likely to have a previous history of hyperlipidemia (4.8% vs 3.8%), HTN (27.0% vs 25.2%), use of antihypertensive agents (36.7% vs 33.2%), diabetes (8.8% vs 7.9%), and lipid-lowering medication use (12.1% vs 11.5%). They were more likely to be current smokers (18.4% vs 15.9%) and less likely to consume alcohol (72.8% vs 75.0%; Table 1).
Descriptive statistics of the cohorts. P value compares non-GCA and GCA factors. Values are % (n) unless otherwise specified.
The relative risk of cerebrovascular disease or CVD
The risk of cerebrovascular disease, CVD, or “cerebrovascular disease or CVD” was higher in patients with GCA than without (Table 2). The largest difference in risk was observed in the “cerebrovascular disease or CVD” analysis where the risks in the GCA and non-GCA cohorts were 18.3% and 12.6%, respectively, giving a crude risk ratio of 1.45.
Relative risk of cerebrovascular disease, CVD, or both in non-GCA patients and patients with GCA. Significant interactions p < 0.05 are cerebrovascular disease: HTN and anti-hypertensives, HTN and lipid-lowering medications, HTN and hyperlipidemia; CVD: HTN and antihypertensive; cerebrovascular disease or CVD: HTN and antihypertensives, HTN and hyperlipidemia.
In the multivariable competing risk model, the SHR for “cerebrovascular disease or CVD” was 1.47 (95% CI 1.37–1.57), cerebrovascular disease was 1.45 (95% CI 1.31–1.60), and CVD was 1.49 (1.37–1.62).
The models were adjusted for risk factors (as described earlier). No 2-way interaction effects were observed between GCA status and the covariates (p > 0.1 for all interactions). However, we included significant 2-way interaction terms between the covariates themselves: HTN and antihypertensives, HTN and lipid-lowering medications, and HTN and hyperlipidemia. Schoenfeld residuals showed that the proportionality assumption was not violated.
No regional variations were seen on subgroup analysis when the multivariable competing risk model for “cerebrovascular disease or CVD” was run for each region in the United Kingdom (Figure 2).
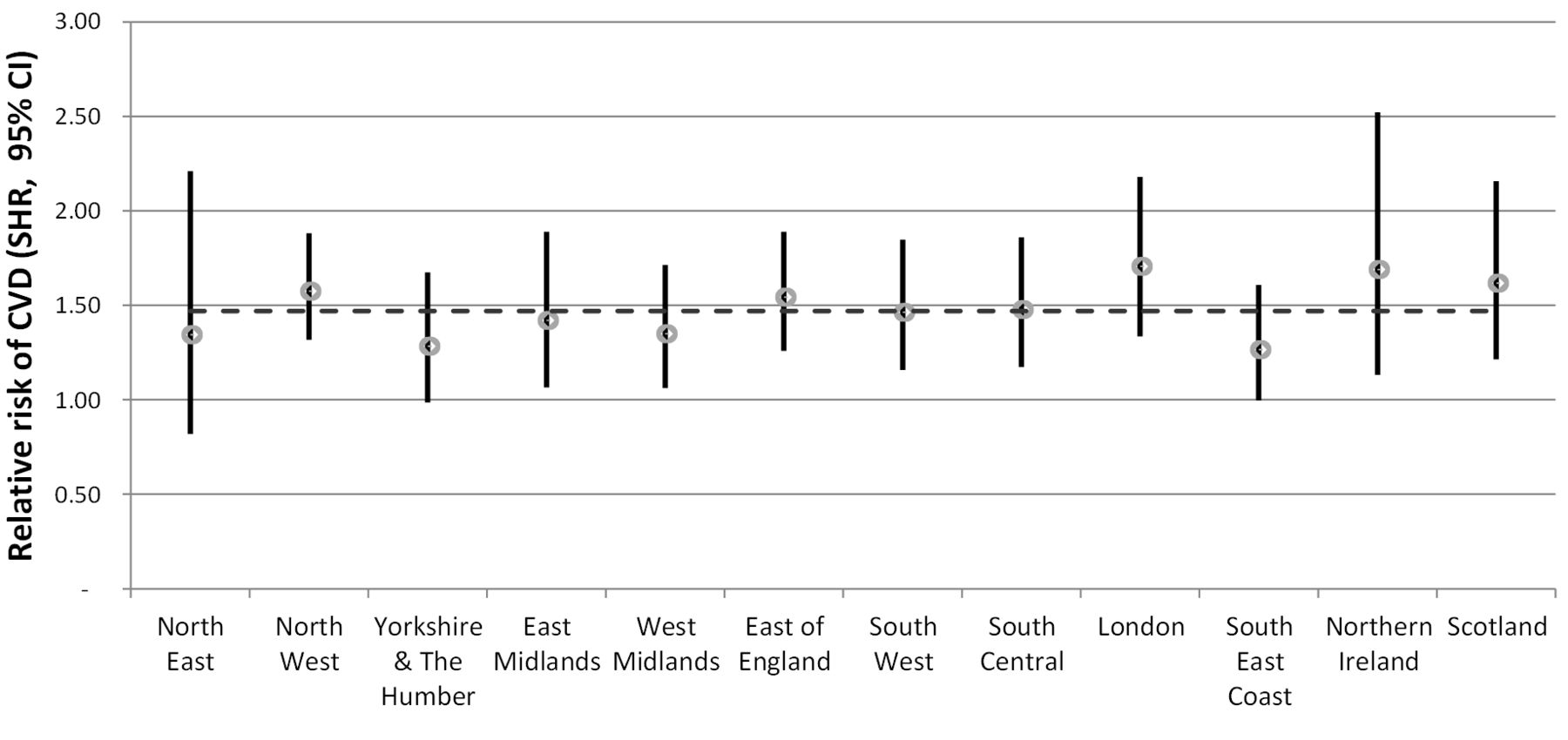
UK regional variations in the relative risk of “cerebrovascular disease or CVD” for patients with GCA compared with non-GCA patients. Overall SHR (1.47) represented by the horizontal dash line. Imputed competing risk models adjusted for body mass index, smoking, alcohol, deprivation, hyperlipidemia, hypertension, anti-hypertensives, diabetes, lipid-lowering medications, and covariate interaction. CVD: cardiovascular disease; SHR: subhazard ratio; GCA: giant cell arteritis.
Predictors of cerebrovascular disease and CVD: Combined outcome of cerebrovascular disease and CVD
In the GCA cohort, these were risk factors for the combined outcome of “cerebrovascular disease and CVD”: increasing age (SHR 1.61 for patients aged 65–70 vs ≤ 65, 95% CI 1.31–1.99), being men (SHR 1.20, 95% CI 1.05–1.38), and being in the most versus the least deprived quintile (SHR 1.34, 95% CI 1.10–1.78). In the non-GCA cohort, these were risk factors for the combined outcome of “cerebrovascular disease and CVD”: increasing age (SHR 1.76 for patients aged 65–70 vs ≤ 65, 95% CI 1.58–1.95), being men (SHR 1.34, 95% CI 1.25–1.43), being in the most versus the least deprived quintile (SHR 1.21, 95% CI 1.08–1.37), current smoking (SHR 1.18, 95% CI 1.08–1.29), previous history of HTN (SHR 1.78, 95% CI 1.59–1.99), and previous history of diabetes (SHR 1.22, 95% CI 1.10–1.36); while previous prescription of antihypertensives was protective (SHR 0.69, 95% CI 0.61–0.79; Table 3).
Predictors of cerebrovascular disease, CVD, or both in non-GCA and GCA cohorts in 6 independent analyses. Multivariable competing risk model (imputed) inclusive of all listed covariates and adjusted for covariate interaction (HTN and antihypertensives, HTN and lipid-lowering medications, HTN and hyperlipidemia). Significant interactions p < 0.05 are cerebrovascular disease non-GCA: HTN and antihypertensives, HTN and hyperlipidemia; CVD non-GCA: HTN and antihypertensives; CVD GCA: HTN and antihypertensives; cerebrovascular disease or CVD non-GCA: HTN and antihypertensives, HTN and hyperlipidemia; cerebrovascular disease or CVD GCA: HTN and antihypertensives. Values are SHR (95% CI).
Predictors of the individual outcomes of CVD or cerebrovascular disease in the GCA and non-GCA cohorts are detailed in Table 3.
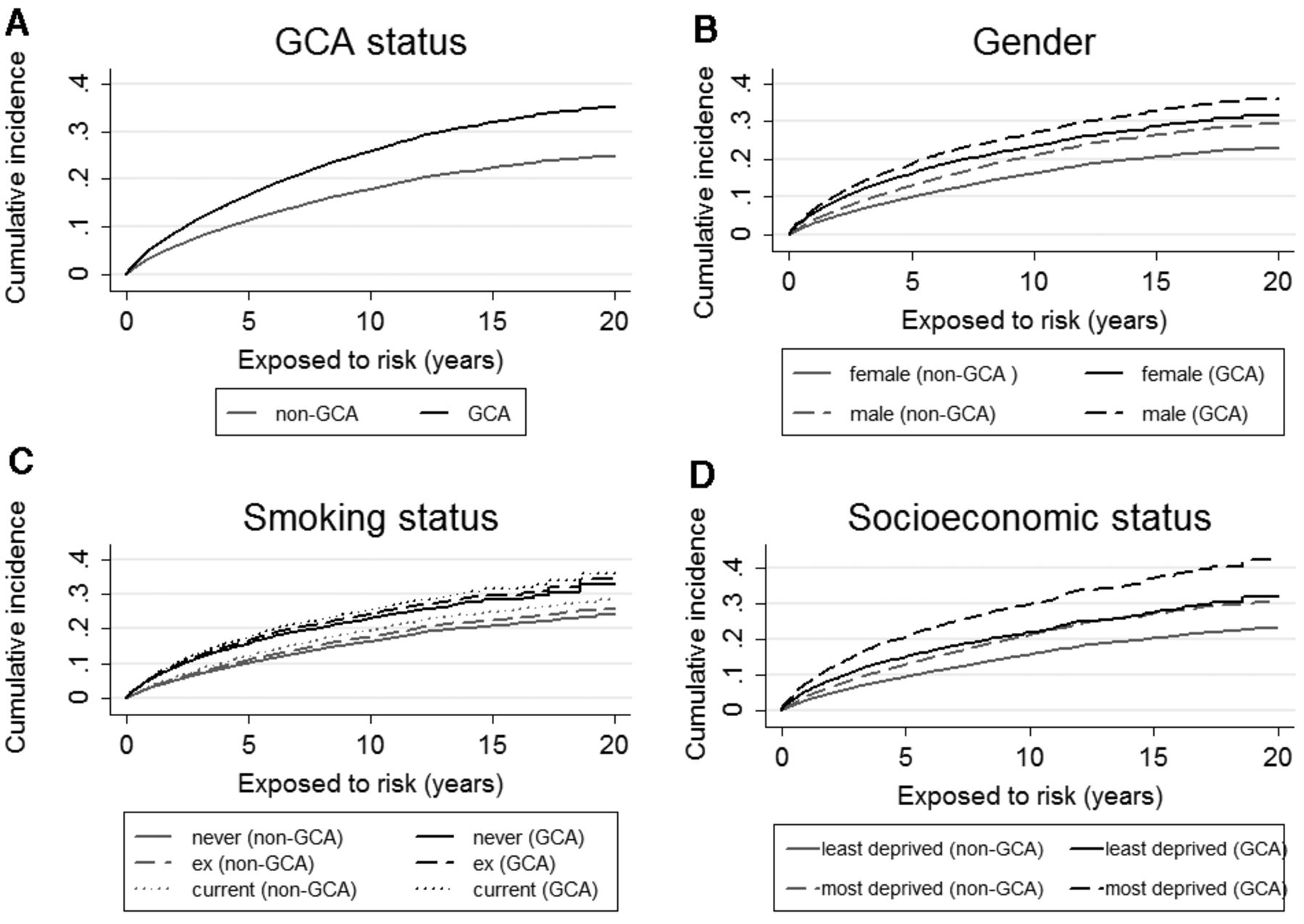
Cumulative incidence plots also demonstrated differences in the risk of “CVD or cerebrovascular disease” when stratified by GCA versus non-GCA diagnosis (increased risk with GCA), sex (increased risk among men with GCA), smoking (increased risk among current smokers with GCA), and socioeconomic status (increased risk among patients from the most deprived areas and with GCA; Figure 3).
{kind=link}
{kind=link}
{kind=link}
Cumulative incidence of CVD or cerebrovascular disease by (A) GCA status, (B) GCA status and sex, (C) GCA status and smoking, and (D) GCA status and socioeconomic status. All plots adjust for age. GCA status, smoking status, and socioeconomic status plots were also adjusted for sex. The log-rank test was used for equality of survivor functions: GCA status p < 0.001; sex (non-GCA) p < 0.001; sex (GCA) p = 0.012; smoking (non-GCA status) p < 0.001; smoking (GCA status) p = 0.1431; socioeconomic status (non-GCA) p < 0.001; socioeconomic status (GCA) p = 0.029. CVD: cardiovascular disease; GCA: giant cell arteritis.
DISCUSSION
Patients with GCA are 50% more likely to develop incident cerebrovascular disease or CVD than age-, sex-, and practice-matched controls, which is in line with previous studies2,4. This effect is independent of conventional CV risk factors and social deprivation. Our study provides new information about the importance of CV risk factors within this population. Lower socioeconomic status, older age (≥ 65), and being men are all independent predictors of “cerebrovascular disease or CVD” within the GCA cohort. A history of HTN is also an independent risk factor for developing CVD in patients with GCA. A wider number of predictors of CVD and cerebrovascular disease was noted in the non-GCA cohort (as per the GCA cohort, but with the addition of previous diabetes as predictive, and lipid-lowering medications and antihypertensives as protective). This may purely be because of the greater statistical power in the non-GCA cohort, as suggested by the lack of any interactions between the main exposure (GCA or non-GCA) and any of the conventional CV risk factors within the overall competing risk analysis. Previous studies in GCA have not found an association between conventional CV risk factors and CV outcomes15 or other ischemic disease12, but sample sizes were relatively small at 245 and 271 patients, respectively, in these studies so they may have been similarly underpowered. In relation to socioeconomic status, to our knowledge, ours is the first study to show an association between the higher levels of deprivation and the development of CVD or cerebrovascular disease in GCA. Social deprivation is known to be associated with CVD within the general population17; our study demonstrates that this is also true of patients with GCA. Further work is needed to understand how this risk may be mediated by specific behavioral, social, and economic factors. For example, there can be significant delays in the initial diagnosis and management of GCA, and this may be associated with an increased incidence of irreversible ischemic complications at diagnosis25. Our study did not identify any regional variations in the risk of developing cerebrovascular or CVD; this may be interpreted as reassuring, but more work is needed to exclude an effect of differing local referral and management protocols.
Ours is a large cohort study of patients with incident GCA (n = 5827) with prospectively recorded data, including baseline risk factors and cerebrovascular disease and CVD outcomes, enabling the identification of risk factors within this population. However, there are limitations. Despite the size of our cohort, greater numbers still may be needed to demonstrate the full range of CV risk factors2 in patients with GCA. It is also not possible to identify biopsy-positive patients or to classify them according to the 1990 American College of Rheumatology criteria26 within the CPRD; instead, a combination of diagnostic code and glucocorticoid prescriptions was used to identify patients with GCA20. This may have resulted in patients being misclassified as having GCA, although inclusion of biopsy-negative patients may underestimate rather than overestimate any potential association between GCA and cerebrovascular disease or CVD. There is also the potential for vascular disease to be more commonly suspected and diagnosed in patients with GCA because they are under closer medical followup postdiagnosis. Read codes were used to define HTN and hyperlipidemia, but not whether patients had an elevated systolic or diastolic blood pressure, or the category of hyperlipidemia, which may be important for differing CV and cerebrovascular outcomes27,28. The proportion of missing data that was imputed, particularly for the IMD (45%), was large. We maintained efficiency by increasing the number of imputed sets from 5 (most commonly used) to 10. However, this process was based on the assumption that values were missing at random. If the values were missing not at random (untestable in the CPRD), our estimates of direct and indirect effects of the IMD on CVD would be affected and this is a limitation of our analysis. Treatment with glucocorticoids was considered part of the diagnosis of GCA in our analysis; their use has, however, been implicated in CVD and cerebrovascular disease, and therefore needs future investigation29,30. In the general population, there is an inverse relationship between physical activity and CVD, with a median risk reduction of 30%–35% in the most- versus the least-active groups31. Information on the amount and intensity of physical activity is not collected through the CPRD, which is another limitation of our study.
In practice, our study suggests that clinicians should be alerted to the fact that patients with GCA are at increased risk of CVD and cerebrovascular disease, particularly if they have preexisting HTN, are older, are men, or live in an area of higher social deprivation. It seems reasonable for patients with other CV risk factors to also be considered as higher risk, but this cannot be categorically stated from our study, possibly because of the lack of power, despite the large sample size. Further work is needed to identify the causal pathways involved in the association between social deprivation and increased CVD and cerebrovascular disease in patients with GCA, so that targeted interventions to address this disparity can be developed.
Footnotes
Supported by a grant from the UK National Institute for Health Research’s Research for Patient Benefit Programme.
- Accepted for publication February 12, 2016.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.