
Abstract
Objective. We studied the urinary sediment mRNA level of Th9- and Th22-related cytokines in patients with systemic lupus erythematosus (SLE).
Methods. We quantified urinary mRNA levels of interleukin (IL) 9, IL-10, IL-22, and their corresponding transcription factors in 73 patients with active lupus nephritis, 13 patients with hypertensive nephrosclerosis (HTN), and 25 healthy subjects.
Results. There was no detectable IL-9 mRNA in all samples. Patients with proliferative lupus nephritis had significantly lower urinary IL-22 mRNA levels than those with nonproliferative nephritis (2.2 ± 5.4 vs 8.6 ± 20.0 copies, p = 0.019), and urinary IL-22 mRNA level inversely correlated with the histological activity index (r = −0.427, p < 0.0001). In contrast, patients with lupus nephritis had significantly higher urinary IL-10 mRNA levels than patients with HTN (7.8 ± 18.5 vs 1.9 ± 4.0 copies, p = 0.012), and urinary IL-10 mRNA levels correlated with its intrarenal mRNA levels (r = 0.337, p = 0.004) and SLE disease activity index (r = 0.277, p = 0.018). Urinary IL-10 mRNA level was significantly lower among patients who achieved complete remission than those with partial remission or no response (4.1 ± 6.5 vs 14.1 ± 28.0 copies, p = 0.036).
Conclusion. Urinary IL-22 mRNA level is decreased in patients with SLE with proliferative nephritis, while urinary IL-10 mRNA levels correlates with its intrarenal mRNA level and disease activity. Urinary IL-10 mRNA levels may also predict treatment response. These results suggest that urinary mRNA levels of IL-10 and IL-22 might be used as biomarkers for assessing disease activity and risk stratification in lupus nephritis.
- SYSTEMIC LUPUS ERYTHEMATOSUS
- LUPUS NEPHRITIS
- CYTOKINE
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease characterized by autoantibodies to multiple nuclear antigens. Although almost any organ in the body could be affected, renal involvement of SLE is one of the most severe and devastating manifestations. In general, lupus nephritis develops in 50% to 75% of cases1, and it remains the leading cause of morbidity and mortality in patients with SLE.
The exact pathogenesis of SLE and lupus nephritis is not completely known. Nonetheless, aberrant activation of T cell subclasses probably plays a key role in the initiation and propagation of immune system activation2,3,4. Notably, Th9 and Th22 are 2 described subsets of T cells that are distinct from other known T cell subsets5,6,7. Th9 cells are generated by polarization with transforming growth factor-β and interleukin (IL) 4 during activation with the specific antigen8. In addition to secreting IL-9 as the signature cytokine9, Th9 cells also produce similar amounts of IL-108. On the other hand, Th22 subset produces cytokines such as IL-22, which includes the increase of innate immunity, protection from damage, and enhancement of tissue regeneration6.
Studies showed that Th9 and Th22 cells may contribute to the pathogenesis of several autoimmune diseases including SLE. For example, Ouyang, et al10 found that the percentages of CD4+IL-9+ T cells in circulation are significantly elevated in patients with SLE. In contrast, serum IL-22 concentration is decreased in the patients with SLE11,12. More importantly, treatment with recombinant cytokine or gene therapy delivery of IL-22 could alleviate tissue destruction during inflammatory responses13. Nevertheless, the exact role of Th9 and Th22 cells in the pathogenesis of lupus nephritis remains unknown. The objective of our study was to determine the gene expression of Th9- and Th22-related cytokines in the kidney and urinary sediment of patients with SLE, and to study the relation between Th9- and Th22-related cytokine expression and SLE disease activity.
MATERIALS AND METHODS
Study population
All experimentation procedures were in adherence to the Declaration of Helsinki. We recruited 73 consecutive patients with SLE from 2010 to 2012 who fulfilled the American College of Rheumatology (ACR) diagnostic criteria with systemic disease activity and renal involvement that required kidney biopsy (the LN group). Patients were excluded if they had life-threatening complications such as cerebral lupus or severe infection, needed dosage augmentation of steroid within the previous 3 months, had a history of poor compliance with drug regimens, or were pregnant. We recruited 25 healthy volunteers as the control group. In addition, we recruited 13 patients with biopsy-proved hypertensive nephrosclerosis (HTN group) to determine whether any alteration in urinary mRNA level represents the result of lupus nephritis or nonspecific change attributable to renal fibrosis. After informed consent, a whole-stream early morning urine specimen was collected immediately before kidney biopsy for mRNA extraction and determination of cytokine gene expression.
Preparation of mRNA
The methods of urinary sediment isolation and mRNA extraction have been described by Li, et al14. Briefly, urine samples were centrifuged at 3500 g for 30 min at 4°C and total RNA was extracted by the RNeasy Mini Kit (Qiagen Inc.). RNA was extracted from the blood samples using the QIAamp RNA Blood Mini Kit (Qiagen Inc.). All samples were pretreated with deoxyribonuclease I (Invitrogen, Life Technologies) and then stored at −70°C.
Quantification of mRNA expression
We performed quantitative real-time PCR (qRT-PCR) by the ABI Prism 7700 Sequence Detector System (Applied Biosystems) to determine the mRNA expression. Based on available evidence5,6,7,8,9,10,11,12,13, we quantified the expression of the following: interferon regulatory factor 4 (IRF4) and PU.1 (both are Th9-related transcription factor); IL-9 and IL-10 (both are Th9-related cytokines); aryl hydrocarbon receptor (AHR; the Th22-related transcription factor); and IL-22 (Th22-related cytokine). The amount of RNA was controlled by 18S rRNA as housekeeping gene. All samples were performed in triplicate.
Disease activity and chronic damage of SLE
SLE disease activity was assessed by the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI)15, and its chronic damage by the Systemic Lupus International Collaborating Clinics/ACR Damage Index16. Renal-specific SLEDAI score was computed as described by Appenzeller, et al17. Kidney biopsy specimens were evaluated according to the International Society of Nephrology/Renal Pathology Society classification of histological type18. Histological activity index and chronicity index were determined by standard methods19. Evaluation of biopsy specimens were performed by a pathologist unaware of the clinical data and result of gene expression study.
Morphometric study of kidney biopsy
Jones’ silver staining was performed on 5-µm–thick sections of renal biopsy specimen of each patient. As previously described by others20, we used computerized image analysis method to semiquantify nephrosclerosis. Ten glomeruli and 10 randomly selected areas were assessed in each patient and the average percentage of scarred glomerular and tubulointerstitial areas, as represented by the percentage of the area with positive staining, were computed for each patient.
Intrarenal gene expression
As described21, cryosections 14 µm thick were prepared on a cryostat (Leica Microsystems) using disposable microtome blades (Leica) in RNase-free conditions. The isolated tissue was then put into a micro centrifuge cap that was filled with guanidine thiocyanate containing lysis buffer for the subsequent RNA isolation. The tissue lysate was kept at −80°C until RNA extraction was performed with the RNeasy Micro Kit, following manufacturer’s instructions. Gene expression study by qRT-PCR was then processed as described above.
Clinical followup
After the initial assessment, all patients were followed for at least 12 months. The clinical management was decided by individual nephrologist and not affected by the study. In general, patients were treated with corticosteroid, together with cyclophosphamide (CYC) or mycophenolate according to published protocols22. Therapeutic response to induction immunosuppressant was assessed at 12 weeks after treatment and classified into complete remission, partial remission, and no response as defined22. Briefly, complete remission was defined as a value for urinary protein excretion that was less than 0.3 g/g creatinine, with normal urinary sediment, a normal serum albumin concentration, and values for both serum creatinine and estimated glomerular filtration rate (GFR) that were 15% or less above the baseline values. Partial remission was defined as a value for urinary protein excretion that was between 0.3 and 2.9 g/g creatinine, with a serum albumin concentration of at least 30 g/dl and stable renal function. Treatment failure was defined as a value for urinary protein excretion that remained at or above 3 g/g creatinine or a value of 0.3 to 2.9 g/g creatinine, but with a serum albumin below 30 g/dl, an increase in the serum creatinine concentration ≥ 50 µmol/l, or a value for estimated GFR that was more than 15% above the baseline value, or the discontinuation of treatment owing to side effects.
Statistical analysis
Statistical analysis was performed by SPSS for Windows software version 18.0 (SPSS Inc.). All data are presented in mean ± SD unless otherwise specified. Because the levels of gene expression were grossly skewed in distribution, the result was compared between groups by Kruskal-Wallis test or Mann-Whitney U test as appropriate. Correlations between variables were determined by Spearman rank correlation coefficient. A p value of < 0.05 was considered statistically significant. All probabilities are 2-tailed.
RESULTS
The demographic and baseline clinical data of the patients are summarized in Table 1. All urinary specimens yielded sufficient mRNA for study. At the time of urine collection and before renal biopsy, all patients of the LN group were receiving prednisolone (at a dose 7.4 ± 4.9 mg/day); 32 patients also received azathioprine (68.8 ± 26.2 mg/day), 7 received mycophenolate (928.6 ± 450.0 mg/day), and 5 received cyclosporine (130.0 ± 75.8 mg/day). Renal biopsy of the LN showed pure mesangial disease (class II, 6 cases), pure membranous disease (class V, 24 cases), pure proliferative glomerulonephritis (class III or IV, 19 cases), and mixed proliferative and membranous disease (21 cases); 3 cases had insufficient material for histological classification. Histological activity and chronicity indices of the LN group were 4.9 ± 4.4 and 1.9 ± 2.4, respectively. Morphometric study showed that percentages of scarred glomerular and tubulointerstitial area were 14.1 ± 21.7% and 10.3 ± 19.0%, respectively.
Demographic and baseline clinical data. Values are mean ± SD unless otherwise specified.
Comparison of urinary mRNA between groups
There was no detectable IL-9 mRNA in any samples. There was no significant relationship between urinary mRNA level and baseline immunosuppressive regimen. There were significant correlations between urinary mRNA levels of IRF4 and PU.1 with that of IL-10 (r = 0.533 and r = 0.496, respectively, p < 0.0001 for both). Urinary mRNA level of IL-22 correlates with that of AHR (r = 0.295, p = 0.002), as well as with IRF4 and PU.1 (r = 0.583 and r = 0.485, respectively, p < 0.0001 for both).
Urinary sediment mRNA levels of IL-10 and IL-22 are compared between patient groups and summarized in Figure 1. In addition, there were significant differences in the urinary sediment mRNA levels of AHR and IRF4 between groups (details not shown). Compared with the HTN group, patients with lupus nephritis had significantly lower urinary sediment levels of IRF4 (0.9 ± 3.7 vs 1.7 ± 2.3 copies, p = 0.001), but higher IL-10 (7.8 ± 18.5 vs 1.9 ± 4.0 copies, p = 0.012) and AHR (1.9 ± 3.4 vs 0.2 ± 0.2 copies, p < 0.0001).
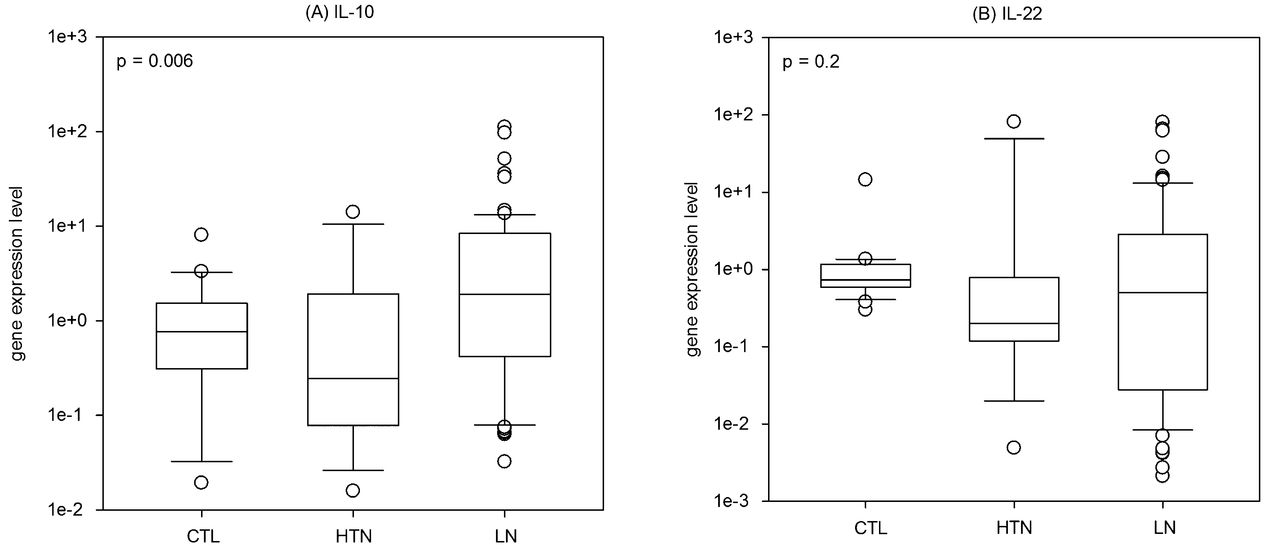
Comparison of urinary sediment mRNA levels of (A) IL-10 and (B) IL-22. Gene expression data are depicted as number of copies per 100,000 copies of housekeeping gene (18S rRNA) mRNA and compared by Kruskal-Wallis test. IL-10: interleukin 10; IL-22: interleukin 22; CTL: healthy control; HTN: hypertensive nephrosclerosis; LN: lupus nephritis.
Relation with clinical and histological variables
Among patients within lupus nephritis, the correlation between urinary mRNA expression and clinical variables was further explored. In essence, urinary mRNA levels of IL-10 correlated with the SLEDAI score (r = 0.277, p = 0.018). On the other hand, urinary mRNA levels of IL-22 had a significant inverse correlation with renal SLEDAI score (r = −0.445, p < 0.0001), and modest but significant correlation with serum estimated GFR (r = 0.270, p = 0.021) and serum complement factor 4 levels (r = 0.321, p = 0.006), but not the degree of proteinuria. None of the clinical variables correlated with the urinary mRNA levels of IRF4, PU.1, or AHR (details not shown).
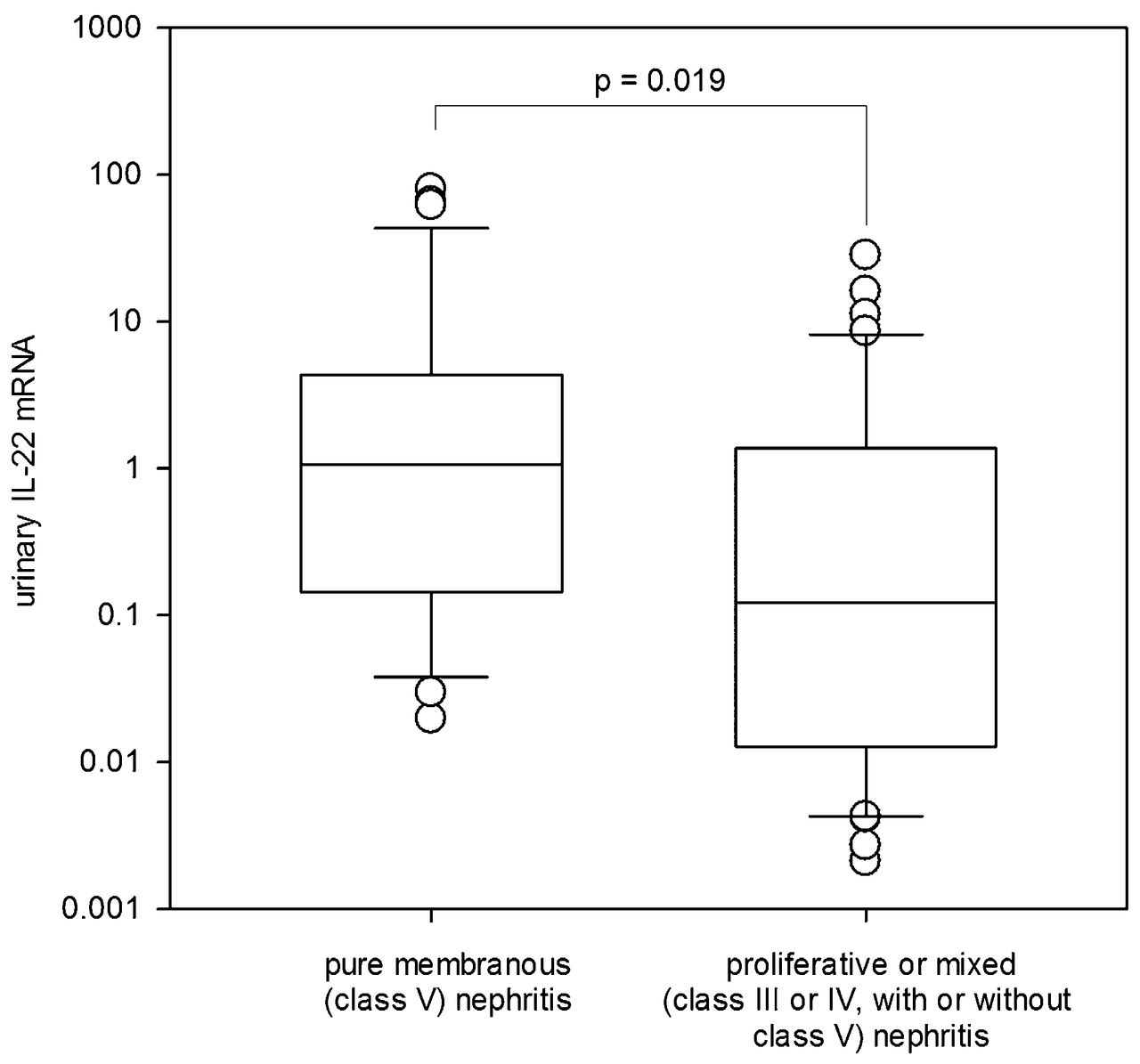
Correlations between urinary mRNA expression and histological variable were further explored. Patients with proliferative or mixed lupus nephritis (class III or IV, with or without class V) had a significantly lower urinary IL-22 mRNA level than those with pure membranous (class V) nephritis (2.2 ± 5.4 vs 8.6 ± 20.0 copies, p = 0.019; Figure 2). On the other hand, urinary mRNA levels of IL-10, IRF4, PU.1, and AHR were similar between patients with proliferative or mixed and pure membranous nephritis (details not shown). Further, urinary IL-22 mRNA level inversely correlated with the histological activity index (r = −0.427, p < 0.0001), but only marginally with chronicity index (r = 0.219, p = 0.063), and not with the degree of glomerulosclerosis or tubulointerstitial scarring. None of the pathological variables correlated with the urinary mRNA levels of IL-10, IRF4, PU.1, or AHR (details not shown). Because the number of patients with class II nephritis was small, subgroup analysis was performed for them.

Relationship between urinary mRNA level of IL-22 with histological pattern of lupus nephritis. Gene expression data are depicted as number of copies per 100,000 copies of housekeeping gene (18S rRNA) mRNA and compared by Spearman rank correlation coefficient or Mann-Whitney U test. IL-22: interleukin 22.
Relation with intrarenal gene expression
The relationship between urinary and intrarenal mRNA levels was explored after excluding 3 patients who had insufficient tissue for assessment. In short, there was a modest but statistically significant correlation between urinary and intrarenal mRNA levels of IL-10 (r = 0.337, p = 0.004). On the other hand, there was no correlation between urinary and intrarenal mRNA levels of IL-22, IRF4, PU.1, or AHR (details not shown).
Relation with treatment response
After renal biopsy, all patients received moderate to high-dose prednisolone (28.5 ± 7.0 mg/day); 33 patients also received mycophenolate (1500 ± 484 mg/day), 6 received monthly intravenous CYC, 6 received oral CYC (91.7 ± 20.1 mg/day), and 5 received cyclosporine (160.0 ± 89.4 mg/day). After 12 weeks of induction treatment, 38 patients (56.3%) had complete remission, 24 (35.9%) had partial remission, and 5 (7.8%) showed no response. Therapeutic response was not determined in 6 patients because of inactive class II disease. There was no difference in treatment response between treatment regimens (details not shown).
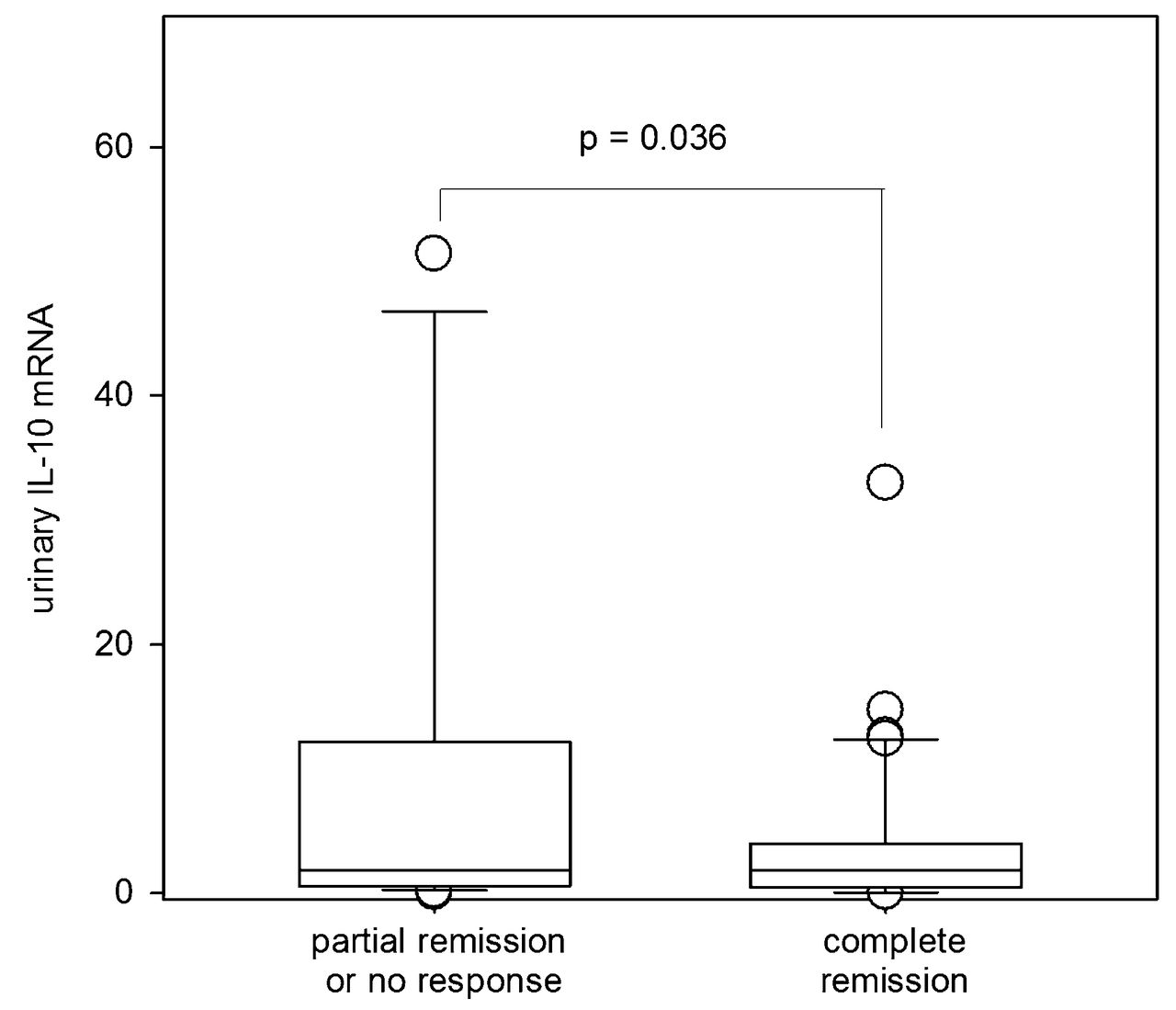
There was a significant difference in urinary IL-10 levels between patients with different therapeutic responses (Figure 3). Urinary mRNA level of IL-10 was modestly but significantly lower among patients who achieved complete remission than among those with partial remission or no response (4.1 ± 6.5 vs 14.1 ± 28.0 copies, p = 0.036). Similarly, intrarenal mRNA level of IL-10 was significantly lower among patients who achieved complete remission than among those with partial remission or no response (2.8 ± 3.7 vs 4.5 ± 6.1 copies, p = 0.027). There was no relationship between therapeutic response and urinary or intrarenal mRNA levels of IL-22, IRF4, PU.1, or AHR (details not shown). Neither urinary nor intrarenal IL-10 mRNA levels correlated with the baseline renal SLEDAI, histological class of nephritis, or activity index, and were considered unlikely to be confounding factors that may account for the relationship between IL-10 and treatment response.

{kind=link}
{kind=link}
{kind=link}
Comparison of urinary sediment mRNA levels of IL-10 between treatment response groups. Gene expression data are depicted as number of copies per 100,000 copies of housekeeping gene (18S rRNA) mRNA and compared by Mann-Whitney U test. IL-10: interleukin 10.
DISCUSSION
In our present study, we studied urinary mRNA levels of cytokines and transcription factors related to Th9 and Th22 pathways in patients with lupus nephritis. We found that urinary mRNA level of AHR (the transcription factor of Th22 pathway) is decreased in lupus nephritis, and urinary IL-22 mRNA level correlates positively with renal function, negatively with the histological activity index, and is decreased in patients with proliferative lupus nephritis as compared with nonproliferative disease. On the other hand, urinary mRNA levels of IRF4 (the transcription factor of Th9 pathway) and IL-10 are elevated in lupus nephritis. Urinary IL-10 mRNA level correlates with its intrarenal mRNA level as well as systemic, but not renal, disease activity. Moreover, urinary and intrarenal IL-10 mRNA levels are significantly higher among patients who had partial remission or no response to treatment as compared with those who achieved complete remission.
In short, our study showed that the Th22 pathway cytokines inversely correlate with the severity of renal inflammation, but not chronic damage. Our finding is consistent with published reports. For example, 2 previous studies showed that serum IL-22 concentration is decreased in the patients with active lupus11,12,23, and treatment with recombinant IL-22 could alleviate tissue destruction during inflammatory responses13. However, it is important to note that the Th22 pathway may not be entirely protective in SLE because studies suggest that Th22 might be a good index to predict the tissue involvement of SLE, with increased Th22 cells in patients with pure SLE skin disease and decreased Th22 cells in those with lupus nephritis24. Because we only recruited patients with SLE with active nephritis, further studies would be needed to determine the change in urinary mRNA expression of Th22-related cytokines in patients with SLE with pure extrarenal manifestations.
We found that IL-9 mRNA is undetectable in the urine and renal tissue of all patients. Our findings may seem to contradict with the previous report by Ouyang, et al10 that found that plasma concentrations and mRNA levels of IL-9 were significantly elevated in patients with SLE compared with healthy controls. Although the Th9 pathway has been found to take part in the development of regulatory T cells and the pathogenesis of autoimmune diseases such as experimental allergic encephalitis25, published data on lupus nephritis are scarce. To date, there is no concluding evidence that IL-9 contributes to the pathogenesis of SLE26.
In our present study, IL-10 mRNA is readily detectable in both urinary sediment and renal biopsy specimen. Theoretically, IL-10 could originate from either regulatory T (Treg) cells or Th9 cells8. Because we did not find IL-9 mRNA, it seems most likely that the IL-10 mRNA we detected came from Treg. The observation is consistent with our previous studies27,28 that showed that urinary mRNA level of FOXP3, the key transcription factor of Treg, was significantly elevated in patients with active lupus nephritis, urinary mRNA level of IL-10 decreases progressively after immunosuppressive treatment28, and urinary FOXP3 mRNA in patients with no response to therapy was higher than those with satisfactory treatment response. Taken together, this series of studies suggests that urinary mRNA levels of the Treg pathway (i.e., FOXP3 and IL-10) indicates active but readily reversible lupus nephritis.
The correlation we observed between urinary and intrarenal IL-10 mRNA supports the hypothesis that urinary IL-10 mRNA comes from T cells infiltrating the kidney (which could be either regulatory or pathogenic-activated T cells) and being leaked into the urine. We have previously reported that CD3+ (i.e., T cells) and CD20+ cells (i.e., B cells) were the major components of urinary mononuclear cells in patients with SLE and their number correlates with SLE disease activity29. Unfortunately, because of the limitations in our original research design, we could not perform in situ hybridization or immunohistochemistry study on intrarenal IL-10 mRNA and correlate that with the urinary result.
On the other hand, we did not find any significant correlation between urinary and intrarenal mRNA levels of IL-22, IRF4, PU.1, or AHR, for reasons not immediately clear. It is possible that inflammatory cells that detach into the urine are intrinsically different from those tightly bound to kidney tissue. On the other hand, the small kidney tissue we used for intrarenal mRNA study has a substantial sampling error. In theory, the mRNA we detect in urine may originate from passenger lymphocytes of the systemic circulation, but that seems unlikely.
There are several limitations of our present study that need to be addressed. First, we have not determined the cellular origin of the mRNA in the urine. Our previous study showed that CD3+ and CD20+ cells were the major components of urinary mononuclear cells in patients with SLE29, while Th9-and Th22-related cytokines are not produced by non-lymphoid cells. Therefore, it seems likely that most of the urinary sediment mRNA detected in our present study originate from T cells, although IL-22 is also produced by innate immune cells (for example, natural killer cells). Flow cytometry study would be necessary to confirm the cellular origin of mRNA detected in urinary sediment. In our study, we did not have the corresponding serum level of our patients for comparison, and it would be interesting to see whether serum IL-10 or IL-22 levels could provide additional prognostic information.
Second, the number of healthy controls was small, so that the result may be difficult for analysis. For the LN group, the distribution of histological class is somewhat different from other series, but similar to our previous report30 with the number of pure class V and mixed nephritis very high as compared with pure proliferative. The response rate to treatment in our series may appear high, but is similar to previous reports from our locality22,31. Moreover, the treatment protocol of our patients was heterogeneous. There are numerous confounding factors that could influence response to therapy and our result should be interpreted with caution, and our study does not have the sufficient statistical power to allow detailed subgroup analysis according to the type of treatment or histological feature.
As mentioned above, we did not include a group of patients with SLE with active disease but no renal involvement, or patients with other types of glomerulonephritis. As a result, we could not conclude beyond doubt that the observed change in urinary mRNA level is specific to lupus nephritis. Although our previous study showed that urinary mRNA level of IL-10 decreases progressively after immunosuppressive treatment28, we have no data on the longitudinal change in urinary mRNA level of Th9- or Th22-related genes in patients with SLE with quiescent disease. It would be interesting to see whether serial monitoring of urinary gene expression would predict disease flare. Although clinical response is usually assessed at 6 months, we deliberately determined the therapeutic response at 3 months in our study because our aim was to identify predictors of slow responders so that early consideration of change in treatment regimen was possible. In addition, it is possible that using urinary albumin-to-creatinine ratio may be more reliable than 24-h urine protein level, although our previous study showed that the 2 variables were closely correlated32.
We found that urinary IL-22 mRNA level is decreased in patients with SLE with proliferative nephritis. On the other hand, urinary mRNA levels of IL-10 correlates with its intrarenal mRNA level as well as systemic disease activity. Moreover, urinary and intrarenal IL-10 mRNA levels may predict response to immunosuppressive therapy. These preliminary results suggest urinary mRNA levels of IL-10 and IL-22 might be used as biomarkers for assessing disease activity and risk stratification in lupus nephritis. Future studies are needed to define their role in clinical practice.
Footnotes
Supported by the Chinese University of Hong Kong (CUHK) research account 6901031.
- Accepted for publication March 25, 2015.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.