
Abstract
Objective. To determine the epidemiology, clinical features, and microbiology of adult native joint septic arthritis in Canterbury, New Zealand, over a 5-year period in individuals with and without an underlying rheumatic disorder.
Methods. Patients with native joint septic arthritis were identified retrospectively and classified by Newman’s criteria. The clinical characteristics were described and comparisons made between those with and without underlying rheumatic disease.
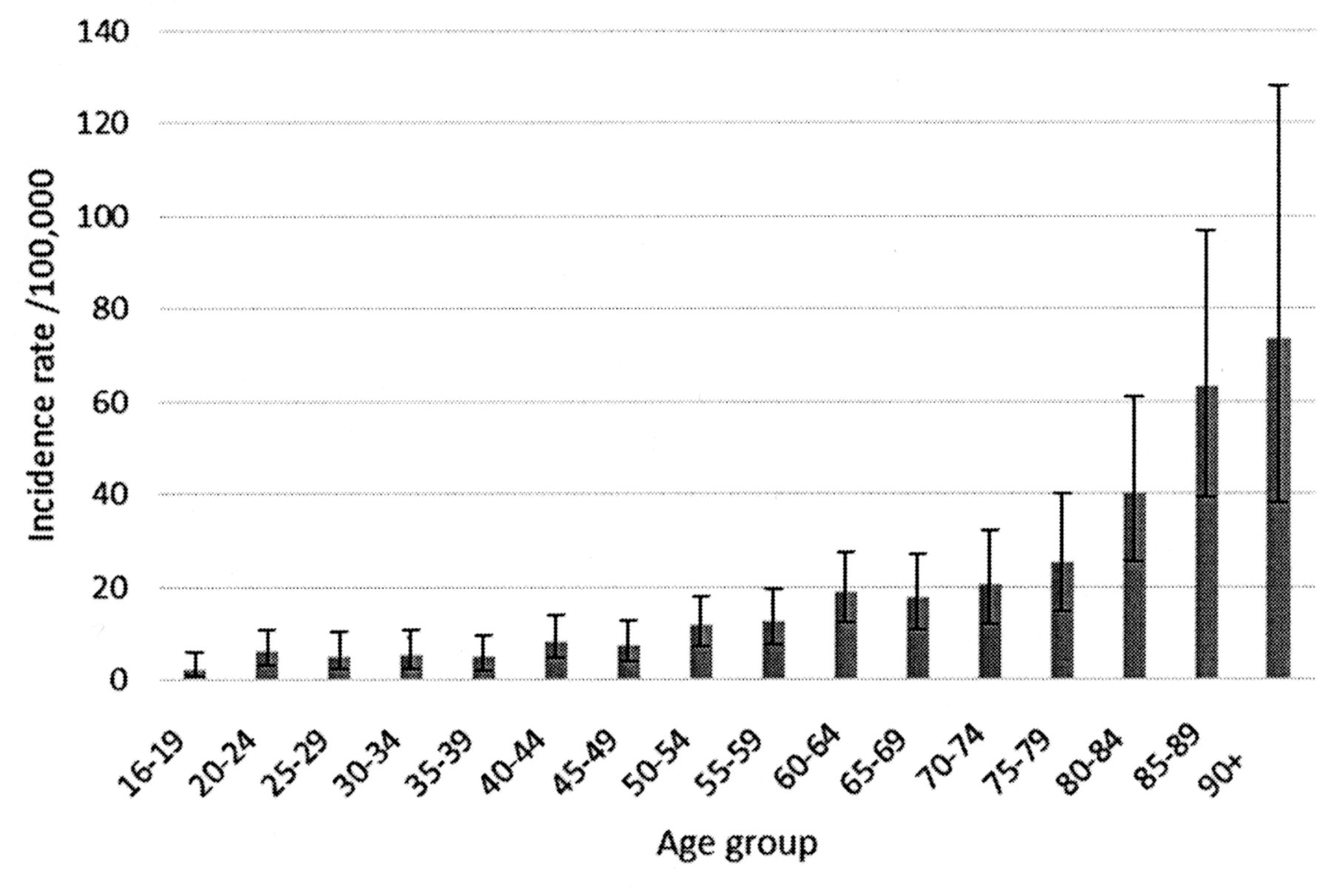
Results. Two hundred forty-eight cases of native joint septic arthritis (mean age 60, range 16–97 yrs) were identified with an overall incidence rate of 12.0/100,000/year (95% CI 10.6–13.6). Yearly incidence increased with age to a maximum of 73.4/100,000 in those > 90 years of age. Septic arthritis was iatrogenic in 16.9% of cases while 27% had an underlying inflammatory arthritis including gout (14.9%), calcium pyrophosphate disease (8.5%), and rheumatoid arthritis (4%). Few patients were taking immunosuppressant therapy, with just 1 taking a biological agent. Staphylococcus aureus was the most commonly identified organism. Those with underlying inflammatory arthritis were significantly older (73.6 yrs vs 55.6 yrs; p < 0.001), more likely to be female (55.2% vs 26.0%; p < 0.001), and to have septic polyarthritis (16.4% vs 4.4%; p = 0.002). The 30-day mortality was 2%, increasing to 6% at 90 days.
Conclusion. The incidence of septic arthritis in Canterbury, New Zealand, is higher than in previous studies. Crystal arthropathy commonly coexisted with infection although autoimmune arthritis and immunosuppression was less of a factor than anticipated.
- SEPTIC ARTHRITIS
- EPIDEMIOLOGY
- NEW ZEALAND
- NATIVE JOINT
- CRYSTAL ARTHROPATHY
Septic arthritis is an uncommon but important cause of a painful swollen joint. Prompt recognition of infection and institution of appropriate drainage procedures and antibiotic treatment are essential to minimize irreversible joint damage. Even with treatment, septic arthritis has a reported mortality rate of 11%, increasing to 19% in patients older than 60 years1,2. The incidence of septic arthritis in Western countries is considered to be rising, with increasing age, medical comorbidities, skin infections, orthopedic procedures, and underlying rheumatic disease all being important risk factors3,4.
There are a number of possible reasons rheumatic disease predisposes to septic arthritis. Structurally abnormal and inflamed joints are likely more prone to bacterial colonization both from hematogenous spread and direct infiltration5. Patients with underlying joint disease are more likely to have joint procedures performed, and depending on the underlying cause, may have abnormal immune function either due to the disease itself or its treatment with disease-modifying agents. Over the last decade the treatment of rheumatic diseases such as rheumatoid arthritis (RA) has been revolutionized by newer biological therapies that may increase the risk of joint infection6.
For such an important condition, there are few large studies of native joint septic arthritis. To address this we undertook a retrospective population-based study of the yearly incidence, demographics, microbiological causes, and underlying rheumatic conditions in Canterbury, New Zealand, over the 5-year period 2009–2013.
MATERIALS AND METHODS
Data sources and population
Christchurch District Health Board (CDHB) provides public healthcare for 482,000 patients, with 71% living in urban Christchurch, New Zealand’s second-largest city. Acute and tertiary level care is primarily provided at Christchurch Hospital, with Ashburton Hospital south of Christchurch being the only other acute-care facility. CDHB operates a number of other facilities across the region providing elective, rehabilitation, and psychiatric services. The CDHB maintains a common database for all institutions for which it is responsible. No private hospitals provide acute inpatient care, and so are unlikely to care for patients with septic arthritis.
All cases of septic arthritis were identified through an International Classification of Diseases (ICD), 10th edition, code search of discharge summaries using septic arthritis specific codes M00.0–M00.9. A database used by the infectious disease department with information on patients treated in the community with intravenous antibiotics was also searched. From the ICD-10 code search, 1191 potential cases were identified, with a further 348 from infectious disease records. After excluding duplicates, patients younger than 15, and nonresidents, the remaining 602 notes were reviewed by a single rheumatology trainee adjudicated by a professor of infectious diseases for a small number of cases (Figure 1). Estimated adult population data for the CDHB region by sex and 5-year age group of each study year were obtained from Statistics New Zealand.

Flow chart for gathering cases of septic arthritis. ICD 10: International Classification of Diseases, 10th ed.; ID: infectious disease.
Data collection, definitions, and statistical analysis
Patients were defined as having septic arthritis using modified Newman’s criteria7. The essentials of this definition are (1) Group A: microbial pathogen isolated from synovial fluid (SF) or joint tissue; (2) Group B: clinical features of septic arthritis with organism isolated from other source such as blood, urine, or swabs; (3) Group C: clinical features of septic arthritis with radiological evidence of septic arthritis or turbid SF aspirate from joint.
Patients with septic arthritis of the spine or chronic osteomyelitis were excluded from analysis. Only the first episode of septic arthritis for any 1 patient in the 5-year period was included.
Data were collected on patient age, sex, and ethnicity. A Charlson comorbidity score was generated by the CDHB clinical records department from electronic notes8. This score includes 22 major medical comorbidities and was used as an indicator of underlying comorbidities. Clinical data including presence of underlying inflammatory arthritis, joints involved, recent injection or instrumentation, and immunosuppressive treatment were recorded from the medical records. Patients were considered to have gout or calcium pyrophosphate disease (CPPD) if they had a medical history of these conditions or had monosodium urate or CPP crystals identified on SF microscopy. Diagnosis of other underlying joint pathology was based on clinical notes including those of the CDHB Department of Rheumatology, Immunology, and Allergy.
All data were collected in a systematic manner and entered into a database for analysis. A combination of descriptive and comparative statistics was used. All statistical analysis was completed using GraphPad (GraphPad Software Inc.). The chi-squared test was used for categorical variables and the Mann-Whitney U test was used for continuous, non-normally distributed data. Incidence rates were calculated by dividing the number of cases per year by the yearly adult Christchurch population. Ethical approval was given by the University of Otago Human Ethics committee (HD13/01).
Microbiological identification of septic arthritis cases
All diagnostic samples were taken as clinically indicated and processed at Canterbury Health Laboratories in the routine diagnostic microbiology laboratory. All specimens were examined microscopically by gram stain and Ziehl–Neelsen stain if the gram stains were negative. Organisms were identified to species level by traditional methods using biochemical profiles or matrix-assisted laser desorption ionization time-of-flight mass spectrometry. Susceptibility testing was performed in accordance with Clinical and Laboratory Standards Institute. Special culture techniques, such as for mycobacterial species, were performed when clinically indicated. These included atypical clinical features at presentation, travel history, or failure to respond to initial treatment. Identification of species by 16S ribosomal sequencing was performed in culture-negative cases if indicated on discussion with clinicians.
RESULTS
Demographics
There were 248 confirmed cases of septic arthritis over the 5-year period 2009–2013 (Figure 1). Of these, 162, 43, and 43 met Newman’s criteria A, B, and C, respectively (Table 1).
Patient demographics. Data are n (%) unless otherwise indicated.
The number of cases per year ranged from 34 to 64. The crude incidence rates were 8.3, 11.2, 15.6, 12.8, and 12.2 for each year (Figure 2). Incidence progressively increased with patient age (Figure 3). In the group as a whole, significantly more men had septic arthritis [males 166/248 (66.9%) vs females 82/248 (33.1%); p < 0.001]. Ages and ethnicities are reported in Table 1.

Crude incidence rates of septic arthritis for each year of the study.

{kind=link}
{kind=link}
{kind=link}
Crude incidence rates of septic arthritis by age group.
Clinical characteristics
Septic arthritis affected a single joint in 229 cases (92.3%). The most common joints involved were shoulder [53 (21.4%)], knee [52 (21%)], and the small joints of the hand [37 (14.9%)]. An underlying inflammatory rheumatic disease was present in 67 patients including gout [37 (14.9%)], CPPD [21 (8.5%)], and rheumatoid arthritis [10 (4%)]. Of these patients, 11 were taking prednisone therapy, with a median dose 6 mg per day (range 5–60 mg), 10 were taking methotrexate, 3 hydroxychloroquine, and 1 each sulfasalazine and leflunomide. Just 1 patient was taking a biological agent [adalimumab (ADA)]. Infection was iatrogenic in 42 cases (16.9%), with 11 (4.4%) patients having a recent intraarticular injection and 31 (12.5%) having recently had a surgical procedure [rotator cuff repair (15), arthroscopy (5), fracture fixation (7), or other (4)]. Of these iatrogenic cases, organisms were identified from synovial aspirate in all cases following intraarticular joint injection and in 23 postsurgical procedure cases. One patient was human immunodeficiency virus–positive. Three patients met the Dukes criteria for endocarditis.
Microscopic examination for crystals was performed on synovial aspirate in 128 cases (51.6%). Dual pathology with both septic arthritis and crystal arthritis was present in 33 of these cases. Monosodium urate crystals were seen in 16 (10.7%), CPP in 19 (12.8%), and both monosodium urate and CPP in 2 (1.3%) SF aspirates. Of the cases of concurrent septic and crystal arthritis, 32/33 (97.0%) cultured organisms from either SF aspirate or blood culture. The median synovial white blood cell (WBC) count for those with concurrent septic and crystal arthropathy in our study was 38,250/mm3, with 2/13 (15.4%) having a WBC < 10,000/mm3.
Bacterial species were identified in 205 cases (82.3%). Of these, 115 (56.1%) were Staphylococcus aureus. Two of these were methicillin resistant. The other bacteria isolated are shown in Table 2.
Microbiology of septic arthritis cases.
The mortality at 30 days was 2%, increasing to 6% at 90 days. The mean age of those who died at 90 days was 79.5 years (range 25–97). Positive blood cultures were present in 52.2% of cases who died at 90 days. At the time of reporting, 78% of patients were alive after a median length of followup of 40 months (range 14–74 mos). There was no significant difference in mortality stratified by the Charlson index at presentation.
Comparison of cases with and without underlying rheumatic disease
Those with underlying rheumatic disease were older (mean 73.6 vs 55.6 years; p < 0.001) and more likely to be female [35/67 (52.2%) vs 47/181 (26%); p < 0.001]. The distribution by Newman’s criteria was similar (A 50/67, B 8/67, and C 9/67). Septic polyarthritis was more common [11/67 (16.4%) vs 8/181 (4.4%); p = 0.002] although the joints involved followed a similar pattern. There was no difference in the proportion of organisms that caused septic arthritis.
DISCUSSION
The overall incidence rate of native joint septic arthritis was 12.0/100,000 over the 5 years of this study. This is higher than previously reported studies of Western European populations in which a rate of 4–10/100,000, including prosthetic joint infections, has been reported4,5,9. In each of these studies, prosthetic joint infection involved 8–10% of cases. There are a number of possible reasons for the increased incidence in our population. Because this study was done in a single district health board with multiple methods of case identification, it is unlikely that a significant number of cases would be missed. Because the incidence of septic arthritis is increasing, older studies likely underestimate current incidence4. Our population has a high proportion of elderly patients and it is recognized both in this study and others that risk of septic arthritis increases with age2. Finally, New Zealand has a high and increasing rate of bacterial infections, which would increase the risk of septic arthritis through hematogenous and direct spread10.
No previous studies have documented the incidence of septic arthritis in New Zealand. One previous Australian study gave an incidence rate of 9.2/100,000, with a rate of 29.1/100,000 in the indigenous aboriginal population11. In comparison, our study did not suggest New Zealand Maori have an increased risk of septic arthritis compared to the general population.
In 7.7% of cases, infection involved multiple joints, highlighting that polyarthritis does not exclude infection as the underlying cause. This is particularly true if the patient had an underlying inflammatory arthritis (16.4% of such cases had septic polyarthritis).
An underlying inflammatory rheumatic disease and in particular crystal arthropathy commonly coexisted with infection. There are likely multiple mechanisms by which underlying joint disease increases the risk of septic arthritis. Inflamed joints are likely more prone to bacterial colonization both from hematogenous spread and direct infiltration5. Patients with underlying joint disease are more likely to have joint procedures performed, and depending on the underlying cause, may be taking immunosuppressant therapy.
RA has previously been identified as a risk factor for septic arthritis, although the extent of this is not well defined. Weston, et al9 reported that 16% of their cases of septic arthritis had RA while Edwards, et al12 reported a 12.9-fold increase in septic arthritis in patients with RA compared to controls. While we do not have data on the local prevalence of RA, the prevalence in similar European populations is estimated at 0.5–1.1%13, which would suggest a 4- to 8-fold increase in incidence of septic arthritis in patients with RA. Few patients with septic arthritis were taking immunosuppression, with only 1 patient receiving a biological agent, the anti–tumor necrosis factor (TNF) inhibitor ADA. Over the period of our study, the rheumatology department issued 298 prescriptions for biological therapy, making it unlikely that this case represents a worrisome safety signal for septic arthritis. Galloway, et al6 estimated the risk of septic arthritis in those with RA treated with anti-TNF therapy is double that of patients receiving traditional disease-modifying agents.
Our study along with others has revealed an association between septic and crystal arthropathy and highlighted that the presence of crystals on aspirate does not rule out septic arthritis14,15. In our study, 58 patients (23.4%) were either known to have a crystal arthropathy or had crystals identified through SF analysis. Because septic arthritis and crystal arthritis can present with a similar clinical pattern of inflammatory monoarthropathy or polyarthropathy, with or without fever, differentiating the 2 can present a diagnostic challenge. Neither the number of joints involved nor the SF WBC count can reliably differentiate those who may have concurrent infection, so a high degree of suspicion is warranted. Even when a patient is known to have a crystal arthropathy or has crystals identified by microscopy, it is imperative that septic arthritis be considered as a differential and that all aspirates are cultured.
Iatrogenic infections are an important and increasing cause of joint infections4. The risk of septic arthritis is estimated at 1/20,000–1/500,000 for arthrocentesis and 1/50–1/200 for arthroscopy4. In our study, 16.9% of cases were iatrogenic, with 4.4% having a recent joint injection and 12.5% having a joint procedure including rotator cuff repair and arthroscopy. This rate corresponds favorably to Geirsson, et al4, who reported iatrogenic infection being the cause of 41.8% of cases of septic arthritis in Iceland. Clinical experience and proper aseptic technique are of great importance when performing arthrocentesis, although optimal sterilization and technique have not been extensively studied16.
As in other studies of septic arthritis, S. aureus was the dominant infecting organism4,5,9,11,14,17. Of interest, 9 out of 10 cases of Propionibacterium acnes infection involved the shoulder; all of these patients had undergone recent rotator cuff procedures. P. acnes is a gram-positive bacillus of low virulence that is commensal in the sebaceous follicles of the head, neck, and thorax. It has been observed to be an important cause of shoulder infections in other studies, so in this circumstance should not be considered a contaminant18,19,20. Our study showed Neisseria gonorrhoeae is no longer a common cause of septic arthritis in adults, with just 2 cases in the 5-year period.
Our study has several limitations because of its retrospective design and reliance on ICD coding and medical records. While this raises the possibility of cases being missed, given the multiple methods of case identification, this effect is not likely to be large. In comparison to our study of adult native joints, most previous studies have included prosthetic joint infections and pediatric populations. While this creates some difficulties in comparing results, the increased incidence in our population is still clearly evident. Pediatric populations are known to have higher rates of septic arthritis than adults, so including them and prosthetic infections would both serve to increase the observed incidence rate4,9.
The case definition used for septic arthritis will affect incidence, joint distribution, and microbiology. Newman’s criteria were used for our study because they represent the most commonly used definition of septic arthritis. This criteria set uses both microbiological and clinical features and strikes a balance between case certainty and inclusiveness. In Newman’s category A, the identification of pathogens from SF is rarely equivocal, but in Newman’s B and C in some cases it may be less clear. Our case series contained proportions of patients in each Newman category similar to other previous studies7,9, suggesting similar judgments on cases were made.
Septic arthritis of the shoulder and P. acnes infection were both prominent findings that are partially explained by the inclusion of postsurgical cases such as rotator cuff repairs. Even taking this into account, the proportion of infections involving the shoulder was higher than previous studies. The reasons behind this are not clear.
In any study of infection, the microbiological methods of identification will influence what organisms are found. Unusual or fastidious infections may not be identified by routine diagnostic laboratory techniques. It is noteworthy that brucellosis has been eradicated from New Zealand and Coxiella burnetii has never been found there, so these organisms were not sought. Clinical tuberculosis is very uncommon and is unlikely to be missed given awareness of the possible diagnosis and its failure to respond to beta lactam therapy, which is used routinely in culture-negative cases. Advances in molecular techniques such as specific real-time and broad-range polymerase chain reaction will be more important in identifying atypical pathogens in the future.
There is potential for errors in the population data we have used to calculate incidence rates. The accuracy of New Zealand Statistics data was likely affected by the major earthquake hitting the region during the study period. Much of the population movement, however, was within the area of the district health board and so would not affect incidence rates21.
Despite its limitations, our study shows that the incidence of septic arthritis is comparatively high in our population. Elderly patients have elevated rates, and iatrogenic infections frequently occur. Underlying crystal arthropathy is very common although RA appears to be a smaller risk factor than in other studies. While the numbers are small, immunosuppressant therapy (and in particular biological therapy) did not appear to be a major risk factor for septic arthritis.
Acknowledgment
We thank the staff of the Christchurch District Health Board Rheumatology and Infectious Diseases departments, and the University of Otago Arthritis Research Theme, who provided funding for a summer studentship.
- Accepted for publication August 10, 2015.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.