
Abstract
Objective. To evaluate the expression of interleukin 33 (IL-33) and its receptor in sera and salivary tissues of patients with primary Sjögren syndrome (pSS), and to investigate the association with clinical profiles.
Methods. Serum IL-33 and soluble ST2 (sST2) of 55 patients with pSS and 48 controls were determined by ELISA and assessed for clinical correlation. The expression of IL-33/ST2 in salivary tissues was investigated by immunohistochemical staining and was further characterized by confocal microscopy. We also measured IL-33 production in salivary glandular epithelial cells by proinflammatory stimuli.
Results. Serum levels of IL-33 and sST2 were higher in patients with pSS compared to those in controls (p = 0.018 and p < 0.0001, respectively). Among patients with pSS, sST2 concentration was associated with thrombocytopenia (p = 0.029) and correlated with disease duration (p = 0.013) and the European League Against Rheumatism Sjögren Syndrome Disease Activity Index (p = 0.042). The expression of IL-33 and ST2 was elevated in salivary glands of patients with pSS with grade 2 inflammation, and diminished in advanced inflammation. In patients with pSS, IL-33 was mainly observed in epithelial and endothelial cells of glandular tissue. The production of IL-33 mRNA by salivary gland epithelial cell line increased under stimulation with interferon-γ.
Conclusion. The expression of IL-33 and its receptor was elevated in sera and salivary tissues of patients with pSS. These results suggest that the IL-33/ST2 axis might have a role in the pathogenesis of pSS.
- SJÖGREN SYNDROME
- INTERLEUKIN 33
- ST2
Interleukin 33 (IL-33) is a recently discovered molecule that belongs to the IL-1 cytokine family1. It is a ligand of ST2, which is an orphan receptor. IL-33 binds the 2 different isoforms of ST2: ST2L, a membrane-bound form that activates the intracellular signaling pathway, and soluble ST2 (sST2), a soluble form that blocks IL-33 signaling by acting as a decoy receptor. These isoforms are generated by alternative splicing of ST2 mRNA2.
IL-33 expression is constitutive in the nucleus of endothelial and epithelial cells3,4, but is also induced in inflamed tissues5,6,7. Recent studies have clarified the dual functions of IL-33 as a nuclear factor and as an extracellular cytokine8. As a traditional cytokine, the biological effect of IL-33 is initiated by binding with ST2L expressed on hematopoietic and many other cells9,10,11.
Because of the diffuse distribution of IL-33 and ST2 in many tissues and organs, the role of IL-33/ST2 signaling has been investigated in various diseases. IL-33 exacerbates allergy, but attenuates atherosclerosis and protects against helminth infection9,10,11. Emerging evidence also indicates that the IL-33/ST2 pathway is involved in the pathophysiology of autoimmune disorders. The levels of IL-33 and sST2 are consistently elevated in rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), systemic sclerosis, and inflammatory myositis12,13,14. Further, IL-33/sST2 concentration is correlated with disease activity, raising the possibility of a potential biomarker12,13,14,15,16. The pathophysiological role of IL-33 has been demonstrated experimentally by the enhancement or elimination of IL-33/ST2 signaling in animal arthritis models17,18.
Primary Sjögren syndrome (pSS), one of the prototypic autoimmune disorders, is characterized by lymphocytic infiltration of the exocrine glands, which causes dry eyes and dry mouths19. It can occur alone or in association with other rheumatologic diseases, including RA and SLE. Although recent advances have provided a better understanding of pSS pathogenesis, much remains to be elucidated. As in other rheumatologic diseases, involvement of proinflammatory cytokines is considered important in the development and progression of glandular inflammation20,21.
In an attempt to identify the role of IL-33/ST2 in the pathogenesis of pSS, we investigated the expression of IL-33 and ST2 in sera and salivary tissues from patients with pSS, and compared the serum levels of IL-33/sST2 based on clinical manifestations. In addition, we observed stimulated production of IL-33 by salivary glandular epithelial cells in the presence of proinflammatory cytokines.
MATERIALS AND METHODS
Patients and materials
Fifty-five patients with pSS and 48 age- and sex-matched healthy controls were recruited from the outpatient clinic at the Department of Rheumatology, Seoul St. Mary’s Hospital, Seoul, Korea. All patients with pSS fulfilled the classification criteria proposed by the American-European Consensus Group22 without evidence of other autoimmune diseases. A salivary gland biopsy was performed in 25 patients with sicca symptoms for diagnostic purposes after written informed consent was obtained. Among these patients, 20 were ultimately diagnosed with pSS by positive diagnostic test results. Salivary tissues of the remaining patients who did not satisfy the serological or pathological criteria were defined as controls. Sectioned slides of salivary tissue were examined for the presence of lymphocytic infiltration and/or foci by 3 observers using Chisholm grading standard23. The focus score was defined as the number of lymphocytic foci per 4 mm2 of glandular tissue.
Human head and neck squamous cell carcinoma A253 cells (ATCC) were used for the salivary gland cell line. A253 cells were cultured in 10% fetal bovine serum (Gibco) containing McCoy’s 5A medium (ATCC) under stimulation with IL-1β, tumor necrosis factor (TNF)-α, and interferon (IFN)-γ (R&D Systems) for 24 h to evaluate IL-33 production by salivary gland cells.
Our study protocol was approved by the Institutional Review Board of Seoul St. Mary’s Hospital (KC13SISE0293).
Clinical and laboratory profiles
All patients underwent comprehensive evaluations composed of clinical examinations and serological tests. Demographic data and clinical manifestations were collected. We measured autoantibodies distinctive of pSS including the following: antinuclear antibody (ANA), anti-SSA/Ro52 antibody, anti-SSB antibody, and rheumatoid factor. Inflammatory markers, such as erythrocyte sedimentation rate and C-reactive protein, were also assessed. Other laboratory data included complete blood cell counts and immunoglobulin G. Disease activity of all included patients was assessed by the European League Against Rheumatism Sjögren Syndrome Disease Activity Index (ESSDAI), based on clinical and laboratory findings24.
Measurement of IL-33 and sST2 concentration
Serum levels of IL-33 and sST2 were measured using ELISA (R&D Systems). All procedures were performed according to the manufacturer’s instructions.
Immunohistochemical staining for IL-33 and ST2
Salivary gland tissue was snap-frozen in liquid nitrogen and stored at −80°C. Tissue sections were blocked with 1% normal goat serum, followed by staining with antibodies to IL-33 (1 μg/ml, R&D Systems), ST2 (1 μg/ml, R&D Systems), and an isotype control antibody (1 μg/ml, R&D Systems). The sections were then incubated with the appropriate biotinylated secondary antibodies (Santa Cruz Biotechnology), followed by an avidin–enzyme complex. Phosphate buffered saline containing 0.05% Tween 20 was used for washing after each step. Chromogenic reactions were visualized with 3, 3′-diaminobenzidine (Sigma), and nuclei were counterstained with hematoxylin. Slides were mounted in permanent mounting media (Dako).
Confocal microscopy
Tissue sections (7 μm) were fixed in 4% paraformaldehyde and stained using purified anti-IL-33 antibody (R&D Systems), phycoerythrin-conjugated anti-human cytokeratin antibody (Biolegend), and allophycocyanin-conjugated anti-human CD31 antibody (Biolegend). After an overnight incubation at 4°C, the slides were stained with FITC-conjugated secondary antibody for IL-33 staining. The same procedure, except anti-IL-33 staining, was repeated to rule out the autofluorescence of salivary tissues. The analysis was performed using the LSM 510 Meta confocal microscopy system (Zeiss).
Quantitative reverse transcription-PCR
mRNA was isolated using Trizol (Invitrogen) according to the manufacturer’s instructions. Total RNA (2 μg) was reverse-transcribed for 10 min at 25°C, 30 min at 55°C, and 5 min at 85°C using the Transcriptor First Strand cDNA Synthesis kit (Roche). Real-time PCR amplification was performed with 0.3–0.5 μl reverse transcription product in a StepOne plus machine (Life Technologies) using the FastStart Universal SYBR Green Master (Roche) according to the manufacturer’s guidelines. The following sense and antisense primers for each molecule were used: IL-33 (forward) 5′−ATC CCA ACA GAA GGC CAA AG−3′ (reverse) 5′−CCA AAG GCA AAG CAC TCC AC−3′; and β-actin (forward) 5′−GGA CTT CGA GCA AGA GAT GG−3′ (reverse) 5′−TGT GTT GGG GTA CAG GTC TTT G−3′. The PCR cycling conditions were as follows: 10 min at 95°C, 45 cycles of 15 s at 95°C, 45 s at 60°C, and 20 s at 72°C. To verify that equivalent amounts of RNA added to each PCR reaction, PCR amplification of β-actin was performed for each sample. Relative fold induction was calculated using the equation 2−(ΔCp), where ΔCp was Cp(target) − Cp(β-actin), and Cp was the cycle at which the threshold was crossed. PCR product quality was monitored using post-PCR melting curve analysis.
Statistical analysis
Comparisons of age and sex between patients with pSS and controls were performed with the Student t test and the chi-square test, respectively. Experimental values were presented as mean ± standard error. Statistical significance was determined by the Mann-Whitney U test or ANOVA with the Bonferroni posthoc test. The correlation of IL-33/sST2 with clinical profiles was analyzed using Spearman rank correlation coefficient. A p value < 0.05 was considered statistically significant. All data were analyzed using SAS 9.1 software (SAS Institute).
RESULTS
Patient characteristics
The clinical characteristics of the patients with pSS are presented in Table 1. The mean age of the patients with pSS was 54.3 years, and 52 of the 55 patients were women (94.5%). The age and sex of the control group were comparable with those of the patient group (p = 0.121 for age and p = 0.066 for sex). The median duration of pSS was 32.9 months in the patient group. ANA was positive in all patients except 2. The immunologic profiles revealed 89.1% positivity for anti-SSA/Ro52 antibody and 65.5% positivity for anti-SSB antibody. Inflammatory markers indicating systemic inflammation were not significantly elevated in the patients with pSS. The median score of ESSDAI was 3, ranging from 0 to 18.
Clinical characteristics of the patients with primary Sjögren syndrome. Values are n (%) unless otherwise specified.
Twenty-six patients (47.3%) presented with extraglandular symptoms, and Raynaud phenomenon was the most common manifestation other than glandular involvement.
Serum levels of IL-33 and sST2 were elevated in patients with pSS
Serum levels of IL-33 and sST2 were measured by ELISA. The mean values of IL-33 and sST2 were 439.62 ± 177.28 pg/ml and 293.17 ± 82.36 pg/ml in patients with pSS, respectively. Sera from controls revealed significantly lower levels of IL-33 and sST2 with mean values of 427.22 ± 273.22 pg/ml and 144.61 ± 94.15 pg/ml, respectively (p = 0.018 for IL-33 and p < 0.0001 for sST2; Figure 1A). No association was detected between IL-33 and the clinical variables in patients with pSS. However, serum sST2 levels seemed to be elevated when accompanied with hematologic abnormalities (Figure 1B). In particular, thrombocytopenia had a significant association with sST2 levels (p = 0.029). A correlation analysis also revealed that sST2 concentration was positively related with the duration of pSS (p = 0.013, r = 0.337) and ESSDAI score (p = 0.042, r = 0.275; Figure 1C).
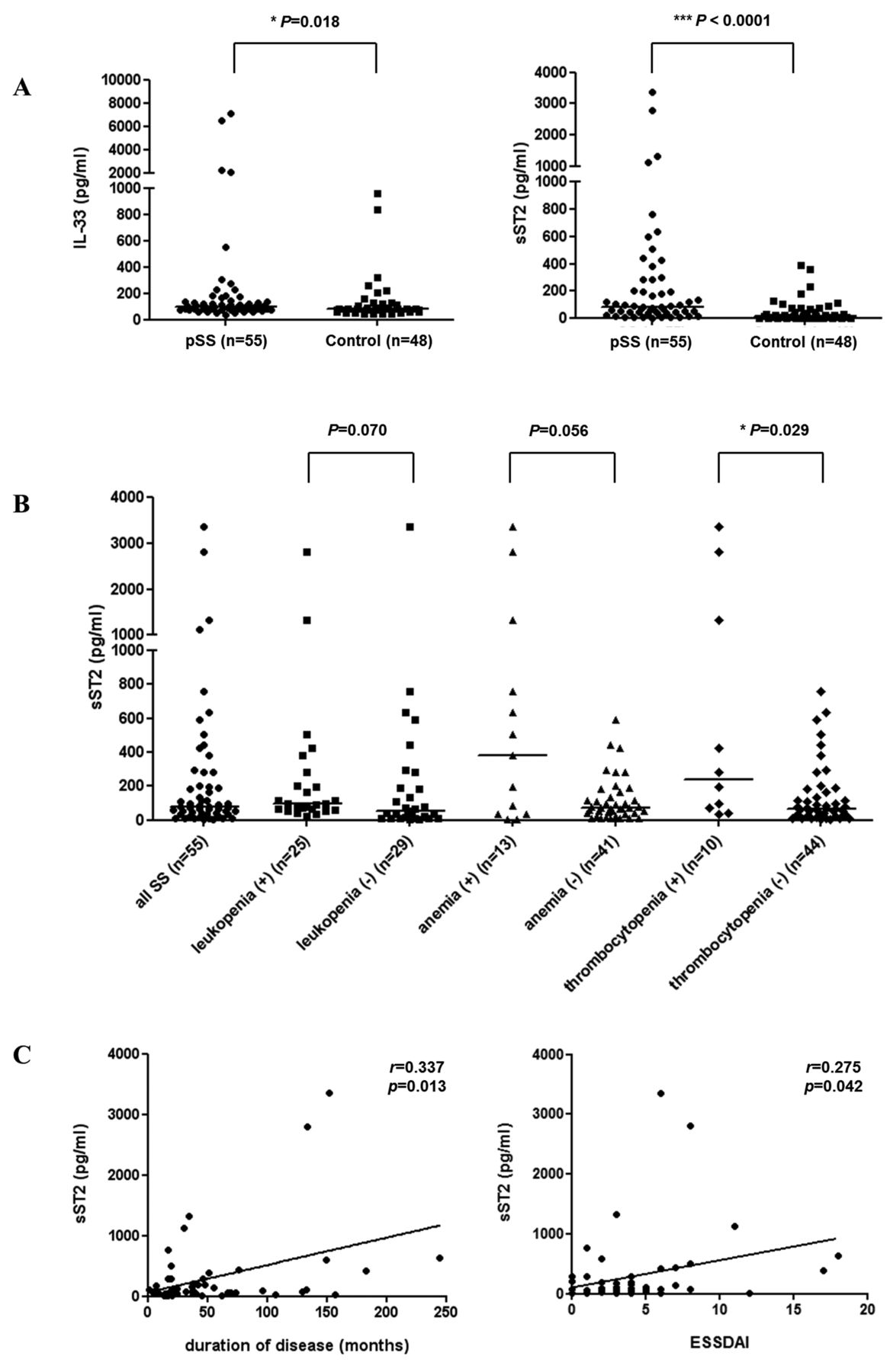
Elevated serum levels of IL-33 and sST2 in patients with pSS. A. Serum concentrations of IL-33 and sST2 were measured by ELISA in patients with pSS (n = 55) and controls (n = 48). B. Serum sST2 levels in the patients with pSS were compared according to hematologic manifestations. C. The correlations between sST2 concentrations and clinical profiles were analyzed in the patients with pSS. Horizontal bars represent the median of individual values within a group. IL: interleukin; pSS: primary Sjögren syndrome; ESSDAI: EULAR Sjögren syndrome disease activity index; EULAR: European League Against Rheumatism.
The expression of IL-33 and ST2 in salivary tissues from patients with pSS decreased as the histological grade progressed
The histological grade of salivary glands was determined from grade 0 to grade 4 by standardized criteria23. To examine in situ expression of IL-33 and ST2, all lip biopsy specimens obtained from subjects with and without pSS were sectioned and stained with antibodies to IL-33 and ST2. The tissues were also stained with isotype antibodies as a negative control. The salivary glandular tissues of controls were rarely stained with antibodies to IL-33 and ST2. In grade 1 of lymphocytic infiltrates, staining with IL-33/ST2 antibodies was dim. The expression of IL-33 and ST2 was markedly increased in grade 2 of inflammation, and weakened in grade 3 and 4 of inflammation with 1 or more focuses (Figure 2A and Figure 2B). The immunoreactivities were mostly observed in the glandular structures of salivary glands.
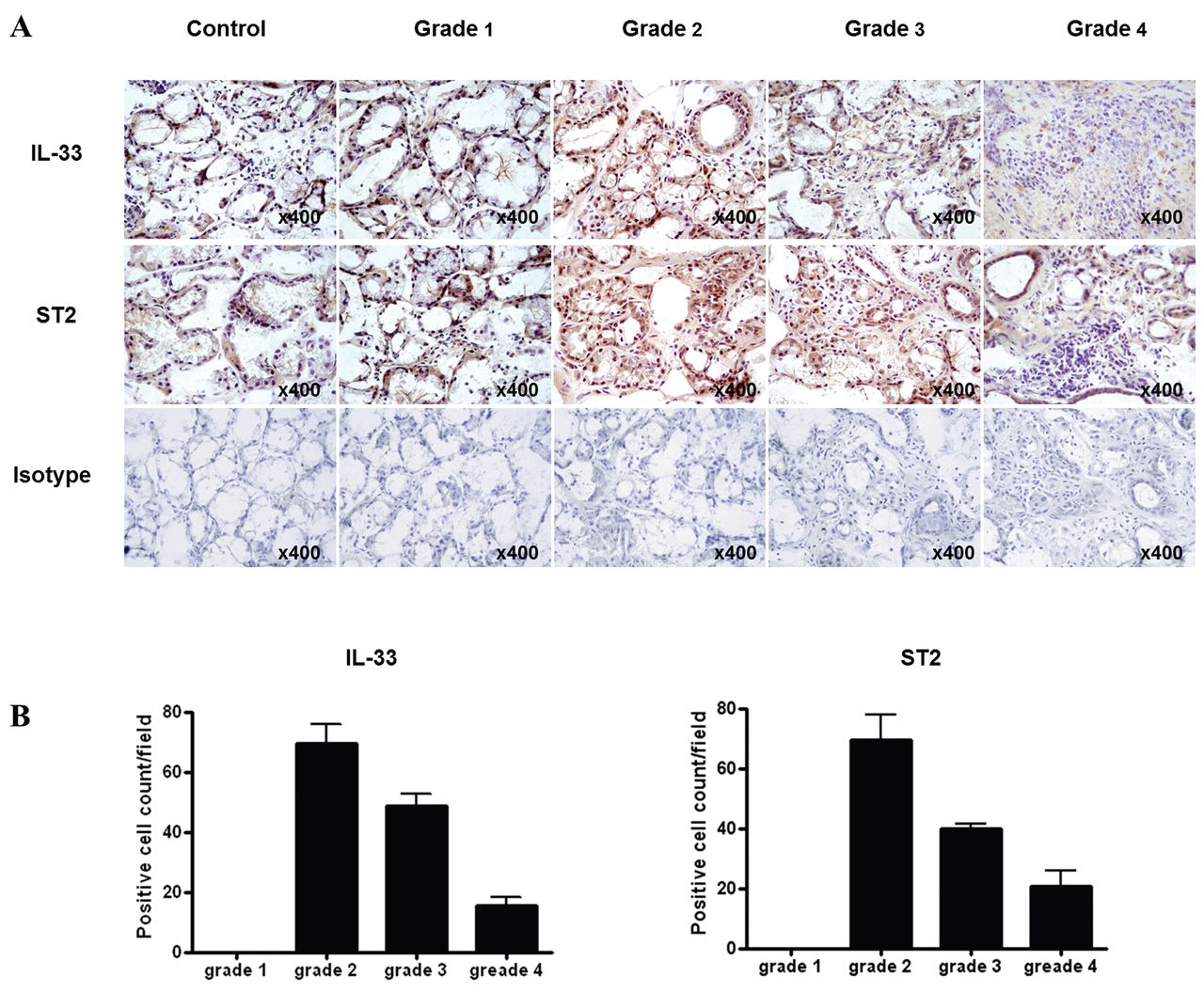
Diminished expression pattern of IL-33 and ST2 in salivary glands of patients with pSS with higher histological grade. A. Salivary tissues of patients with pSS were stained with antibodies to IL-33 and ST2. Immunohistochemical staining shows different levels of expression according to the histological grade. B. The expressions of IL-33 and ST2 in different grade of salivary glands were determined by the number of cells stained with IL-33/ST2 antibodies in high-power field. Data are expressed as mean ± standard error, and are representative of 3 experiments. IL: interleukin; pSS: primary Sjögren syndrome.
Sources and presentation of IL-33
IL-33 was mainly expressed in ductal epithelial cells and endothelial cells of salivary glands, and the production of IL-33 mRNA in salivary gland epithelial cells was stimulated by IFN-γ. IL-33 presents in various human cell types, including endothelial and epithelial cells. To investigate the major source of IL-33, the tissue sections were simultaneously stained with antibodies to cytokeratin and CD31 as markers of epithelial cells and endothelial cells, respectively. Confocal microscopy showed IL-33 positive cells merged with the expression of cytokeratin and CD31 (Figure 3A). Therefore, we confirmed that IL-33 is expressed in epithelial and endothelial cells of inflamed glandular tissues.

{kind=link}
{kind=link}
{kind=link}
Expression of IL-33 in ductal epithelial and endothelial cells from patients with pSS, and the induction of IL-33 mRNA in salivary gland epithelial cell by stimulation with proinflammatory cytokine. A. Salivary gland tissue from patients with pSS was stained with specific antibodies to IL-33 (green), cytokeratin (red), and CD31 (white). IL-33 expression in epithelial and endothelial cells was assessed by double immunofluorescent staining and confocal microscopy. The images in the bottom right corners represent the magnified results of white and yellow boxes. The arrows indicate the double-positive cells stained with specific antibodies. B. A253 cells, a salivary gland epithelial cell line, were cultured with or without proinflammatory cytokines, including IL-1β, TNF-α, and IFN-γ for 24 h. IL-33 mRNA was measured in the culture supernatant. Data are expressed as mean ± standard error, and are representative of 3 experiments. ** p < 0.01. Nil: no stimulation; NS: not significant; pSS: primary Sjögren syndrome; IL: interleukin; TNF: tumor necrosis factor; IFN: interferon.
To verify the induction of IL-33 in salivary gland epithelial cells under the inflammatory condition, A253 cells were cultured in the presence of IL-1β, TNF-α, and IFN-γ. The level of IL-33 mRNA increased significantly after stimulation with IFN-γ (p < 0.01). However, IL-1β and TNF-α did not promote the production of IL-33 mRNA in A253 cells (Figure 3B).
DISCUSSION
We demonstrated the increased level of IL-33 and sST2 in sera of patients with pSS, as well as an association between sST2 concentration and clinical profiles. The expression of IL-33 and ST2 was elevated in salivary glands of patients with pSS, but it was downregulated in tissues with advanced inflammation.
Two different studies have reported that serum levels of IL-33 and sST2 are higher in patients with pSS compared to those in healthy controls25,26, which was consistent with our results. However, we had some different observations in our study. Contrary to a prior report25, the presence of interstitial lung disease (ILD) did not affect serum concentrations of IL-33 and sST2, and no correlation was observed between IL-33 concentration and autoantibodies. This discrepancy might be attributed to the differences in the study population. In the previous series, more patients with ILD were included and the autoantibody profiles were different.
We found a possible association between clinical variables and sST2 rather than IL-33. According to previous research, sST2 levels correspond with the disease activity of autoimmune disorders13,14,15,27. Moreover, sST2 has been described as a prognostic factor in other medical conditions, such as sepsis, heart failure, and hepatocellular carcinoma28,29,30,31. In our study, sST2 concentration was correlated with ESSDAI. In particular, serum level of sST2 tended to be higher in patients with pSS with low blood cell count. Hematologic disorders, including leukopenia, anemia, and thrombocytopenia, are a clinical domain in the ESSDAI24. Therefore, sST2 levels could partially reflect the disease activity of pSS. In addition, sST2 levels were associated with disease duration. Although there is a lack of data indicating a direct association between tissue destruction and disease duration, longterm inflammation can induce glandular damage and dysfunction.
The decoy receptor of IL-33, sST2, regulates IL-33 function by binding and neutralizing IL-33. Ohto-Ozaki, et al observed increased serum sST2 levels in response to serial injections of IL-33, and suggested that sST2 was a negative regulator of IL-3332. Earlier evidence also indicated the antiinflammatory effects of sST2. Administration of sST2 attenuates the inflammation in a collagen-induced arthritis model33, and adenovirus-mediated overexpression of sST2 protects against the lipopolysaccharide-induced lung injury in mice34. Further, sST2 expression is induced by proinflammatory cytokines35, and in turn, sST2 suppresses production of inflammatory cytokines36,37. Thus, sST2 might reveal the severity of inflammation, as well as act as a defense mechanism.
The expressions of IL-33 and ST2 were elevated in salivary glands of patients with pSS compared to those of controls. However, salivary glands with higher histological grade showed a decreasing pattern of IL-33 and ST2 expression as the degree of inflammation increased. This finding is consistent with a recent study showing downregulated expression of IL-33 and ST2 in grade 3 and 4 compared to grade 226. In grade 2 of salivary glands, the glandular structures were mostly preserved with prominent lymphocytic infiltration. Destruction of salivary tissues was increasingly noted as the histological grade advances. This would explain the expression patterns of IL-33 and ST2 because IL-33 and ST2 were mainly observed in the ducts of salivary glands similar to the earlier report26.
We confirmed the expression of IL-33 in epithelial and endothelial cells of salivary glands. In addition, we first reported that the production of IL-33 mRNA by salivary epithelial cell can be promoted by IFN-γ stimulation. The biological significance of IL-33 is not only as an extracellular cytokine, but also as an intracellular protein with nuclear function that is released in response to cell damage and acts as an alarmin4,38. Because pSS can be accompanied by glandular inflammation and destruction, it is unclear whether IL-33 is secreted for extracellular functions or is released as a danger signal in pSS. However, the induction of IL-33 expression by IFN-γ suggests a potential role in the pathogenesis of pSS. One recent study26 supported the pathophysiological role of IL-33 based on the in vitro result that IL-33 triggers the secretion of IFN-γ by natural killer cells and natural killer T cells in conjunction with IL-12 and IL-23. We can assume that there could be a positive feedback between IL-33 and IFN-γ. IFN-γ is notably overexpressed in pSS, and is mainly secreted by type 1 Th cells. Accordingly, polarization toward the Th1 cell response is one of the major pathogenic features of pSS. Although IL-33 is known to skew the T cell population toward a type 2 helper cells phenotype, the current results suggest that IL-33 can also play a pathophysiological role through the interaction with IFN-γ.
The IL-33/ST2 signaling pathway might be involved in the pathogenesis of pSS. Increased expression of IL-33 might contribute to the progression of pSS, and sST2 could reflect disease activity and play a protective role. More data from in vivo experimental models are required to explain the precise role of IL-33/ST2 in the pathogenesis of pSS.
Footnotes
-
Supported by a grant from the Korea Healthcare Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (HI13C0016).
- Accepted for publication October 15, 2014.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.