
To the Editor:
Tumor necrosis factor inhibitors (TNFi) are widely used for the treatment of ankylosing spondylitis (AS), with infliximab (IFX) being approved by the US Food and Drug Administration for AS in 2004. Adverse event rates remain low for IFX, with risk of infection being the primary concern. IFX is accompanied by a black box warning highlighting reports of T cell lymphoma in young male patients with inflammatory bowel disease (IBD). These are often rare γδ T cell lymphomas occurring in the setting of concomitant immunosuppressive therapies1.
The patient, an HLA-B27+ white man, first developed back pain at the age of 19 following an episode of trauma. He was diagnosed with AS at 23 and started treatment with IFX (5 mg/kg/6 weeks) in 2003 in addition to naproxen (1000 mg/day). This patient had no comorbidities. February 2015 radiographs documented fusion of the sacroiliac joints (modified New York criteria grade 4) and spinal ankylosis (modified Stoke Ankylosing Spondylitis Spine Score = 72). He has had sustained symptomatic response to IFX with the Bath Ankylosing Spondylitis Disease Activity Index consistently < 4.
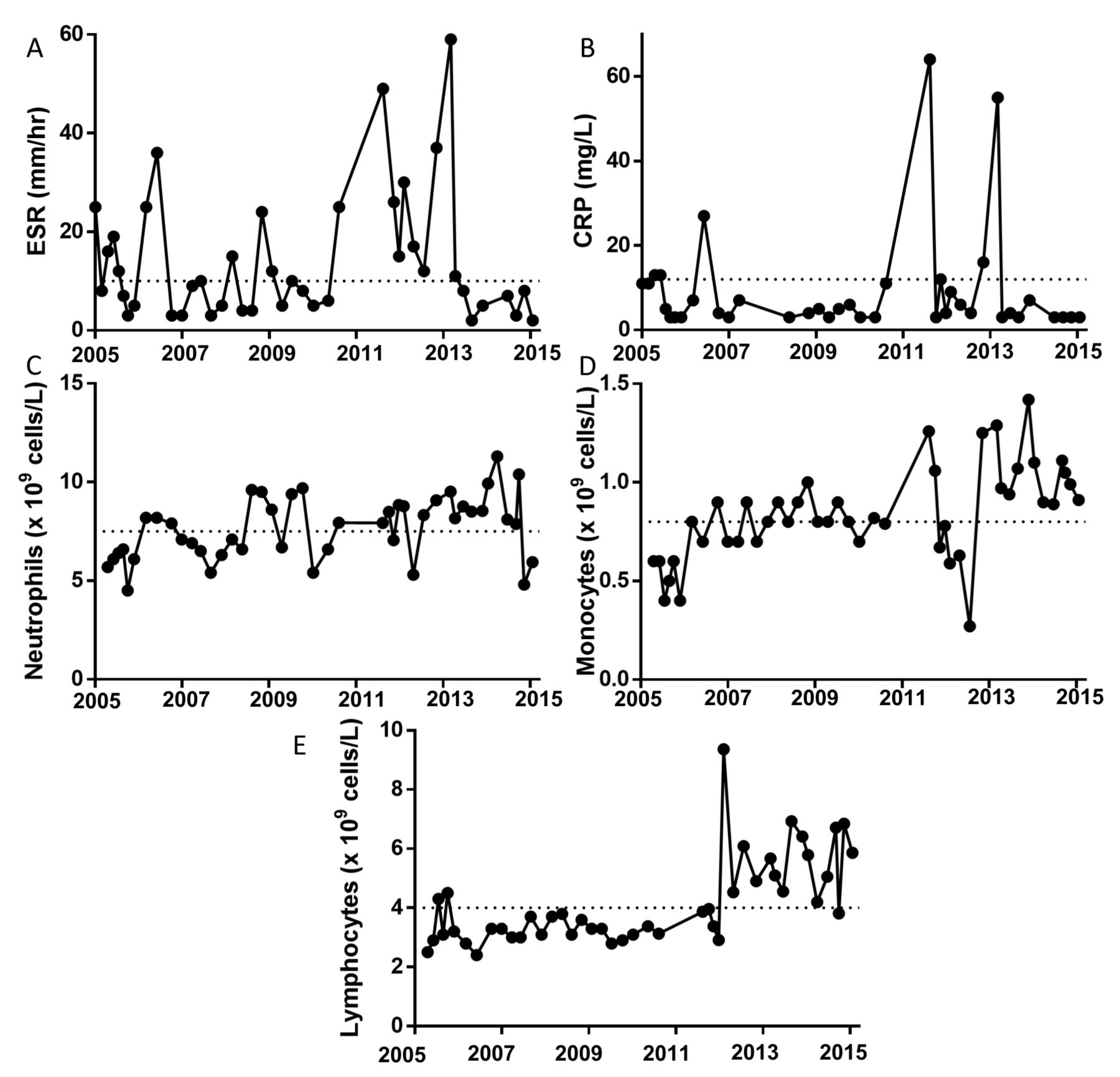
Routine clinical laboratory tests revealed an asymptomatic, afebrile inflammatory event in 2010. This was reflected in an abrupt elevation in erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP; Figures 1A–B), with an elevation in neutrophils and monocytes (Figures 1C–D). Thorough clinical evaluation revealed no evidence for antecedent infection and therefore no grounds for culture testing. Fecal calprotectin was not measured because colitis was not suspected. For these reasons, elevated CRP/ESR was viewed as an AS flare. Following this event, the patient’s lymphocyte count exceeded normal levels (Figure 1E). This lymphocytosis persisted, prompting us to define its cellular nature.
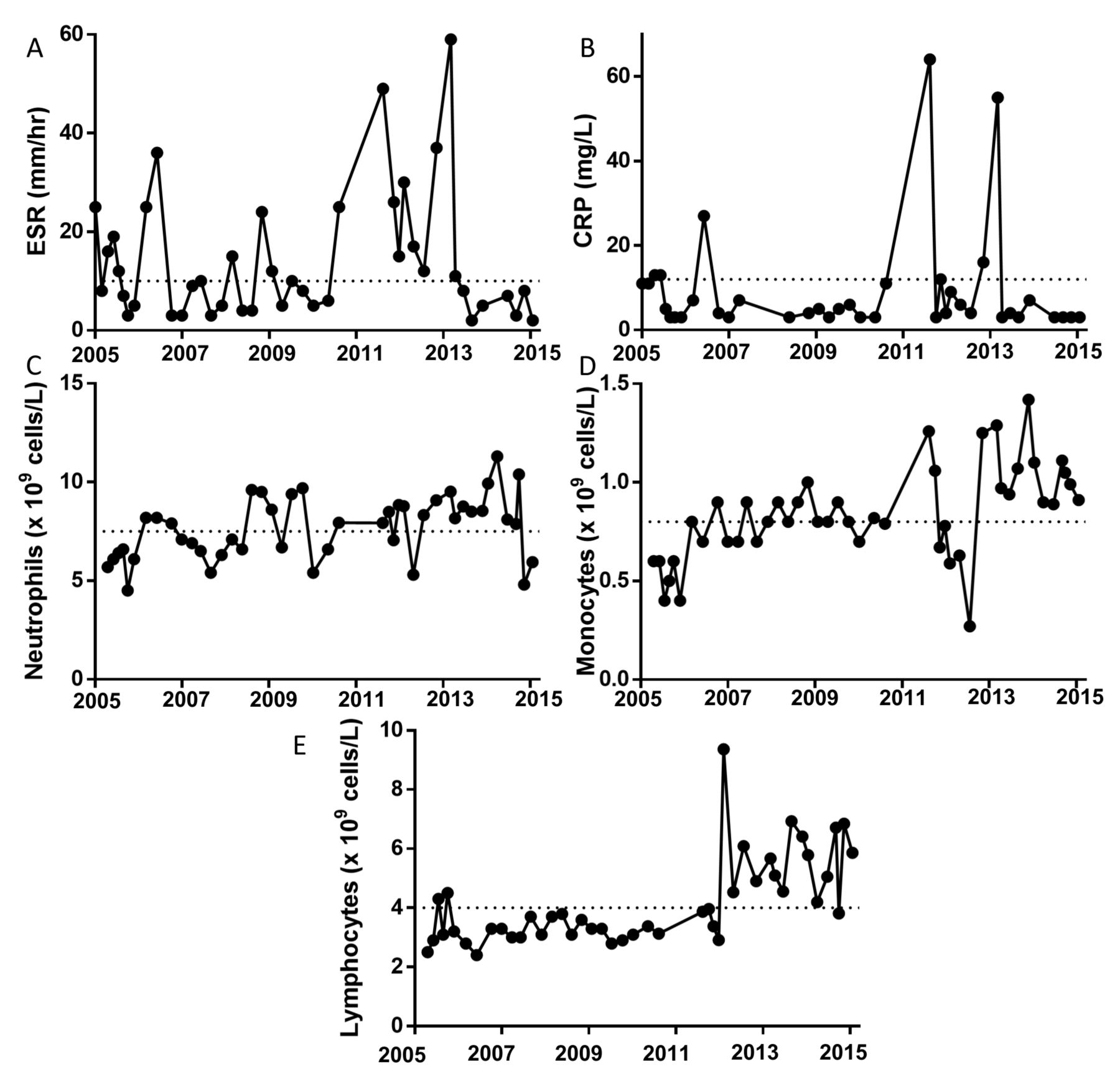
Lymphocytosis following an inflammatory flare in a male patient with AS (Patient A) receiving longterm infliximab. (A) ESR, (B) CRP, and (C–E) WBC count on venous blood performed by clinical diagnostic laboratory on indicated dates. Dotted lines represent limit of normal values. AS: ankylosing spondylitis; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; WBC: white blood cell.
Flow cytometry performed by the clinical hematology laboratory confirmed a normal αβ CD4:CD8 T cell ratio of 1.9, and B cells with polytypical light chain expression. The lymphocytosis was found to be because of an expansion of CD2/CD5/CD7 dim γδ T cells. Diagnostic multiplex PCR was performed to assess T cell receptor (TCR) β and TCRγ repertoire. Results were suggestive of clonal proliferation for TCRγ. Further consultation with hematology included computed tomography imaging, which documented no abnormalities in the lymph nodes or spleen.
Flow cytometry on peripheral blood mononuclear cells (PBMC) was performed in a research laboratory to characterize the expanded γδ T cells. Blood was obtained from repeat visits over a period of 6 months (November 2014 to June 2015) and frozen cells were processed for analysis as previously described2. This demonstrated that the γδ T cell expansion of the patient was restricted to the T cell subset Vδ2+ (Figure 2A). Although normal for CD45RO, the Vδ2+ T cells were low for CD69 and largely CD27-negative. Stimulated Vδ2+ cells produced negligible interleukin 17A (IL-17A), yet were granzyme B+ and interferon-γ (IFN-γ)+. We further characterized the patient’s PBMC with mass cytometry, which showed that his γδ T cells were homogeneous for the 36 markers tested (Figure 2B). Analysis using the viSNE3 data visualization tool demonstrated a tight clustering of the γδ T cells in comparison with the heterogeneous character of CD4+ and CD8+ T cells (Figure 2C), supporting the observations of oligoclonality. The location of the patient’s γδ T cell cluster was distinct from that seen in 5 other male patients with AS of a similar age (3 of the 5 patients were receiving TNFi), suggesting a distinct cell phenotype.

{kind=link}
{kind=link}
Flow cytometric characterization of γδ T cells in our patient demonstrates specific expansion of a homogeneous Vδ2+ T cell population. Flow cytometry performed on frozen PBMC either unstimulated for surface markers or PMA/ionomycin/brefeldin A stimulated for intracellular molecules. (A) FACS used to identify live, singlet lymphocytes (not shown), which were gated on to identify CD3+ T cells in the patient and a representative IFX-treated control (HC). CD3+ cells further gated on to identify Vδ1+/Vδ2+ T cells. The indicated plots display markers specific to the Vδ2+ T cell population with gates based on FMO control (not shown). (B) Mass cytometry used to identify live, singlet, CD3+CD14-CD19-TCRγδ+ cells in the patient’s PBMC for expression of the indicated markers. (C) viSNE analysis performed using 36 markers to cluster PBMC populations in the patient and 5 age-matched male patients with AS. CD3ε, CD4, CD8α, CD14, CD19, CD56, and TCRγδ antigens were used to gate indicated cell populations, with CD45RO signal indicated in color scale (yellow = positive, purple = negative). Graphs show frequency of cells in gate as percent of total live PBMC. (D–G) PBMC from male HC and patients with AS either biologic-naive (−) or receiving longterm IFX examined by FACS using the gating in panel A. Our patient’s PBMC examined at 3 timepoints over 6 months for comparison. Pooled results from 3 independent experiments for (D) Vδ2+ T cell as a frequency of total T cells, (E) granzyme B+, (F) CD27+, and (G) CD69+ as a frequency of Vδ2+ T cells. Graphs displayed as scatterplot with median. Where indicated, HC, bio (−), and IFX-treated patients with AS analyzed by Kruskal-Wallis test with Dunn post-test. Data from single subject representative of all subjects. *** p < 0.0001 (H) IL-17A expression by γδ cell subset in CD3+ PBMC. PBMC: peripheral blood mononuclear cells; PMA: phorbol myristate acetate; IFX: infliximab; HC: healthy control; FMO: fluorescence minus one; AS: ankylosing spondylitis; IFNγ: interferon-γ; bio (−): biologic-naive; Pat. A: our patient; ns: not significant; IL: interleukin; TCR: T cell receptor; NK: natural killer; inflix: infliximab.
We compared the cell profile of the patient to 14 healthy controls (HC), 14 biologic-naive patients with AS, and 12 IFX-treated patients with AS (Table 1 and Figures 2D–G). This comparison demonstrated a distinct elevation in Vδ2+ T cells in IFX-treated patients. IFX-treated patients had a higher frequency of Vδ2+ T cells than HC when compared head-to-head (Mann-Whitney U test, p = 0.006). Vδ2+ T cells from other IFX-treated patients with AS did not display the phenotype seen in our patient. Interestingly, our IFX control cohort contained HLA-B27+ twins, who were disparate for Vδ2 frequency (11.4% vs 4.2%) despite having been treated with IFX for a comparable time period. This observation suggests that the TNFi-associated Vδ2 cell expansion is not genetically determined.
Patient demographics for flow cytometry. Values are mean (range) unless otherwise specified.
In contrast to previous reports in patients with AS4, IL-17A was barely detected in γδ T cells, despite being identifiable in the CD3+ population (Figure 2H). Although reports on IL-17A expression by human peripheral blood γδ T cells are conflicting, a strong body of evidence suggests they require extensive ex vivo cytokine priming to induce IL-17 expression5. In contrast, IL-17–producing γδ T cells can be easily identified in cord blood, mucosal tissue, and murine peripheral blood6.
These results demonstrate that our patient has an expansion of Vδ2+ T cells with an abnormal phenotype. Vδ2+ T cells are known to produce TNF-α, IFN-γ, and granzyme, are abundant in gut tissue, especially in patients with IBD7,8,9, and are responsive to bacterial phosphoantigens through the atypical activating molecule CD277 (butyrophilin-3). Antigenic stimulation can cause a robust expansion of Vδ2+ T cells, which is self-limiting9. The TCR-PCR was suggestive of a clonal expansion, but was not considered diagnostic of lymphoma. The lack of CD62L expression suggests that the patient’s γδ T cells were likely not found in secondary lymphoid organs, which may explain the lack of lymph node/spleen enlargement.
Because TNF-α is inhibitory to Vδ2+ T cell proliferation10, it is possible that IFX has promoted the proliferation of these cells. Further work is required to elucidate such a mechanism. Abnormal cell growth is supported by the striking lack of CD27 expression, an important mediator of apoptosis11,12. With the continued symptomatic control of his AS, the stability of the hematologic variables, and lack of any symptoms consistent with a progressive lymphoid abnormality, the patient elected to continue his IFX treatment because of its profound effect on his quality of life.
We present a case of abnormal expansion of Vδ2+ γδ T cells associated with longterm IFX use. Although there are reports in the literature of IFX-associated γδ T cell lymphomas, especially in young men with IBD, data are lacking on the causation and diagnostic criteria. Our case report may be informative to clinicians noting the development of lymphocytosis during the course of IFX treatment of patients with AS.
Footnotes
Funded by Canadian Institutes of Health Research.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.