
Abstract
Objective. To develop a personalized treatment target approach in patients with rheumatoid arthritis (RA) based on baseline risk factors for joint damage progression in combination with disease activity over time.
Methods. Data were used from the Nijmegen early RA cohort. Presence or absence of anticyclic citrullinated peptide antibodies (anti-CCP), high erythrocyte sedimentation rate, and erosions were translated into 4 risk profiles: 0, 1, 2, and 3. Joint damage progression was assessed with the Ratingen score, and disease activity with the original Disease Activity Score (DAS) over 3 years. The probability for joint damage progression was calculated for each risk profile and each DAS category using logistic regression models. The probabilities were translated into personalized disease activity treatment targets.
Results. More risk factors at baseline as well as a higher DAS level resulted in a higher probability for joint damage progression in a dose-dependent way. Low DAS corresponded with a probability of 0.0, 0.08, 0.20, and 0.58 in patients with 0, 1, 2, and 3 risk factors, respectively. Moderate DAS corresponded with a probability of 0.06 in patients with 0 risk factors and 0.35 with 1 risk factor. High DAS resulted in a probability of 0.50 with no risk factors present at baseline.
Conclusion. Presence of anti-CCP, acute-phase response, and erosions at baseline can be used to set individual treatment targets in RA. In patients without these risk factors, a moderate DAS as a target is sufficient, while for patients with all 3 risk factors, a low DAS is not strict enough to limit the risk for joint damage.
- RHEUMATOID ARTHRITIS
- DISEASE ACTIVITY
- JOINT EROSIONS
- ACUTE-PHASE REACTION
- ANTICYCLIC CITRULLINATED ANTIBODIES
The treat-to-target approach in the treatment of rheumatoid arthritis (RA) has been shown to be beneficial in clinical trials, as well as in clinical practice1,2,3,4. Remission or low disease activity is commonly used as the target in a treat-to-target approach because generally, more disease activity leads to more joint damage progression, especially in the first 3 years of the disease5. The exact treatment target differs in studies and between guidelines3,6,7. However, patient characteristics are not commonly taken into account: a 1-size-fits-all treatment target such as the Disease Activity Score (DAS) < 1.6 or DAS at 28 joints (DAS28) < 2.6 is used for all patients with RA. Although drug-free remission is the ultimate treatment target for all patients, this is infrequently reached8.
The relationship between disease activity and joint damage progression is strongly modified by the presence of rheumatoid factor (RF) and anticyclic citrullinated peptide antibodies (anti-CCP)9,10. There is evidence that anti-CCP–positive patients with RA have joint damage progression at lower levels of disease activity than anti-CCP–negative patients10. This idea is in line with observations by many rheumatologists in clinical practice. Consequently, it can be conceived that if the aim is to prevent joint damage progression, the treatment target can be personalized using baseline risk factors. Then, not all synovitis needs to be repressed in patients with a low risk for joint damage progression while for patients with a high risk for joint damage progression, no residual synovitis can be accepted.
Another reason for the personalization of treatment targets is that the Patient Acceptable Symptom State is often at the level of low or moderate disease activity11,12. At the same time, guidelines prescribe remission as the ultimate goal in all patients with RA and current treatment targets do not regard these individual patient preferences6,7. If a patient is satisfied with a certain level of inflammation and the rheumatologist could reliably estimate that the risk for joint damage progression is limited, there probably is no good reason to strive for remission for that individual patient at all costs. It is desirable to take a step toward personalized medicine and differentiate from the 1-size-fits-all treatment target based on the individual risk for joint damage progression and patient preferences. It should be clear that with the progress in effective and affordable treatment options, treatment targets should and will shift in the future.
Several prognostic models have been developed to estimate the individual risk for joint damage progression13,14,15,16,17. These models agree in the importance of 3 baseline factors for predicting worse prognosis regarding joint damage progression: presence of anti-CCP, high level of erythrocyte sedimentation rate (ESR), and presence of erosions. The matrix models seem to be especially practical for use in daily practice18,19,20,21. However, none of these matrix models are currently widely used in daily practice. A reason might be that the models are based on baseline factors and that the most important dynamic prognostic factor, disease activity over time, is not included in these models. Therefore, the objectives of our study were to combine baseline risk factors with disease activity over time and to show how this combination can be used to derive personalized treatment targets for disease activity in RA with the scope to prevent joint damage progression in the first 3 years of disease.
MATERIALS AND METHODS
Design
Data were extracted from the Nijmegen early RA cohort of the Radboud University Medical Centre in Nijmegen, the Netherlands. In this old cohort that started in 1985, patients were not as intensively treated as currently. Patients included before December 2008 were part of our study; data of the first 3 years of the disease were used22. All patients provided written informed consent to be included in the cohort. No additional formal approval of a medical ethics committee had to be obtained because it was not required in the Netherlands for this type of observational study.
Patients
Patients were consecutively included in the early RA cohort if they fulfilled the 1987 American College of Rheumatology criteria for RA, had a disease duration of less than 1 year, had no prior use of disease-modifying antirheumatic drugs (DMARD), and were aged 18 years or older. Cohort patients were included for the current analyses if the radiographs of hands and feet were available at baseline and at 2-year or 3-year followups, and if patients had at least 4 visits with an assessment on the original DAS23. The maximum accepted interval between 2 visits was 1 year. Patients treated with biological DMARD during the first 3 years were excluded from our current study because this type of medication changed the relationship between disease activity and joint damage24,25.
Assessments
Demographics, smoking status, shared epitope (SE), and disease activity were assessed. Disease activity was assessed at baseline and every 3 months, including swollen joint count (SJC) at 44 joints, tender joint count (TJC) at 53 joints, Ritchie Articular Index, ESR, and general health on a visual analog scale (VAS GH), so that the original DAS could be calculated23. In the analyses, instead of the mean DAS, the 80th percentile of the DAS between 6 and 36 months for each individual patient was used. This meant that after the initial decrease of the DAS in the first 6 months of treatment, 80% of the DAS of an individual patient was at or below this level between 6 and 36 months. Sensitivity analyses were done with the median and maximum DAS. DAS were classified according to the known DAS cutpoints: low DAS (< 2.4), moderate DAS (2.4–3.7), and high DAS (> 3.7).
Radiographs of the hands and feet were taken at baseline and at the 1-, 2-, and 3-year followups. Radiographs at baseline and the 3-year followup were scored according to the Ratingen erosion score26. This was a modification of the Larsen score, evaluating the percentage of joint surface destruction, graded from 0 to 5 (range 0–190). Progression of joint damage was defined as a difference of > 5 Ratingen points. This was based on the smallest detectable change in our cohort, as previously calculated27. A subset of radiographs had been read in 2002 by 4 raters (ICC 0.85). For our study, radiographs from 2002 up to 2011 were read by 2 raters (ICC 0.95).
Baseline risk factors
A baseline prediction model for joint damage progression between 0 and 36 months was previously developed28. In this model, anti-CCP, RF, SE, SJC at 28 joints, TJC at 28 joints, ESR, VAS pain, VAS general health, erosions at baseline, and smoking status were included as possible predictors for joint damage. A multivariable model using backward selection showed that anti-CCP, ESR, and erosions at baseline were strongly and significantly associated with joint damage progression. An extended model with categorization of these 3 factors was compared to a simplified model in which the 3 prediction factors were dichotomized. The cutpoints chosen in the simplified model were anti-CCP > 25 U/l (ELISA immunoscan RA Mark 2, Euro Diagnostica) and > 10 U/l for the posthoc evaluated samples (with fluoro enzyme immunoassay, EliA-CCP, Thermo Scientific). ESR > 25 mm/h was considered high (60 min Westergren mode, StaRRsed Compact InteRRliner V8, Mechatronics), and for the presence of erosions at baseline, the cutpoint was ≥ 1 Ratingen point. Both the extended model and the simplified model had moderate to good discriminative ability (area under the receiver-operation characteristic curve 0.77 and 0.75, respectively) and adequate calibration. Because the simplified model was more user-friendly for daily practice, we used the simplified model. Four risk profiles were defined based on the presence or absence of the 3 main baseline risk factors for joint damage progression in the simplified baseline model. The 3 risk factors were anti-CCP positivity, high ESR, and the presence of erosions. The risk groups (0, 1, 2, and 3) represented the number of risk factors present in the individual patient.
Analyses
Patient characteristics at baseline and followup were evaluated separately for the 4 risk groups. Differences between the groups were analyzed with the 1-way ANOVA, chi-square test, and Kruskal-Wallis test, as appropriate. The difference in joint damage progression between the risk groups was analyzed in 2 ways, i.e., the probability for progression and the amount of progression between 0 and 36 months. Next, patients were categorized by the number of baseline risk factors and the level of the DAS over time (80th percentile): low (< 2.4), moderate (2.4–3.7), and high (> 3.7). The probability for joint damage progression was analyzed for each category of disease activity and for all 4 risk groups separately using logistic regression models. Finally, the probabilities for joint damage progression were translated into the DAS treatment targets for each risk profile with the aim to limit the risk for joint damage progression.
Missing values analysis of the DAS variables was performed by evaluating the frequencies and patterns of missing variables using SPSS (IBM SPSS) missing value analysis. Missing values showed no recognizable pattern and were considered missing at random. Missing visits were interpolated by calculating the average DAS of the closest visits before and after the missing DAS, taking into account the distance to the previous and following visit with a maximum of 6 months. The number of DAS was completed to 11 for each patient. Missing Ratingen scores at 3 years followup were imputed according to the last observation carried forward principle, with the limitation that the radiograph was taken between 24 and 36 months’ followup. SPSS version 20.0 was used for all analyses.
RESULTS
Until December 2008, 607 patients were included in the cohort; 435 of the cohort patients (72%) had available radiographs at 0 and 3 years. There were 362 patients (60%) who had at least 4 visits with a maximum interval of 1 year. At all visits, the DAS28 was assessed, but the DAS was assessed in only 320 patients (53%), which was needed for the analyses. Anti-CCP and ESR at baseline were available for 269 of the cohort patients (44%). Nine patients were treated with biologic DMARD in the first 3 years of the disease and were excluded, so that finally 260 patients (43%) could be included for analyses. Cohort patients that were excluded from the study did not differ significantly or relevantly from the patients included in our study (not shown). The median number of visits was 9.5 (interquartile range 8–11) and 29% of the DAS scores were imputed. Twelve percent of the 260 patients (31) had 0 risk factors, 30% (79) had 1 risk factor (40 anti-CCP, 26 ESR, 13 erosions), 33% (86) had 2 risk factors (43 anti-CCP and ESR, 27 anti-CCP and erosions, 16 ESR and erosions), and 25% of the patients (64) had all 3 risk factors.
With an accumulation of risk factors, patients were more often positive for RF and SE. The DAS and SJC at baseline were also significantly higher in patients with an accumulation of risk factors (Table 1). The percentage of patients with joint damage progression between 0 and 36 months was 10% in patients with 0 risk factors, 25% in patients with 1 risk factor, 58% in patients with 2 risk factors, and 80% in patients with 3 risk factors (p < 0.001; Figure 1A). The amount of progression between 0 and 36 months was also increasing, with an increasing number of risk factors present at baseline (Figure 1B; p < 0.001).

Joint damage progression by number of risk factors. A. No. patients with and without joint damage progression between 0 and 36 months, with Ratingen ≥ 5 points as cutpoint. B. Cumulative probability plot of joint damage progression by number of risk factors (Ratingen score).
Baseline of patients in the study population by number of risk factors. Variables are presented as % (n), mean (SD), or median (IQR).
Patients in the cohort were treated with synthetic DMARD therapy: 83% received DMARD monotherapy and 13% received combination therapy [of which 68% were treated with methotrexate (MTX) and sulfasalazine (SSZ), 18% with SSZ and hydroxychloroquine, and 14% with other combinations]. Forty percent of patients received MTX with 10 mg (3.8) as the mean dose (SD), and 19% of the study population used oral prednisone. Within the 19%, 8% (21) used ≥ 15 mg daily during the first 3 years of disease. Treatment changed over time. None of the patients were treated with biologic DMARD because that was an exclusion criterion. There were only small differences in treatment between the 4 different risk profiles (Table 2).
Medication use of the study population by number of risk factors. Use of synthetic DMARD and maximum dose of prednisone in the study population between 0 and 36 months is given as percentage (number of patients).
The probability for joint damage progression increased with an increasing DAS level and also with an increasing number of risk factors. This is depicted in the margins of Figure 2. Thus, at the same DAS level, patients had a higher probability for joint damage progression when more baseline risk factors were present (Figure 2). Low DAS or lower during 80% of the time in the first 3 years of disease corresponded with a probability of 0.0 in patients with 0 risk factors, a probability of 0.08 in patients with 1 risk factor, 0.20 when 2 risk factors were present, and 0.58 when 3 risk factors were present. Similarly, a higher probability was seen with an increasing number of risk factors in moderate and high DAS categories.

Probability for joint damage progression by number of risk factors and different levels of DAS between 6 and 36 months. The risk factors are anti-CCP positivity, ESR > 25 mm/h, and ≥ 1 erosion at baseline. Low DAS < 2.4, moderate DAS 2.4–3.7, high DAS > 3.7. DAS: Disease Activity Score; anti-CCP: anticyclic citrullinated peptide antibodies; ESR: erythrocyte sedimentation rate.
The predicted probabilities for joint damage progression for each risk profile and DAS category were translated into personalized treatment targets. A cutpoint of the risk for joint damage progression was arbitrarily set at 0.20, which was considered acceptable for now. For patients with 0 risk factors, this meant that moderate DAS should be strict enough as a treatment target. Patients with 1 or 2 risk factors should reach low disease activity, and for patients with 3 risk factors, low DAS is not strict enough and stricter targets should be achieved.
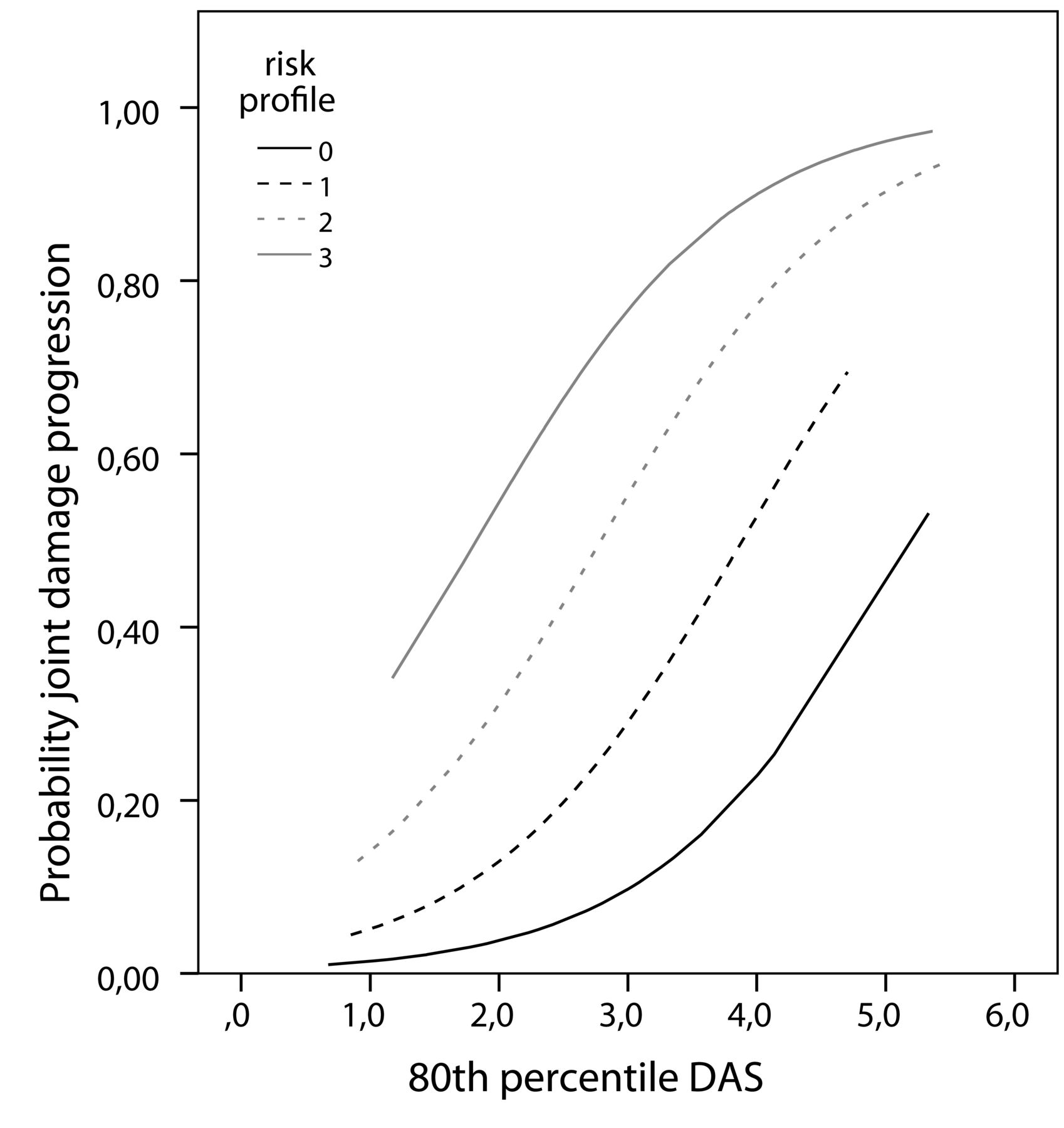
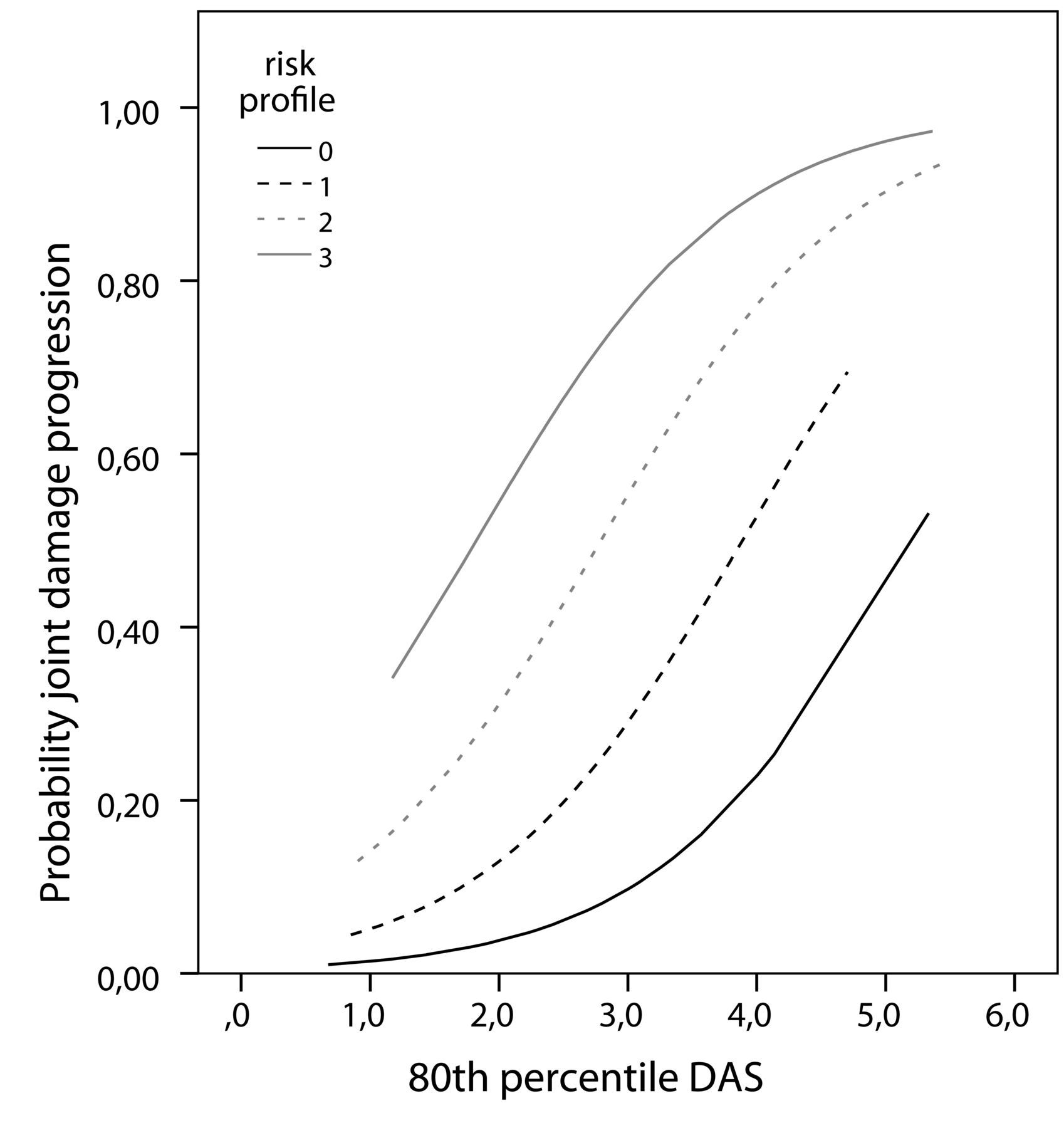
In Figure 3, the relationship between the DAS level over time and the risk for joint damage progression is shown for the 4 risk groups. This shows that the differentiation of treatment targets for patients with a different number of baseline risk factors was also true for cutpoints higher or lower than 0.20. Sensitivity analyses with the median and maximum DAS instead of the 80th percentile showed a similar gradient of probabilities, but resulted in different treatment targets.
{kind=link}
{kind=link}
{kind=link}
Probability curves for joint damage progression for 4 risk factor groups with 0, 1, 2, or 3 risk factors at baseline. DAS: Disease Activity Score.
DISCUSSION
Complete absence of symptoms, preferably without medication, is the ultimate goal in the treatment of RA. The treatment target in the starting phase of RA is, therefore, DAS remission. However, sustained remission is usually hard to achieve with the treatment options currently available8. According to the results of our study, remission is not needed in all patients with RA from the viewpoint of preventing joint damage progression.
An increasing level of the DAS over time, and an increasing number of risk factors at baseline, were associated with a higher probability for joint damage progression after 3 years. Patients with more risk factors had a higher probability for joint damage progression at the same DAS level over time. In subgroups of patients with 0 risk factors for joint damage progression, the treatment target can be adapted to moderate disease activity while the chance of developing joint damage progression is quite low. For patients with 1 or 2 risk factors, a more stringent target should be aimed for and low DAS should be achieved as soon as possible. In the majority of patients with 3 risk factors, low disease activity is not strict enough to prevent joint damage progression.
The clinical implication of our study is that not all patients need to achieve clinical remission to avoid joint damage progression. In a personalized treatment target, the prognostic profile of the individual patient is taken into account. The treatment target and the need for therapy change should be subjects of discussion between rheumatologist and patient. This might bridge the gap between the patient acceptable symptom state, which is often at the level of moderate DAS, and the guidelines that advise DAS remission, also in patients with a low risk for unfavorable prognosis11. In other cases, individual estimation of the prognosis might convince the rheumatologist of the importance to firmly suppress disease activity because underappreciation of the risk and outdated treatment still lead to poor outcomes4.
The importance of measuring and using anti-CCP, ESR, and erosions at baseline was confirmed in our study, not only for the prognosis at baseline, but also when setting an individual treatment target. The same was true for the association between the DAS and joint damage progression. Two important steps were made in our study to support the application of this knowledge in clinical practice: (1) the use of a simplified baseline prediction model, and (2) the translation to personalized treatment targets based on the probability for joint damage progression. Personalized medicine in RA focuses on optimal pharmacotherapy algorithms and predictors for response and side effects29. We showed that the personalized approach can also be used when setting a personalized treatment target.
In current daily practice, rheumatologists often accept low or moderate disease activity in an individual patient with few symptoms, especially when radiographs or ultrasounds show neither erosions nor power Doppler activity. The results of our study confirm this practical way of dealing with the current guidelines. Moreover, this approach opens up the possibility of quantifying the risks of joint damage progression, extending beyond the experience of individual rheumatologists.
The aim of our study was to show a practical way of personalized medicine. Several steps need to be taken before definitive treatment targets for clinical practice can be defined. The simplified baseline prediction model needs to be externally validated, and the equal importance that was given to anti-CCP, ESR, and erosions at baseline should be checked in another population. Because treatment influences the relationship between disease activity and joint damage progression, treatment targets might differ between patients receiving DMARD therapy and patients receiving biologic therapy. This should be considered in a validation study by stratification of the treatment given. In the future, other promising prognostic factors may be added for refinement of the model, such as the ultrasound of an index joint30. Also, the category DAS < 2.4 could be divided into remission and low disease activity. Because of the small study population, this was not possible in our study. Studies about the importance of inflammation of the foot joints for the prediction of joint damage progression and defining remission have contradictory results. We therefore chose to use the full DAS in this prediction model and not the more frequently used DAS2831,32. Application of this principle to the DAS28 and other indices of disease activity used for treat-to-target is a logical next step.
Progression of joint damage was the only outcome measure considered in our study because this is currently the focus of treatment. However, other consequences of RA, such as functional disability and extraarticular features such as lymphomas or atherosclerosis, are important when defining treatment targets. The treatment target for prevention of cardiovascular diseases may differ from the target for prevention of joint damage33. This should be taken into account when defining clinical treatment targets. Also, the patient’s comfort and fatigue levels should be considered.
We used the Ratingen score for evaluation of radiographs and not the modified Sharp score. This could be seen as a limitation of our study. The main differences between these 2 scores are that in the Ratingen score, the percentage of eroded joint surface is evaluated instead of the number of erosions, and joint space narrowing (JSN) is not evaluated. However, Ratingen score and modified Sharp are closely correlated because the same joints are evaluated and because of the relative weight that is given to erosions versus JSN in the Sharp van der Heijde score34,35,36,37.
Ideally, prognostic models are developed in patients who are untreated, i.e., following the natural course of disease. The advantage of an older cohort that is less intensively treated is that it resembles the natural course of RA as closely as possible, and is more sensitive for differences between the risk groups. The risk for and amount of joint damage progression in more recently diagnosed patients with RA are expected to be lower because of earlier diagnosis, better treatment, and possibly a milder disease course38,39. Therefore, the generalizability of the results to more recent cohorts is limited. It is, however, expected that the gradient of probability with more risk factors and at higher levels of disease activity will still be there. A limitation of the older cohort and the observational study design is that treatment was not randomized in the 4 risk groups. Patients treated with biologics were excluded in our analyses. These patients probably had a worse prognosis. Because it concerns only 9 patients, this exclusion criterion did not influence the results of the analyses.
The 80th percentile of the DAS was used in the analyses, representing the DAS over time between 6 and 36 months. The purpose of a target is that most observations should be below target. The maximum DAS could overestimate the level of disease activity in an individual patient. The median DAS does not reflect a treatment target because half of the observations are above the median. Sensitivity analyses with the median and maximum DAS showed a similar gradient of probabilities for joint damage progression when more baseline risk factors were present and at higher levels of the DAS, but resulted in different treatment targets because of other probabilities.
In RA, personalized treatment targets can be defined based on the combination of baseline risk factors and disease activity over time. Presence of persistent disease activity with 1 or more risk factors is an indication to treat toward a more intensive target. In further research, the concept and treatment targets should be validated and other outcomes, such as cardiovascular risk and function, should be studied. This should be the basis for a personalized treat-to-target approach in RA.
Acknowledgment
We thank all research nurses and rheumatologists for their participation and contribution in data collection, and Thea van Gaalen, Lia Schalkwijk, Carien Versteegden, Erik Brummelkamp, and Marjon de Lange-Brand for data processing. Further, we thank Maarten Boers for his suggestion regarding Figure 2.
- Accepted for publication October 31, 2014.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.