
Abstract
Objective. To determine the prevalence and type of ultrasonographic (US) lesions of the anterior chest wall (ACW) in cases of spondyloarthritis (SpA).
Methods. This monocentric, prospective, and controlled study included patients consulting for SpA (Assessment of Spondyloarthritis International Society criteria) and control subjects. Clinical (pain and swelling) and US assessments (synovitis, joint effusion, erosion, ankylosis, margin narrowing, or Doppler signal) were performed on the sternoclavicular (SCJ) and the manubriosternal (MSJ) joints. The main characteristics of SpA were recorded [disease duration, biologic features, Ankylosing Spondylitis Disease Activity Score (ASDAS), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), radiographic and extraarticular involvement].
Results. The study included 131 patients with SpA and 49 control subjects (same age and sex ratio). Clinical and US involvement of ACW were found in, respectively, 39% and 35.5% of SpA and in 12% and 14.3% of controls (p < 0.01). US highlighted erosions (34 vs 0), margin narrowing (12 vs 0), power Doppler activity (18 vs 2; p < 0.05), and ankylosis of the MSJ (24 vs 3). US involvement was associated with disease duration (14.9 vs 11.1 years; p = 0.04), age (45 vs 41 years; p = 0.004), radiographic change of sacroiliac joint (p = 0.05), and presence of inflammatory bowel disease (IBD; p = 0.03). No associations were found with HLA-B27, psoriasis, enthesitis, uveitis, or clinical involvement of ACW. Clinical involvement is associated with a higher BASDAI (47 vs 32; p = 0.0009) and ASDAS (2.9 vs 2.2; p = 0.006).
Conclusion. US involvement of ACW is frequent in SpA (36.5%), mainly with erosion of SCJ and ankylosis of MSJ. It is associated with disease duration, radiographic sacroiliitis, and IBD.
- ULTRASONOGRAPHY
- SPONDYLOARTHRITIS
- ANTERIOR CHEST WALL
Spondyloarthritis (SpA) is a chronic inflammatory rheumatic disease characterized by inflammation of the spine, often at the thoracic level. The lesion of the sacroiliac joint is recognized as a major sign for the diagnosis of SpA and is included in the ASAS (Assessment in Spondyloarthritis International Society) classification criteria1. Involvement of the anterior chest wall (ACW), not included in these criteria, is a typical lesion of SpA. Several studies have reported a clinical lesion of the ACW in 30%–50% of cases2,3 in advanced forms. Recently, a study from the DESIR cohort4 showed clinical involvement of the ACW in 44% of early forms of SpA.
The ACW location is not routinely explored. In a pilot study, Weber, et al5 found involvement of the ACW with magnetic resonance imaging (MRI) in about 50% of early or confirmed cases of SpA (5 patients). These results were confirmed in a larger study, with 122 SpA cases [including 96 ankylosing spondylitis (AS)]. In that study, MRI involvement of the ACW (bone marrow edema and/or erosion and/or synovitis and/or fusion and/or fat infiltration) was found in 59% of the cases6. MRI lesions may be present without clinical expression, and some consider MRI lesions of the ACW to have the same importance as sacroiliitis7. To date, there is no gold standard procedure for the imaging exploration of the ACW8. The computed tomography (CT) scanner is sensitive and can highlight structural bone lesions. MRI is more specific and reveals several types of lesions such as bone marrow edema, erosions, and synovitis. The CT scanner could be a good screening procedure and MRI a good diagnostic tool. The limits of these procedures are their high cost, their limited availability, and the use of radiation for the scanner.
To date, no study has focused on the contribution of ultrasonography (US) in the diagnostic management of ACW involvement in cases of SpA. This has been evaluated in rheumatoid arthritis (RA)9, and more US lesions than clinical lesions were found. This procedure has several benefits such as absence of side effects, speed of realization, sensitivity for detecting erosions, and availability in a routine practice.
The main objective of our study was to determine the prevalence and type of US lesions of the anterior chest wall in cases of SpA. The secondary objectives were to identify factors associated with US and clinical involvement.
MATERIALS AND METHODS
Patients
Our study was conducted from November 2012 to September 2013 in the Department of Rheumatology of the University Hospital of Besançon on consecutive inpatients and outpatients with a diagnosis of SpA according to ASAS criteria1 and control subjects free of any inflammatory rheumatism (subjects with disc-related sciatica and staff member). Exclusion criteria included patients less than 18 years old, absence of consent, steroid injection of a sternoclavicular joint less than 4 weeks before, sepsis, a history of thoracic surgery with thoracotomy, or sternal fracture. For each patient we recorded laterality, active smoking, class I HLA typing, presence of sacroiliitis and syndesmophytes on radiograph or MRI, disease duration, axial or peripheral phenotype of the disease, the presence of enthesitis and arthritis, history of uveitis, the presence of skin lesions (psoriasis, pustulosis), the presence of inflammatory bowel disease (IBD), current treatment, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), and Ankylosing Spondylitis Disease Activity Score (ASDAS)-CRP. Informed consent was obtained from each patient.
Clinical assessment
Patients and controls were examined in supine position with elbows placed in contact with the body. The right and left sternoclavicular (SCJ) and manubriosternal (MSJ) joints were investigated for (1) spontaneous pain (joint pain without pressure on the joint, asking the question: Are these joints painful?); and (2) pressure pain (intensity of the pressure for appearance of nail bed pallor). Costochondral junctions were not examined because they are not real joints.
US assessment
US B mode and Doppler power mode examination of the 3 joints were performed by 1 of 2 experienced rheumatologists. Before the study, the US examinations were standardized and interobserver agreement was reached. All US examinations were performed with the same device (Esaote MyLab 70 XVG using a 10–18 MH probe). For each patient and control subject, US examination included a longitudinal section of the left and right SCJ and the MSJ, followed by a cross-section in case erosion was detected. During the examination, synovitis, joint effusion, erosion, ankylosis, joint space narrowing, or Doppler signal were investigated. The elementary lesions were defined as follows: (1) synovitis: hypoechoic intracapsular incompressible area; (2) joint effusion: compressible anechoic intracapsular area, absence of Doppler flow; (3) erosion: disruption of the cortical bone line displayed in 2 perpendicular axes (different from bone irregularity by a clear disruption); (4) margin narrowing: the loss or reduction of the space between the 2 parts of the joints; (5) Doppler: power Doppler signal; and (6) ankylosis: loss of joint space. Costochondral junctions were not examined because they are not easily accessible with US for all patients.
Statistical analysis
Statistical analysis was performed using Statview software. Results of the standard descriptive study of the 2 groups were expressed as mean ± SD. Descriptive comparison between the 2 groups was performed by Student t test for continuous variables and chi-squared test for qualitative variables. P values < 0.05 were considered significant. Interobserver agreement was calculated with a κ test.
RESULTS
One hundred eighty subjects were included in the study. Demographic data of the patients with SpA are summarized in Table 1. A total of 131 patients with SpA and 49 control subjects were included. The 2 groups were statistically comparable in age and sex ratio. κ coefficient measured in 10 patients (30 joints) evaluated interobserver agreement at 0.85.
Demographic data of the spondyloarthritis (SpA) and control groups.
Prevalence
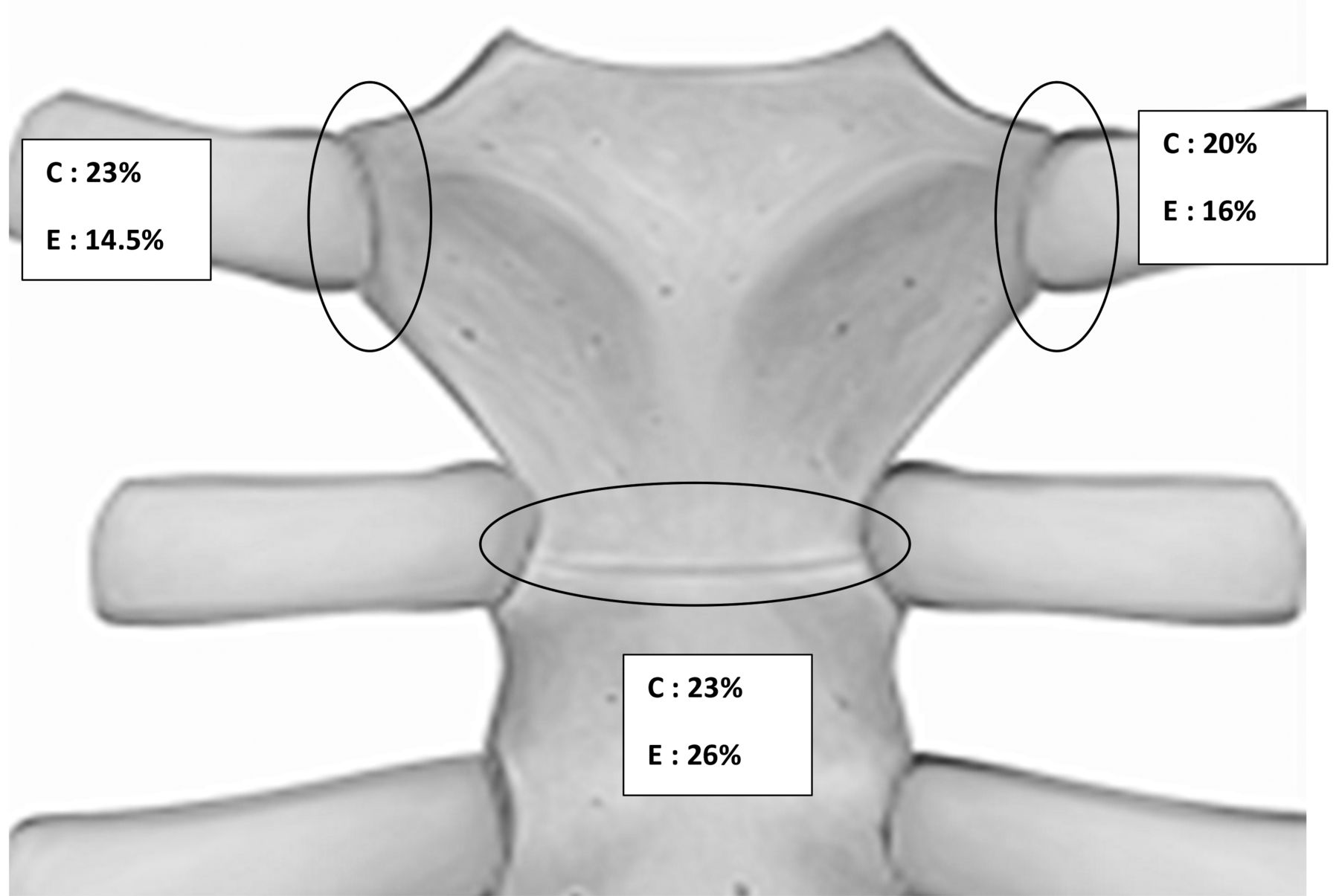
The prevalence of clinical involvement of the ACW was 39% in the SpA group versus 12% in the control group (p < 0.01). The prevalence of US involvement was 35.5% in the SpA group versus 14.3% in controls (p < 0.01). Among the 3 joints studied, there was a homogeneous distribution of lesions detected by clinical examination, but there was a predominance of manubriosternal lesions detected by US examination (Figure 1).
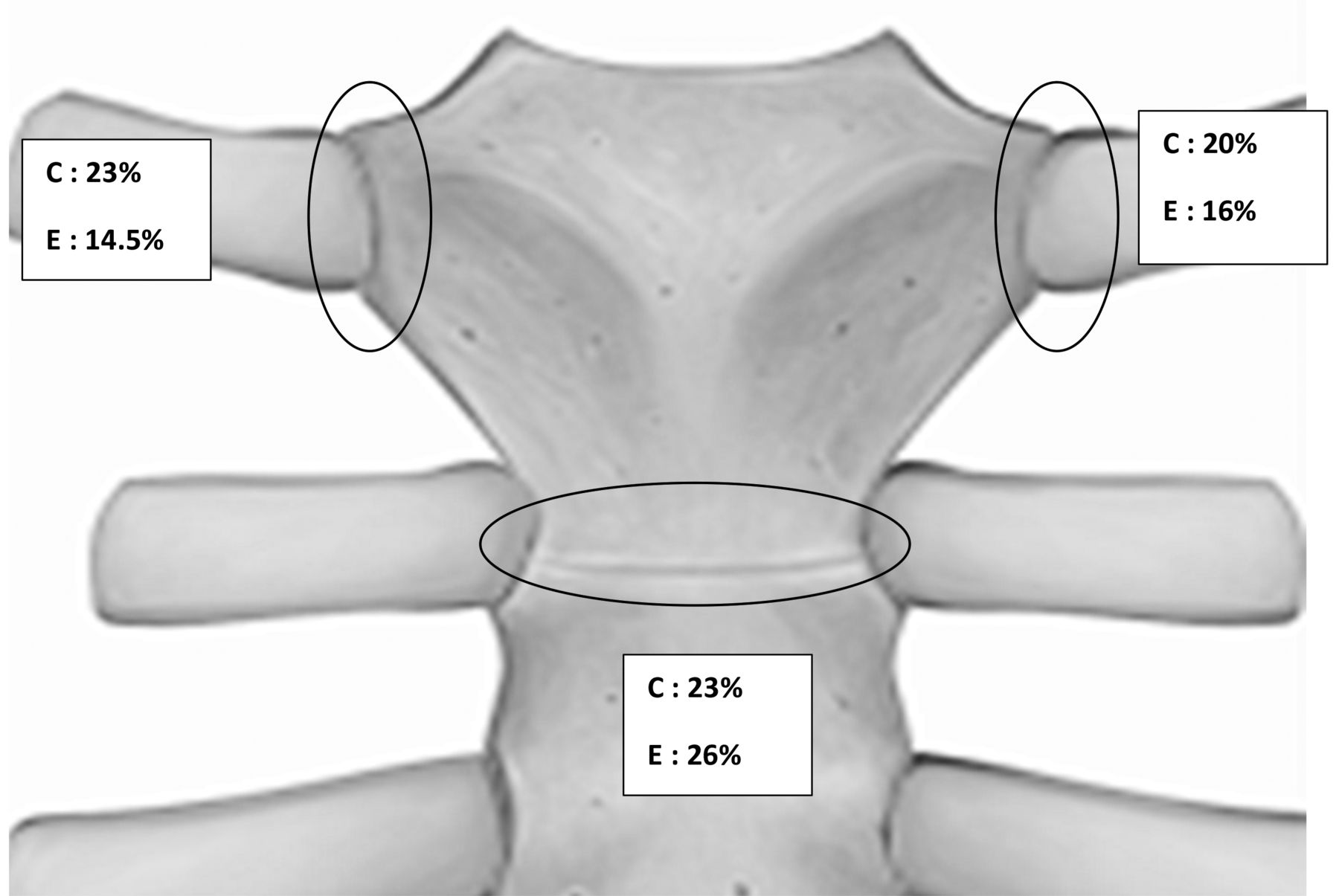
Distribution of clinical and ultrasound (US) involvement of the anterior chest wall in the spondyloarthritis group. C: clinical involvement; E: echography (US).
Type of lesion
US highlighted 34 erosions, 12 cases of margin narrowing, and 18 Doppler signals of these joints (primarily the SCJ) in the SpA group versus 0, 0, and 2 in the control group, respectively, with a significant difference (p < 0.05; Figure 2). There were 24 cases of ankylosis of the MSJ (Figure 2) in the SpA group versus 3 in the control group (p < 0.05). The SpA group had no more synovitis than did the control group.
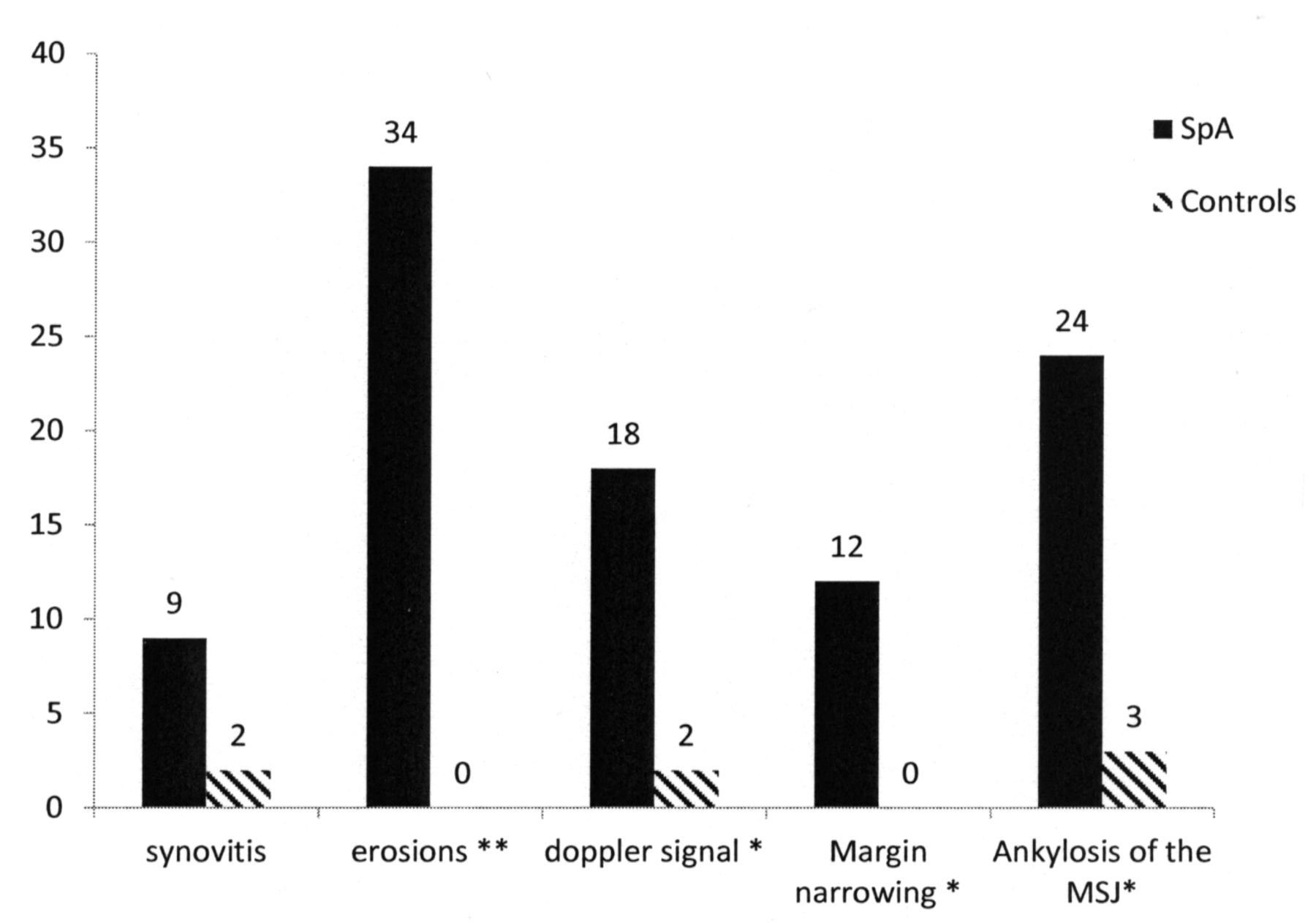
Type of ultrasound lesions of the anterior chest wall. Y axis = no. patients. * p < 0.05. ** p < 0.01. SpA: spondyloarthritis; MSJ: manubriosternal joint.
Factors associated with clinical involvement
In SpA, clinical involvement of the ACW was associated with the presence of HLA-B27 (p < 0.05) and with higher disease activity using both ASDAS-CRP (2.9 vs 2.2, p < 0.006) and BASDAI (47 vs 32, p < 0.0009). There were no correlations with presence of inflammatory syndrome (ESR, CRP), history of enthesitis, or ACW pain.
Factors associated with US involvement
In SpA, US lesions were associated with the presence of radiographic sacroiliitis (p = 0.05), disease duration (14.9 yrs vs 11.1 yrs, p = 0.04), patient age, and presence of Crohn disease (p = 0.03; Table 2); there was a trend for an association with smoking (p = 0.06). No association was found with HLA-B27, presence of psoriasis, enthesitis, or previous history of uveitis.
Factors associated with ultrasound (US) involvement of the ACW in the SpA group: comparison between patients with and without US involvement. Significant values are indicated in bold face.
Finally, there was no link between US lesions and clinical expression of the ACW.
Correlation between US lesions and clinical symptoms
We found that 20% of the patients had isolated clinical symptoms, 18% had both US lesions and clinical symptoms, and 17.5% had isolated US lesions (Figure 3). When patients presented both clinical symptoms and US lesions, there was not necessarily a topographical correspondence.

Percentage of patients with clinical and ultrasound involvement of the anterior chest wall.
DISCUSSION
US involvement of the ACW is frequent in cases of SpA. The study showed a homogeneous distribution of clinical involvement of the SCJ and MSJ. With US, we found a predominance of the involvement of the MSJ. This is in line with results from studies with MRI6. With radiographs, 1 study showed involvement of the MSJ in 51% of 76 patients with AS10,11. We found mainly ankylosis (in 24 patients) of this joint and very few inflammatory instances. This prevalence is higher than the prevalence found by MRI (11%). This may be due to the disease duration of our cohort — we included both early and established SpA.
The prevalence of US lesions was 35.5% in our study. This is lower than what is found in the literature with MRI, which places the prevalence at 59%–62%6,7. The bone scintigraphic examination highlights 50% involvement of the ACW in SpA2. MRI can highlight structural damage and especially bone edema and fat infiltration. The MRI study by Weber, et al6, showed prevalence of erosion at 34%, synovitis of the SCJ and MSJ at 13%, and ankylosis of the MSJ at 11%, closer to the type of lesions highlighted in US. In fact, US detected erosion at 25%, synovitis at 9%, and ankylosis of the manubriosternal joint at nearly 25%. The higher prevalence of these structural lesions (ankylosis) in our study may be explained by the longer disease duration in our cohort.
Statistically more radiographic sacroiliitis was observed in patients with US involvement of the ACW. Moreover, this US involvement was associated with disease duration and the patient’s age, and there was a tendency toward an association with active smoking. An association with the presence of IBD (Crohn disease) has been demonstrated. This was not previously described and this may be explained by the presence of a higher inflammatory syndrome in this population compared to the SpA without IBD (26.08 vs 9.1 mg/l, p < 0.001 for CRP; 43.3 vs 23.16 mm, p < 0.05 for ESR). Indeed, the most frequently detected US lesions were ankylosis of the MSJ (Figure 4), which can be considered as a postinflammatory lesion.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Different ultrasound lesions. A. Ankylosis of the MSJ. B. Normal MSJ. C. Synovitis with Doppler signal of the right SCJ. D. Multiple erosions of the right SCJ. MSJ: manubriosternal joint; SCJ: sternoclavicular joints.
We demonstrated a link between clinical involvement of the ACW and disease activity assessed by BASDAI and ASDAS. These results are in line with the literature4.
Clinical involvement of the ACW is not correlated with US involvement. There was 20% of clinical involvement without US abnormality and 17.5% of US involvement without clinical symptoms. Eighteen percent of patients had both US and clinical involvement without necessarily a spatial relationship, reflecting weak correlation between clinical and US findings. This finding corresponds with other studies using MRI6 or bone scan2. Some studies showed a correlation between clinical and bone scan involvement7, but the study population consisted mainly of psoriatic arthritis with a predominance of synovitis. In a study of patients with RA, there was a good correlation between clinical and US findings9. Again, the main lesions were synovitis and the clinical assessment included a current or previous history of pain. Our population includes mainly AS and it is not surprising that synovitis is rare and less frequent than erosions. In addition, we considered only current pain during examination as part of the clinical assessment and recorded history of pain of the ACW separately.
Our study highlighted erosions localized mainly to SCJ. A similar study was conducted in RA9 in which the prevalence of erosions on US was less important and where MSJ ankylosis was not described. In our cohort, synovitis lesions were not statistically more frequent than in the control group. The few instances of synovitis found in the SpA group occurred mainly in patients with peripheral forms and were not exclusively axial. In the axial forms, the profile of lesions is more structural than inflammatory.
Our study focused on the intensity of the disease and not on its consequences. The correlation was not evaluated. BASMI and chest expansion findings were not available for all the patients. It could be interesting to evaluate the relationship between US findings and clinical disability.
The limits of our study are the absence of double-blind examination and the use of a second imaging procedure as a control. The limit of US examination is that it is operator-dependent. Nevertheless, interobserver agreement was good with a κ coefficient of 0.85.
Involvement of the ACW is frequent in SpA and does not necessarily reflect a simultaneous clinical involvement. US can highlight specific structural damage of the ACW in SpA and could be an additional way to monitor the disease, particularly its structural effects. US could be useful in diagnosis to detect specific lesions, but this needs to be validated in a larger population.
- Accepted for publication August 5, 2014.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.