
Abstract
Objective. To investigate the performance of the new remission criteria for rheumatoid arthritis (RA) in daily clinical practice and the effect of possible misclassification of remission when 44 joints are assessed.
Methods. Disease activity and remission rate were calculated according to the Disease Activity Score (DAS28), Simplified Disease Activity Index (SDAI), Clinical Disease Activity Index (CDAI), and a Boolean-based definition for 1402 patients with RA in Keio University Hospital. Characteristics of patients in remission were investigated, and the number of misclassified patients was determined — those classified as being in remission based on 28-joint count but as nonremission based on a 44-joint count for each definition criterion.
Results. Of all patients analyzed, 46.6%, 45.9%, 41.0%, and 31.5% were classified as in remission in the DAS28, SDAI, CDAI, and Boolean definitions, respectively. Patients classified into remission based only on the DAS28 showed relatively low erythrocyte sedimentation rates but greater swollen joint counts than those classified into remission based on the other definitions. In patients classified into remission based only on the Boolean criteria, the mean physician global assessment was greater than the mean patient global assessment. Although 119 patients had ≤ 1 involved joint in the 28-joint count but > 1 in the 44-joint count, only 34 of these 119 (2.4% of all subjects) were found to have been misclassified into remission.
Conclusion. In practice, about half of patients with RA can achieve clinical remission within the DAS28, SDAI, and CDAI; and one-third according to the Boolean-based definition. Patients classified in remission based on a 28-joint count may have pain and swelling in the feet, but misclassification of remission was relatively rare and was seen in only 2.4% of patients under a Boolean definition. The 28-joint count can be sufficient for assessing clinical remission based on the new remission criteria.
- RHEUMATOID ARTHRITIS
- REMISSION CRITERIA
- 44 JOINTS
- VERIFICATION
Therapeutic developments over the past several decades in the treatment of rheumatoid arthritis (RA) have made remission an achievable goal. While different remission criteria had been used, new criteria have recently been presented by the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR)1: the index-based criteria defined as a Simplified Disease Activity Index (SDAI) of ≤ 3.3 and a Boolean-based definition requiring 4 criteria to be ≤ 1 [patient global assessment (PGA; in cm), swollen and tender joint counts (SJC, TJC), and C-reactive protein (CRP; in mg/dl)]. Definitions for clinical practice were also proposed: a Clinical Disease Activity Index (CDAI) level of ≤ 2.8 and a Boolean-based definition requiring 3 criteria to be ≤ 1, eliminating the CRP. In the past, the most widely used criteria were the Disease Activity Score (DAS) and DAS28, with 44 and 28 joints assessed, respectively. While the 44-joint count is more comprehensive, the 28-joint count correlates well with the full joint count2,3,4 and is easier to assess and more convenient in daily practice; the newly suggested criteria are also based on a 28-joint count. However, the 28-joint count excludes evaluation of ankle and foot joints, potentially leading to misclassification of patients to remission status, particularly if the patient has disease activity only in the ankles and feet.
While van Tuyl, et al5 did report that residual disease activity in the forefeet had a limited effect on outcome using a 38-joint count, it remains unclear whether using only a 28-joint count is sufficiently accurate in evaluating remission, because the van Tuyl team did not assess activity in the ankles. We assessed the performance of the new remission criteria in daily clinical practice and evaluated the effects of possible misclassification of remission on their performance when 44 joints are assessed instead of 28.
MATERIALS AND METHODS
All patients with RA in Keio University Hospital were evaluated cross-sectionally in the period December 2011 to February 2012. Joint counts were assessed by 6 rheumatologists, all of whom had at least 10 years’ experience. The 44-joint count includes ankle (n = 2), metatarsophalangeal (n = 10), sternoclavicular (n = 2), and acromioclavicular (n = 2) joints, as well as the usual 28-joint count.
Findings for laboratory data included CRP, erythrocyte sedimentation rate (ESR), and matrix metalloproteinase-3 (MMP-3). Patient pain, patient global assessment (PGA), and physician global assessment (PhGA) were measured on a visual analog scale ranging from 0 to 100 mm. A Health Assessment Questionnaire (HAQ) was filled out by each patient.
We first classified patient disease activity into states of remission and low, moderate, and high activity, based on DAS28, SDAI, and CDAI values, and then examined the number of criteria that were satisfied under a Boolean-based definition. We also assessed the characteristics of patients in remission according to each definition and then evaluated the number of misclassified patients — those classified into remission based on a 28-joint count but as nonremission based on a 44-joint count for each definition criterion. In addition, for patients with an involved joint count ≤ 1 in the 28-joint count but > 1 in the 44-joint count (meaning they could have been misclassified into remission under the Boolean definition) who were not classified into remission, variables that prevented them from being misclassified were also investigated.
Comparisons of mean values were performed using Student’s t test with IBM SPSS version 20.0 (IBM Corp.).
RESULTS
Characteristics of all study patients and those in remission for each definition
Of the 1449 patients with RA in our hospital, 47 were excluded because of insufficient data, resulting in a total of 1402 patients (83% female) included in study analysis. Mean patient age was 60.1 years, mean disease duration 10.9 years, and mean DAS28 was 2.8. About half the patients were treated with a biologic agent (Table 1).
Characteristics of all patients studied and patients in remission according to SDAI, CDAI, and Boolean-based definition. Data are expressed as mean (SD), unless otherwise indicated.
Characteristics of patients in remission according to DAS28, SDAI, and CDAI values as well as Boolean-based criteria are shown in Table 1. The remission rates were 46.6% in DAS28, 45.9% in SDAI, 41.0% in CDAI, and 31.5% under a Boolean definition. The mean value of HAQ score was significantly better in patients in remission under the Boolean definition than in those deemed to be in remission based on the other definitions.
Comparison of characteristics of patients in various remission states by definition
We compared the characteristics of patients whose remission status varied among the 4 sets of remission criteria (Table 2). Patients classified into remission based only on the DAS28 showed relatively low ESR but higher PGA values and SJC than those classified into remission based on the other definitions, while those classified into nonremission using only DAS28 showed relatively high ESR. Although few patients were classified into remission only by the Boolean definition, their mean PhGA was greater than their mean PGA score.
Comparison of characteristics of patients in various remission states stratified by definition.
Possible misclassification with assessment of 44 joints instead of 28 joints
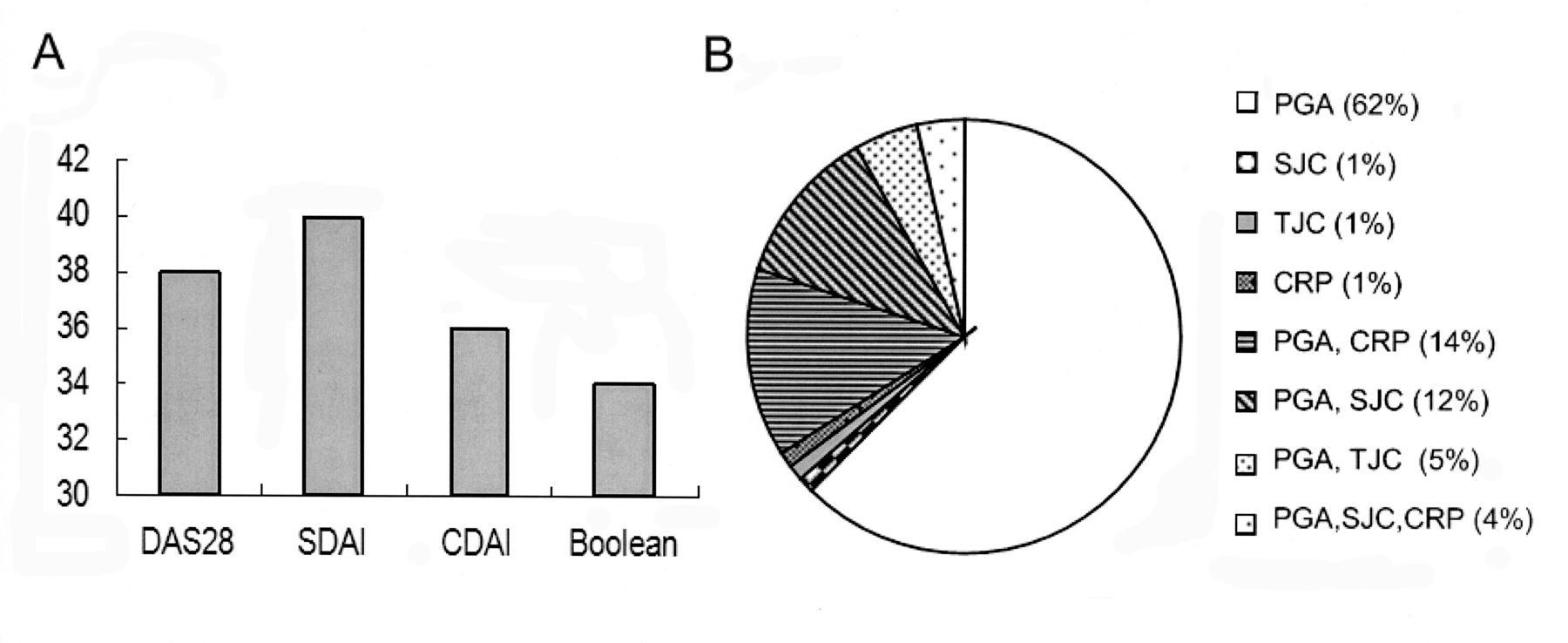
We then investigated the effect of possible misclassification into remission on the performance of each remission definition when 44 joints were assessed instead of the 28-joint count. The numbers of patients classified into remission using the 28-joint count but as nonremission with the 44-joint count were 38, 40, 36, and 34 under the DAS28, SDAI, CDAI, and Boolean definitions, respectively, which means the possible remission rate would be 43.9%, 43.1%, 38.4%, and 29.0% according to the 44-joint count. Although the effect of possible misclassifications on performance was smallest using the Boolean definition, the difference was modest (Figure 1A).

{kind=link}
A. Number of patients classified as “in remission” in the 28-joint count but as “nonremission” when 44 joints were assessed. This number was smallest under a Boolean definition, but the difference was modest. B. Variables preventing patients with ≤ 1 involved joint in the 28-joint count but > 1 in the 44-joint count from being misclassified as “in remission.” Almost all reasons (97%) included patient global assessment (PGA). DAS28: 28-joint Disease Activity Score; SDAI: Simplified Disease Activity Index; CDAI: Clinical Disease Activity Index; SJC: swollen joint counts; TJC: tender joint counts; CRP: C-reactive protein.
A total of 119 patients (8.5% of all subjects) had ≤ 1 involved joint in the 28-joint count but > 1 in the 44-joint count, indicating the potential for misclassification into remission using the Boolean definition. However, only 34 of these 119 patients (2.4% of all subjects) were actually misclassified into remission, which was averted largely due to the presence of high PGA (45%), high SJC (1%), high TJC (1%), high CRP (1%), or a combination of several findings (24%) (Figure 1B). Given these findings, the remission rate could have potentially decreased from 31.5% to 29.0% using a Boolean definition when 44 joints were assessed.
DISCUSSION
Our study investigated effects of possible misclassification of remission on the performance of new ACR/EULAR remission criteria when 44 joints are assessed instead of 28, and we found that misclassification was relatively rare and was seen only in 2.4% of patients under a Boolean definition.
Although assessment of all joints is clearly required in a patient assessment, a 28-joint count has frequently been used because it has been recognized to provide as much information as a full joint count with considerably greater feasibility. However, there should be a compromise between comprehensiveness and feasibility6, and several groups have studied the residual disease activity in feet and ankles of patients in remission using a reduced joint count. Landewé, et al showed that remission defined by DAS28, which excludes ankles and feet, is inferior to the original DAS definition because of residual swelling and tenderness in the ankles and feet7. Kapral, et al compared the extended joint count with the limited joint count in DAS28 and SDAI, noting a negligible difference in findings, because other components of remission criteria would be higher in patients with foot joint involvement, helping to avoid misclassification8. In our study, we noted only a modest effect of possible misclassification into a remission category on the performance of the provisional ACR/EULAR remission criteria. While 8.5% of patients had ≤ 1 involved joint in a 28-joint count, but > 1 in a 44-joint count, only 2.4% were misclassified into remission under the Boolean-based definitions, mainly due to PGA values. Reinforcing the findings of the ACR/EULAR remission task force in their development of these new criteria that the effect of missing residual disease activity in the ankles and feet appeared to be limited because patients with activity in those joints showed increased levels in other measures in the definition, we demonstrated here that the 28-joint count can be sufficiently accurate in assessing remission status based on Boolean definition criteria. However, whereas the disease duration of our study patients varied considerably, Wechalekar, et al examined 123 patients with RA who had synovitis symptoms for less than 24 months and reported that remission criteria using 28-joint count did not adequately identify the resolution of foot synovitis9. This should be confirmed in a large population in a future study.
We also observed that 46.6%, 45.9%, and 41.0% of patients with RA could be deemed to be in remission using DAS28, SDAI, and CDAI values, respectively, with 31.5% remaining valid even using a Boolean-based definition. The remission rates with SDAI and CDAI were quite similar to that under DAS28 and were higher than values in other reports5,10,11. We believe this discrepancy exists because about half of our patients were treated with biologic agents, which can lead patients not only into remission but into a deep remission. While the prevalence of clinical remission in patients with RA after 6 months of treatment with anti-tumor necrosis factor (TNF) agents was previously reported to be 27% in DAS28 and 6% under Boolean definitions12, we noted that patients received various biologic agents in our study, i.e., 65% were receiving anti-TNF, 26% tocilizumab, and 9% abatacept.
Some patients were classified into the remission category based on only DAS28 or Boolean criteria. Reflecting the marked difference in the formulas between the DAS28 and SDAI, CDAI, and Boolean definitions, patients who were classified into remission based only on DAS28 showed relatively low ESR but higher values for PGA and SJC than those classified into remission based on the other definitions, while those classified as being in nonremission based only on DAS28 showed relatively high ESR. Moreover, while Studenic, et al reported that pain is the most important determinant in the PGA whereas it is mostly joint swelling in the PhGA13, in our study the mean PhGA of patients classified into remission based only on Boolean definitions was found to be greater than the mean PGA, and interestingly, this phenomenon was noted only in that particular group. The relatively low number of patients in this group, however, hampered our investigation, and future studies should therefore assess this matter in greater detail.
Several limitations to our study warrant mention. First, we assessed remission status cross-sectionally at 1 timepoint. It is known that there are patients with predominant foot involvement who could be underestimated in the 28-joint count, as reported by Bakker, et al14, and because the aim of sustained remission is to achieve little or no radiographic and functional deterioration, we need to also examine structural and functional outcomes under 44-joint counts longitudinally. Second, all data used in this study were obtained from a single hospital in Japan. While we are confident that our patients are representative of those in other clinics nationally, because our hospital is one of the biggest rheumatology centers in Japan, the high rate of use of biologic agents might hinder generalizations about the results.
In daily clinical practice, roughly half of patients with RA can be deemed to be in a state of clinical remission based on DAS28, SDAI, and CDAI values, while one-third can be so classified under a Boolean-based definition. Patients deemed to be in remission based on a 28-joint count may show pain and swelling in the feet, but misclassification was relatively rare in our study and was observed in only 2.4% of patients under a Boolean definition. The 28-joint count seems to be sufficient for assessing remission using the ACR/EULAR remission criteria.
- Accepted for publication April 5, 2013.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.