
Abstract
Objective. To determine the elapsed time while receiving aggressive therapy to the first observation of clinically inactive disease (CID), total duration of CID and potential predictors of this response in a cohort of children with recent onset of polyarticular juvenile idiopathic arthritis (poly-JIA).
Methods. Eighty-five children were randomized blindly to methotrexate (MTX), etanercept, and rapidly tapered prednisolone (MEP) or MTX monotherapy and assessed for CID over 1 year of treatment. Patients who failed to achieve intermediary endpoints were switched to open-label MEP treatment.
Results. Fifty-eight (68.2%) of the 85 patients achieved CID at 1 or more visits including 18 who received blinded MEP, 11 while receiving MTX monotherapy, and 29 while receiving open-label MEP. Patients starting on MEP achieved CID earlier and had more study days in CID compared to those starting MTX, but the differences were not significantly different. Patients given MEP (more aggressive therapy) earlier in the disease course were statistically more likely to have a higher proportion of followup visits in CID than those with longer disease course at baseline. Those who achieved American College of Rheumatology Pediatric 70 response at 4 months had a significantly greater proportion of followup visits in CID, compared to those who failed to achieve this improvement (p < 0.0001). Of the 32 patients who met criteria for CID and then lost CID status, only 3 fulfilled the definition of disease flare.
Conclusion. Shorter disease duration prior to treatment, a robust response at 4 months, and more aggressive therapy result in a higher likelihood and longer duration of CID in patients with poly-JIA. The original trial from which data for this analysis were obtained is registered on www.clinicaltrials.gov NCT 00443430.
- JUVENILE IDIOPATHIC ARTHRITIS
- EARLY AGGRESSIVE THERAPY
- CLINICALLY INACTIVE DISEASE
- CLINICAL TRIAL
- CHILDREN 2–16 YEARS
The development of biologic response modifiers (biologic disease-modifying antirheumatic drugs, DMARD) has revolutionized the treatment and prognosis of juvenile idiopathic arthritis (JIA). The use of biologic DMARD that block relevant inflammatory pathways make achieving and maintaining clinically quiescent disease a realistic expectation1,2,3,4. The polyarticular [rheumatoid factor (RF) positive and negative] categories comprise nearly 30% of all patients with JIA, and the majority of these children remain on multiple combinations of medications for many years5,6,7. Disease-free periods without medication longer than 1 year are uncommon8.
Newly published guidelines from the American College of Rheumatology (ACR) provide some guidance for the treatment of polyarticular juvenile idiopathic arthritis (poly-JIA)9. However, the optimal timing and sequencing of treatment, aggressiveness of treatment, and specific combinations of medications in patients most likely to be effective in achieving clinical inactive disease (CID) have yet to be determined.
The TRial of Early Aggressive Therapy (TREAT) study was a proof of concept study that randomized 85 patients with newly diagnosed poly-JIA to 1 of 2 aggressive treatment regimens10. TREAT demonstrated that CID could be achieved in a large proportion of patients within 6 months of initiating treatment10. Further, an early window of opportunity was evident; the likelihood of achieving CID increased by over 30% for each month earlier that aggressive treatment was started following disease onset.
The objectives of the present analyses were to assess data over the entire 1 year of patient participation in TREAT to determine (1) the elapsed time receiving aggressive therapy until the first occurrence of CID was observed, (2) the durability of CID (expressed as time duration and number of visits) once attained, and (3) the ability of baseline disease characteristics, treatment, and an early robust response to predict attainment of CID. Additionally, we characterize the patterns of disease status over the entire followup period for all patients at all visits.
MATERIALS AND METHODS
The original TREAT study was conducted by 15 Childhood Arthritis and Rheumatology Research Alliance (CARRA) sites in the United States. Results have been published elsewhere10.
Patients
Eighty-five patients aged 2 to 16 years with clinically active poly-JIA (RF-positive or negative) of less than 12 months in duration were enrolled in the original trial; data from these same patients were used for the present analysis. Other categories of JIA were excluded to increase the homogeneity of the study population. At baseline, patients had no prior therapy with the exception of brief oral (or intraarticular) steroids, or methotrexate (MTX; started no earlier than 6 weeks prior to enrollment). As presented in the report of the original trial, both groups were well matched on demographic and disease characteristics at baseline, except that the MTX group had a statistically higher number of active joints and a higher erythrocyte sedimentation rate (ESR). However, neither of these variables affected the likelihood of achieving the primary endpoint of CID at 6 months.
Study design and treatments
TREAT was a prospective, randomized, double-blind, placebo-controlled study that compared the efficacy of 2 aggressive treatment regimens for achieving CID within 6 months of baseline visit (primary endpoint). Patients were randomized in a 1:1 ratio. Arm 1 consisted of open-label subcutaneously (SC) administered MTX at a dose of 0.5 mg/kg/wk (maximum 40 mg/wk), blinded etanercept administered SC at a dose of 0.8 mg/kg/week (maximum 50 mg), and oral blinded prednisolone daily at 0.5 mg/kg/day (maximum 60 mg/day tapered to 0 mg over the first 4 months of therapy). For clarity, Arm 1 is referred to as the MEP arm. Arm 2 medications included open-label SC administered MTX, as in the MEP arm, blinded placebo-etanercept administered SC every week and daily blinded placebo-oral prednisolone tapered to 0 over 4 months. Arm 2 is referred to as the MTX arm. All patients received oral folic acid 1 mg/day and were allowed use of a single nonsteroidal anti-inflammatory drug as concomitant therapy. Up to 2 intraarticular corticosteroid injections within 2 weeks after the baseline visit and again after 6 months of study were allowed. No other antiinflammatory or antirheumatic therapies were allowed during the 1-year study participation.
Study procedures
Study visits occurred at screening, baseline, 1, 2, 4, 5, 6, 7, 8, 10, and 12 months. All joint examinations were done by certified joint assessors who were unaware of which treatment the patient was receiving (blinded joint assessment). At each visit after baseline, patients were assessed for ACR Pediatric response level, CID, and flare of disease.
There were interim treatment assessments at 4 and 6 months that influenced treatment allocation. At the 4-month visit, patients who failed to achieve an ACR Pediatric 70 were switched to open-label MEP medications. Similarly, patients who did not achieve CID at the 6-month visit were switched to open-label MEP medications.
Endpoints
CID served as the primary endpoint for this analysis. CID was strictly defined as (1) no joints with active arthritis; (2) no fever, rash, serositis, splenomegaly, or generalized lymphadenopathy attributable to JIA; (3) no active uveitis; (4) ESR in the normal range in the laboratory where tested; and (5) a physician’s global assessment of disease activity score of 011. At the 12-month visit patients were assessed for clinical remission on medication (CRM), defined as CID for a period of 6 consecutive months.
In the current study we calculated statistical descriptors of the elapsed time of receiving aggressive therapy prior to the initial observation of CID and durability of this clinical state. We estimated the ability of selected baseline disease characteristics, achievement of the ACR Pediatric 70 at 4 months, and treatment to predict CID at any time over the entire 1 year study period, as well as durability of CID.
Statistical considerations
Using data from the TREAT study, we performed descriptive statistics, Mann-Whitney U test, repeated measures logistic regression, Fisher’s exact probability test, and Cochran-Mantel-Haenszel and Pearson’s chi-square tests. Where appropriate, p values were adjusted for multiple tests of hypothesis using the family-wise Bonferroni correction.
The protocol specified that patients who failed to meet intermediary endpoints at Month 4 or Month 6 were to switch to open-label MEP for the remainder of the study.
For this analysis we defined the observation period as the time (in days) from the baseline visit until the patients’ last visit, whether or not they continued to take blinded or open-label medications. Cumulative time in CID was calculated as the time difference (in days) between the date of the visit at which the patient was observed to be in CID until the date at which he/she was observed to no longer be in CID, or completed the study. We assumed that if a patient was found to be in CID at 2 consecutive visits, the patient had CID on all days between these visits (at which no examination was done). If a patient was found to meet criteria for CID at a visit, but lost CID status at the next visit, then he/she was considered to have been in CID until observed to have active disease. Patients found to be in CID only on the final day of the study contributed a single day of CID.
RESULTS
Time of observation by treatment arms
Patients randomized to MEP initial therapy were observed for a median of 335 days (range 98–350) and those initially starting MTX were observed for a median of 331 days (range 32–357). Overall 58/85 patients (68%) achieved CID during this 12-month study. Table 1 shows the total number and percent of patients who achieved CID at any time during the study, elapsed days to achieve CID from baseline, and the total days and percent of total days in CID, based upon the group to which they were randomized. Those randomized to MEP tended to achieve CID earlier than those in the MTX group (median of 168.5 and 192 days, respectively), but this difference was not significant (p = 1.0). Similarly, median and percent of days spent in CID tended to be higher among those started on MEP compared to MTX starts. A total of 12 patients (14%; 9 randomized to the MEP group and 3 to MTX) achieved CRM, indicating continuing CID for 6 consecutive months (p = 0.53). A total of 27 patients (12 who started in the MEP group and 15 who started in the MTX group) failed to achieve CID (p = 0.362).
Percent of all randomized patients who achieved CID at any visit, elapsed time to the first occurrence, and total time spent in CID, by initial treatment arm.
Because Table 1 presents results based upon the treatment arm to which the patient was randomized rather than the treatment the patient was actually receiving at the time CID was observed, further clarification is provided in Table 2. This table presents the numbers and percent of patients who remained in the arm to which they were randomized for the entire study (blinded therapy), whether they achieved CID under blinded conditions and whether they achieved CID after switching to open-label MEP. The proportion of patients completing the entire 12-month study under blinded conditions was statistically significantly higher for the MEP group than for the MTX group (p = 0.033). The proportion of patients who achieved CID while in the blinded MEP group is higher than those in the MTX group, but the difference was not significant (p = 0.338). Half of those randomized to MEP (21 of 42) entered the open-label phase, and 11 of these 21 (52.3%) attained their first occurrence of CID in the open-label phase. Twenty-nine of the 43 (67.4%) randomized to MTX entered the open-label phase and 17 of those (58.6%) attained their first occurrence of CID after switching to open-label MEP medications. Initial blinded treatment did not significantly influence whether CID was achieved during the open-label phase. When data were combined from the blinded and open-label phases, CID was observed at 154 of 481 visits (32%) while patients were receiving MEP, compared to 45 of 203 visits (22%) while receiving MTX alone. The percentages of those who failed to achieve CID in either the blinded or open phase were not significantly different between treatment groups (p = 0.64) although the power was limited owing to small sample size (Table 1).
Numbers and percent of patients achieving or failing to achieve CID while undergoing blinded therapy.
Predictors of CID. Initial treatment as a predictor of the proportion of visits in CID
The 42 patients initially randomized to MEP had twice the percentage of visits at which CID was observed compared to the 43 who were initially randomized to the MTX group (23.6% vs 12.5%).
Disease duration prior to enrollment as a predictor of CID
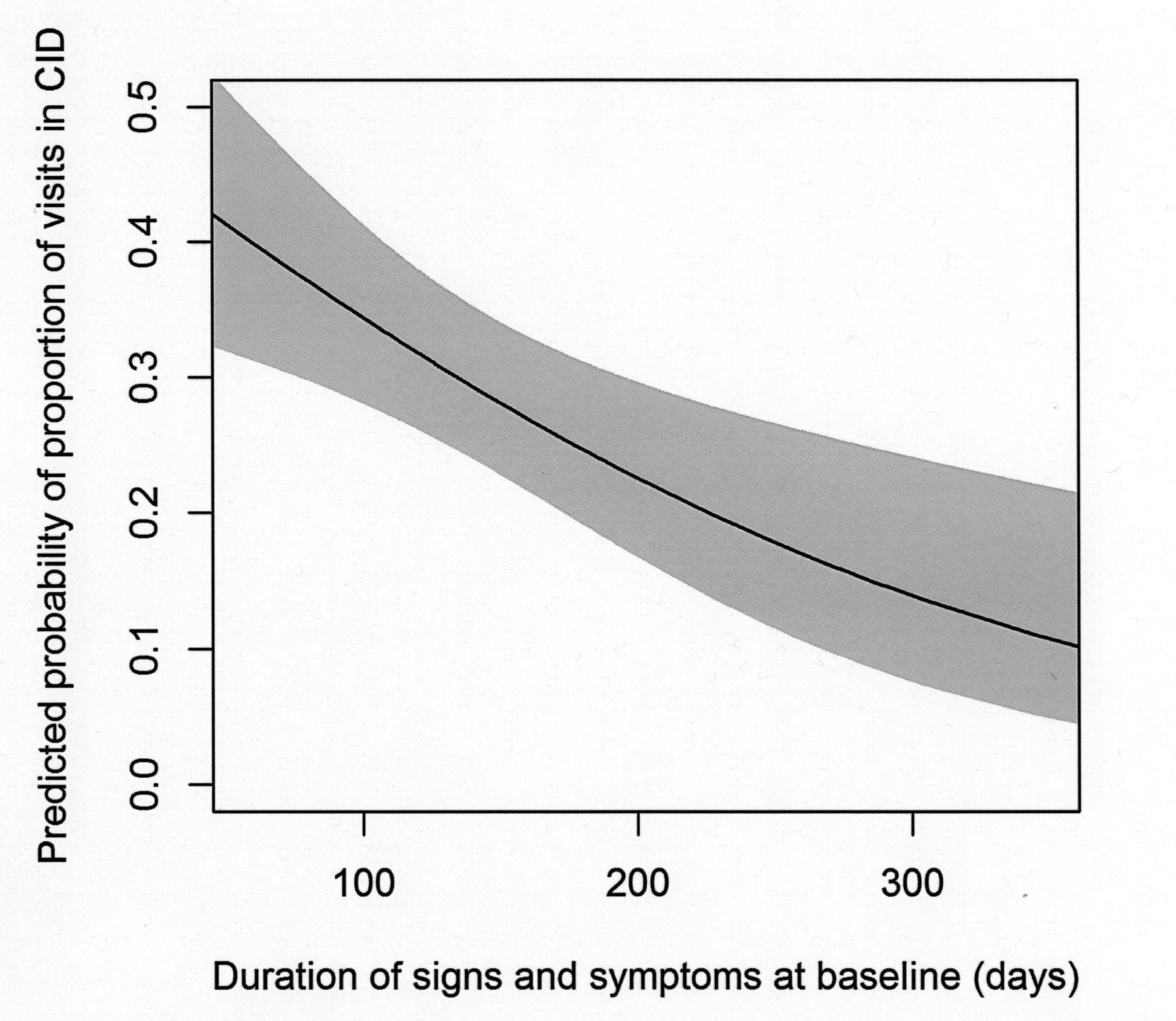
Logistical analyses on the total study sample of 85 patients identified the patient disease duration at baseline as a significant predictor. Patients with shorter duration of disease showed significantly greater percentage of visits in CID compared to those with longer disease duration (Figure 1, p = 0.002)

Repeated measures logistic modeling results showing predicted probability of proportion of inactive disease visits over the study decrease as the duration of disease prior to initiation of aggressive therapy increases; p = 0.002.
Achievement of an ACR Pediatric 70 response at 4 months as a predictor of CID
Achievement of a response of at least ACR Pediatric 70 by 4 months was a strong predictor for achievement of CID during the course of the study (Table 3). The 49 patients who demonstrated this early, robust response to aggressive therapy at 4 months were found to be in CID at 58% of their followup visits. In contrast, the 30 patients who failed to achieve this intermediary endpoint were found to be in CID at only 14.2% of followup visits (OR = 7.95, 95% CI 4.93–12.83; p < 0.0001).
Numbers and percent of patients achieving or failing to achieve CID while undergoing open-label therapy.
ACR Pediatric 70 at 4 months as a predictor of clinically inactive disease after 4 monthsa.
No other baseline disease characteristics analyzed, including antinuclear antibody and RF status, active joint count, and ESR (which were statistically higher in the MTX arm) were found to predict the number or percentage of visits in CID (data not shown) over the 12-month followup.
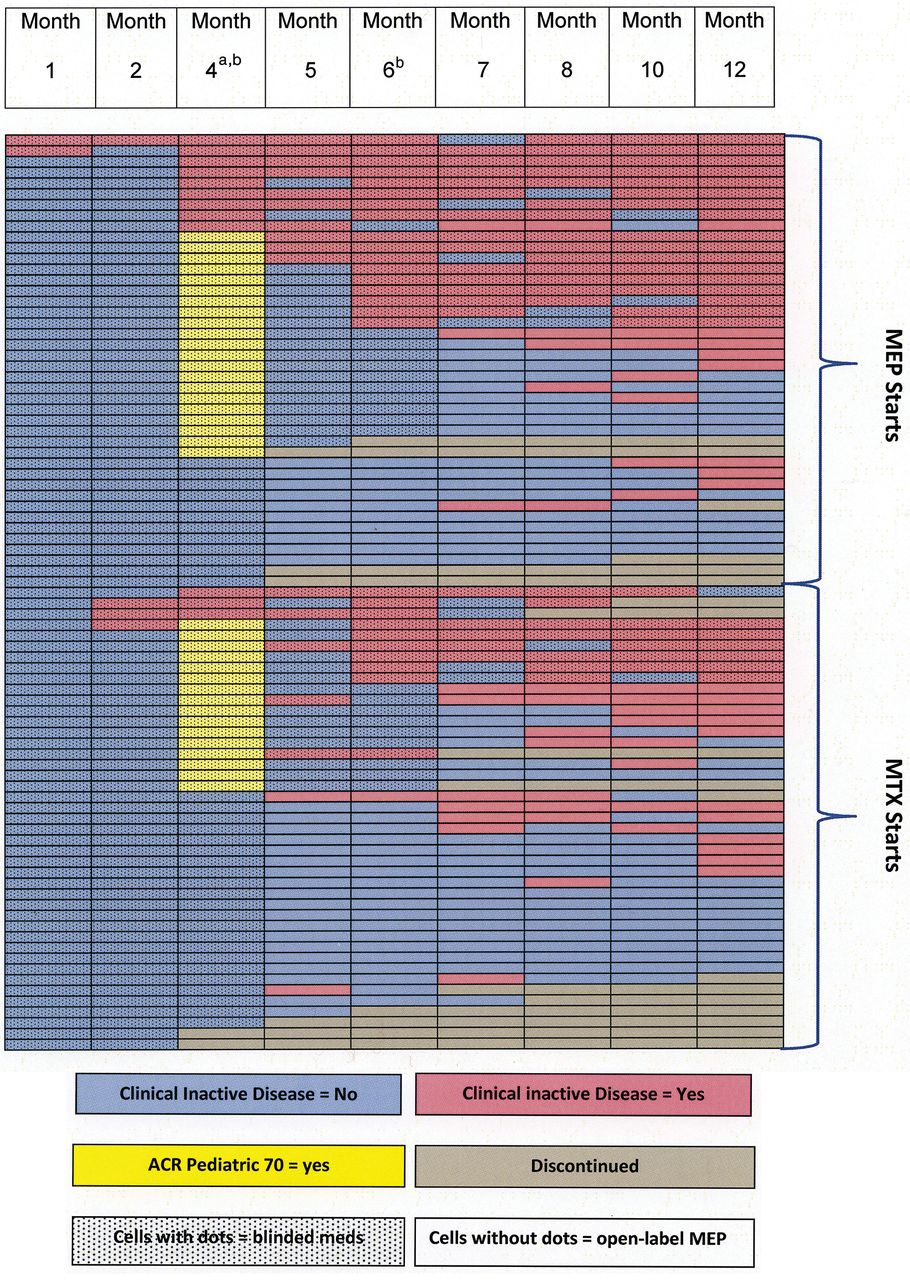
Figure 2 is a visual and more granular representation of the disease course for each patient over the 1-year study and provides a more detailed view of the disease status over the entire study duration for each patient, what medications the patient was receiving when CID occurred, and whether the medications were still being given under blinded conditions. Figure 2 demonstrates the importance of achieving the intermediary endpoint of an ACR Pediatric 70 by 4 months. Figure 2 also shows that once CID was achieved, the likelihood was high that this state of inactivity would persist. Exceptions did exist, but the exacerbation was typically mild in the 32 patients who did not continue CID at every visit after achieving CID. Only 3 of the 58 patients (5.2%) who achieved CID met the criteria for disease flare10 (as defined a priori in the protocol) following achievement of CID. The other 29 patients lost the state of CID owing to minor increases in joint count, ESR, or physician global assessment (PGA). Specifically: 11 patients had 1–2 active joints; 6 had 1–4 active joints plus a PGA of 1; 4 had minor increases in ESR; 5 had PGA change from 0 to 1; 2 had 4–6 joints; and 1 had 1 active joint, an increase in ESR and a PGA of 2.
{kind=link}
{kind=link}
Disease patterns in all patients during 1 year of study. Patients were not assessed at months 3, 9, or 11 of the study. aPatients were assessed for achievement of an ACR Pediatric 70 response at the Month 4 visit only. bPatients who failed to reach an ACR Pediatric 70 at the 4-month visit or clinically inactive disease by 6 months were given open-label MEP until the end of the study or discontinuation. ACR: American College of Rheumatology; MEP: Methotrexate, blind etanercept, blind prednisolone tapered to zero by 17 weeks.
Joint injections
Five patients in each treatment arm had joint injections within 2 weeks of the baseline visit. Of these, 2 patients had 1 joint injected, 5 had 2 joints injected, 1 had 3 joints injected, and 2 had 4 joints injected. Because of disease severity and lack of ambulation, a protocol waiver was granted for the 3 patients who had more than 2 joints injected at baseline. There was no association between having joint injections, or the number of joint injections, and later achievement of ACR Pediatric 70 response or CID.
Four patients had joint injections after the primary outcome was assessed — 3 at the 6-month visit (1 had 1 joint injected and 2 had 2 joints injected), and 1 at the 7-month visit (1 joint injected). All 4 were switched to open-label medications, 2 achieved CID at the next visit, and 2 never achieved CID.
Patients who did not achieve CID at any time in the study
Twenty-seven patients (32%) did not achieve CID at any time during our study. These patients did not differ from those patients who achieved CID at baseline in median joint count, percent RF positivity, or median PGA of disease severity. However, the patients not achieving CID tended to have less antinuclear antibody positivity (59% vs 74%) and a longer median time to treatment (180 days vs 120 days).
Discussion
In contrast to the analysis of the original TREAT study, the present analysis focuses on the time needed to achieve CID, duration of CID, and the strength of the predictors of achieving CID. Further, this analysis quantifies the percentage of total observation time spent in CID for each treatment group.
The importance of early aggressive treatment and the strong predictive ability of an early, robust response (ACR Pediatric 70) for achieving CID are underscored by these data. Therefore, patients who show an early, marked favorable response should likely continue aggressive therapy because CID often takes 6 months or longer to achieve.
Although both treatment arms are considered aggressive, with MTX given SC (at a dose of 0.5 mg/kg/week) in both, the more aggressive arm (MEP) showed a trend toward increasing the likelihood of achieving and maintaining CID.
The children with poly-JIA enrolled in TREAT were severely affected by their disease, with a large proportion having positive RF and high physician global assessments of disease activity as reported10. Still, CID began to appear in some patients as early as 1 month after therapy initiation, and high percentages of patients in both groups achieved CID at some point during the 12-month followup period. However, the fact that nearly one-third of patients did not achieve CID at any time during this study with early, aggressive therapy underscores the need for rapid identification of those patients who will need therapies different from those used in our study.
Our original analysis of the TREAT data did not reveal strong clinical predictors of the eventual achievement of CID, with the exception of disease duration at baseline. The current analysis substantiates that finding. RF positivity has often been considered a predictor for a poorer prognosis. While this may indeed be valid for studies with less rigorous endpoints, we were unable to confirm this hypothesis when using time spent in CID as the outcome over the 12-month study.
Attainment of CID did not guarantee its persistence during followup, even during continuation of therapy. However, patients who achieved CID and then no longer met criteria at a followup visit typically experienced only a mild worsening of disease. Figure 2 provides visual representation of the conclusion that once CID is achieved, further occurrences of it are likely, even in the setting of a strict definition of CID and the use of blinded joint assessors at every visit.
Interestingly, the attainment of CID was more likely to occur in children randomized to MEP, versus those given the same drugs in an open-label manner later in the trial, because of failure to meet intermediary endpoints. The addition of MEP at 4 or 6 months into the study did not result in the same level of response over the next 6 months, as those same medications yielded if started initially. While this finding may have resulted from selection bias (difficult-to-treat disease), it may represent a decrease in the likelihood of response due to longer disease duration at the time of assessment in the open-label MEP phase or the presence of an immunologic window of opportunity.
There was a trend of patients treated with MEP to spend longer periods of time in CID, which is clinically relevant for estimating prognosis. If children treated with early aggressive therapy follow a disease trajectory pattern similar to adults with RA treated with early aggressive therapy, these time periods of no discernible disease should bode well for longterm outcome.
Our study has a number of limitations including the small number of participants. Our failure to find marked trends that were statistically significant is likely due to small sample sizes and the very strict definition of CID. Results of inferential statistical tests presented in this work are considered exploratory in nature. We did not perform formal sample size calculations or posthoc power estimates. Therefore, it is possible that some of the nonsignificant comparisons were a result of limited sample size and may represent type II errors. The treatment period of observation was limited to 12 months when the true benefits of early control of disease may require longer-term followup studies. Such an effort involving patients who participated in the original trial to assess disease course has recently been completed but has yet to be published. While the strictly controlled environment of a randomized trial minimizes potential biases, a trial setting is quite different from the “real-world” and the external validity of trial conclusions is always a concern. Thus, similar results may not be observed in patients followed under real-world conditions rather than during a trial. Our study was not designed to determine the role or necessity of prednisolone at the initiation of aggressive therapy, or the probability of attaining CID with SC MTX alone among those who did not achieve an ACR Pediatric 70 response at 4 months and were therefore switched to open-label MEP for the remainder of the study. Both of these questions require further investigation.
Results of the TREAT study suggest that patients with poly-JIA treated with aggressive therapy as early as possible in their disease course, and who demonstrate an early, robust response by 4 months will likely have a more favorable prognosis than those in whom aggressive therapy is delayed. These findings underscore the need for increased awareness about JIA among physicians and other practitioners who first encounter these patients to decrease time to presentation, evaluation, diagnosis, and initiation of aggressive therapy.
Acknowledgments
The authors thank Nora Singer, MD, for her idea of the format of Figure 2 of disease states.
Footnotes
-
Supported by US National Institutes of Health Grants: 1RO1 AR049762-01A2, 3R01AR049762-04S1, P60 AR047784-07, the Howe Endowment for Juvenile Rheumatoid Arthritis Research. Support for medication and placebo for the original trial from Amgen.
- Accepted for publication February 28, 2014.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.