
Abstract
Objective. The role of follicular Th (TFH) cells remains unclear in the pathogenesis of ankylosing spondylitis (AS). Our study examined the frequency of different subsets of circulating CXCR5+CD4+ T cells in patients with AS before and after receiving therapy.
Methods. Percentages of peripheral blood inducible costimulator (ICOS)+, programmed death 1 (PD-1)+, and interleukin 21 (IL-21)+ CXCR5+CD4+ T cells in 26 patients with AS and 12 healthy controls (HC) were examined by flow cytometry, and the disease activity of individual patients was measured by Bath AS Disease Activity Index (BASDAI). The concentrations of serum IL-21, IgG, IgA, IgM, and C-reactive protein (CRP) were examined and the values of erythrocyte sedimentation rate (ESR) were measured. The potential association among these measures was analyzed.
Results. In comparison with that in HC, significantly increased percentages of CXCR5+CD4+, CXCR5+CD4+PD-1+, and CXCR5+CD4+IL-21+, but not CXCR5+CD4+ICOS+ and PD-1+ICOS+CXCR5+CD4+ T cells, and elevated concentrations of serum IL-21 were detected in patients with AS (p = 0.001, p = 0.012, p < 0.001, p = 0.233, p = 0.216, p < 0.001, respectively). Treatment with meloxicam, thalidomide, and etanercept for 1 month significantly reduced percentages of IL-21+CXCR5+CD4+ T cells and concentrations of serum IL-21 (p < 0.001, p < 0.001, respectively), accompanied by significantly minimized disease activity in drug responders, but not in the drug nonresponders. Further, percentages of IL-21+CXCR5+CD4+ T cells were positively correlated with BASDAI in patients (r = 0.6, p = 0.0012) and in the drug-responders 1 month after treatment (r = 0.68, p = 0.005), while the percentages of PD-1+CXCR5+CD4+ T cells were negatively correlated with BASDAI (r = −0.58, p = 0.0018).
Conclusion. These data suggest that IL-21+CXCR5+CD4+ T cells may be associated with development of AS and that the frequency of IL-21+CXCR5+CD4+ T cells may be a biomarker for evaluation of disease activity and drug responses in patients with AS, particularly in drug-responding patients.
- FOLLICULAR HELPER T CELLS
- INTERLEUKIN 21
- ANKYLOSING SPONDYLITIS
- DISEASE ACTIVITY
- THERAPEUTIC RESPONSE
Ankylosing spondylitis (AS) is a severe autoimmune disease characterized by chronic inflammation in the spine and sacroiliac joints, leading to inflammatory back pain, peripheral arthritis, and enthesitis. Patients with AS usually suffer from chronic pain and stiffness in the spinal and peripheral joints during their second to third decades, and from social and psychological burdens1. AS is estimated with a prevalence of about 0.2%–0.3% in China and predominantly affects young adult males. Currently, there is no effective and specific therapy for patients with AS, which continually progresses, leading to a high rate of disability in those patients. Therefore, coming to a greater understanding of the pathogenesis of AS is of great significance.
Although the precise factors that initiate AS are unclear, previous studies have shown that genetic factors may play an important role in the pathogenesis of AS2. Indeed, HLA-B27 and other non-MHC genetic variants, such as endoplasmic reticulum aminopeptidase (ERAP1), are associated with an increased risk for the development of AS3,4. Further, autoreactive T and B cells as well as natural killer (NK) cells may also contribute to the pathogenesis of AS. A high frequency of peripheral blood inflammatory Th1 and Th17 cells and high levels of serum cytokines, such as interferon-γ, interleukin 17 (IL-17), tumor necrosis factor-α (TNF-α), IL-6, and IL-23, accompanied by lower frequency of regulatory T cells (Treg), are detected in patients with AS5,6,7,8,9,10. Although there are few studies on the pathogenic role of B cells in AS, recent reports show that a high frequency of B cells and high levels of autoantibodies are present and associated with disease activity in patients with AS11,12,13. Indeed, treatment with rituximab, a monoclonal antibody targeting B cells, benefits patients with AS who have not been treated with anti-TNF-α14. These findings suggest that autoreactive B cells and autoimmune antibody responses may participate in the pathogenesis of AS and an imbalance of proinflammatory and antiinflammatory responses is associated with the development and progression of AS.
CD4+ T cells can differentiate into distinct lineages and have unique functions. Follicular Th (TFH) cells are a subset of CD4+ T cells and have been demonstrated to be crucial regulators of B cell differentiation, antibody production, and humoral immunity15. Although the identification of TFH cells remains controversial, TFH cells express chemokine (C-X-C motif) receptor 5 (CXCR5). A previous study has shown that CXCR5+CD4+ T cells share the functional property of TFH and has considered CXCR5+CD4+ T cells as TFH cells16. Further, TFH cells also express inducible costimulator (ICOS), programmed death 1 (PD-1), CD200, and IL-21 receptor as well as other cell surface markers and produce IL-21 and other cytokines17,18. Hence, TFH cells may also regulate other immune responses. Previous studies have shown that ICOS+ TFH cells positively regulate B cell differentiation, while engagement of PD-1 on TFH cells promotes negative signals that inhibit humoral immunity19,20. Studies indicate that a high frequency of CXCR5+CD4+ TFH and high levels of serum IL-21 are present in patients with autoimmune diseases, such as systemic lupus erythematosus, rheumatoid arthritis (RA), and Sjögren syndrome21,22,23,24,25,26. These findings suggest that TFH cells participate in the pathogenic process of these diseases. However, there is no information on whether CXCR5+CD4+ TFH cells are associated with the development of AS and what subsets of TFH cells are involved.
Currently, the therapies of patients with AS in China include nonsteroidal antiinflammatory drugs (NSAID), painkillers, steroids, immunosuppressants, and TNF-α blockers, as well as physical therapies. However, there is no information about how the treatments affect the frequency of different subsets of CXCR5+CD4+ TFH cells in patients with AS.
We examined the frequency of peripheral blood CXCR5+CD4+ T, ICOS+, PD-1+, or IL-21+ CXCR5+CD4+ T cells and the concentrations of serum IL-21 in 26 patients with AS, and 12 sex-matched and age-matched healthy controls before and 1 month after treatment. We analyzed the potential association between the percentages of different subsets of CXCR5+CD4+ T cells and disease activity in those patients. Our data indicate that a higher frequency of PD-1+CXCR5+CD4+, and IL-21+CXCR5+CD4+ T cells presented in patients with AS, but the percentages of IL-21+CXCR5+CD4+ T cells were reduced 1 month after treatment in the drug responders. The percentages of IL-21+CXCR5+CD4+ T cells were positively correlated with the disease activity, but the percentages of PD-1+CXCR5+CD4+ T cells were negatively correlated with disease activity in this population. Therefore, different subsets of CXCR5+CD4+ T cells have different regulatory functions in the pathogenesis of AS.
MATERIALS AND METHODS
Patients and controls
A total of 26 patients diagnosed with AS were recruited sequentially at the inpatient service of the First Hospital of Jilin University. Another 12 healthy controls (HC) matched by sex, age, and ethnicity were recruited. Individual patients with AS were diagnosed according to the 1984 modified New York criteria27. All patients met the criteria. Disease duration was defined as the interval from the time of symptom appearance to this study. No patient received NSAID, steroids, or other immunosuppressants from 1 month before their blood samples were collected. The disease activity of individual patients was measured for the Bath AS Disease Activity Index (BASDAI), as described28. The scores for each item ranged from 0 to 10, and high disease activity was defined as a BASDAI score ≥ 4. Individual subjects were excluded if they had RA, multiple sclerosis, type 1 diabetes, immunodeficiency, chronic inflammatory diseases, and recent infection. Written informed consent was obtained from individual patients, and the experimental protocol was approved by the Ethics Committee of the First Hospital of Jilin University.
After hospitalization, individual patients were treated orally with 15 mg meloxicam (Boehringer Ingelheim), 50 mg thalidomide daily (Changzhou Pharmaceutical Factory), and injected subcutaneously with 25 mg etanercept (Wyeth) every 2 weeks. In addition, 8 patients with severe back pain were treated with physical therapy. After 1-month treatment, drug responders were classified according to the ASAS20 (response criteria of the Assessment of SpondyloArthritis International Society)29.
Laboratory examinations
Fasting venous blood samples were obtained from individual subjects before and 1 month after treatment, and their sera were prepared. The number of white blood cells (WBC), erythrocyte sedimentation rate (ESR), and the concentrations of serum C-reactive protein (CRP), IgG, IgA, and IgM of individual subjects were measured by an analyzer (Siemens Healthcare Diagnostics Products GmbH) and ELISA using specific kits.
Stimulation of PBMC
Peripheral blood mononuclear cells (PBMC) were isolated from individual patients and HC by density-gradient centrifugation using Ficoll-Paque Plus (Amersham Biosciences). PBMC at 4×106/ml were cultured in 10% fetal calf serum RPMI-1640 (Hyclone) in U-bottom 24-well tissue culture plates (Costar, Corning Corp.) and stimulated with, or without, 50 ng/ml of phorbol myristate acetate and 2 μg/ml of ionomycin (Sigma) for 1 h, followed by culturing in the presence of Brefeldin A (10 μg/ml, GolgiStop, BD Sciences) for an additional 5 h. The cells were subjected to intracellular staining and flow cytometry analysis.
Flow cytometry analysis
Expression of HLA-B27 in T cells of individual subjects was characterized by flow cytometry analysis30. Briefly, PBMC were stained with FITC-anti-HLA-B27 and PE-anti-CD3 and subjected to flow cytometry analysis on a FACSCalibur (Beckton Dickinson). Human PBMC at 5×105/tube were stained with Alexefluor647-anti-CXCR5 and PE-CY7-anti-CD4, PE-anti-ICOS, and FITC-anti-PD-1 (BD PharMingen) in the dark at room temperature for 30 min. Control cells were stained with FITC-anti-IgG1, PE-anti-IgG1, PE-CY7-anti-IgG1, and Alexefluor-647-anti-IgG2b (BD PharMingen). Cells were gated on living lymphocytes and then on CD4+, and the frequency of different subsets of CXCR5+CD4+ T cells was analyzed using the FlowJo software (7.6.2)31.
Stimulated PBMC were harvested and stained in duplicate with Alexefluor647-anti-CXCR5 and PE-CY7-anti-CD4 for 30 min. Subsequently, cells were fixed, permeabilized, and stained with PE-anti-IL-21 (BD PharMingen). The frequency of IL-21+CXCR5+CD4+ TFH cells was determined by flow cytometry analysis. To ensure the quality of each batch of data during the longitudinal study, we used the same lot of antibodies from the identical manufacturers, according to the same protocol in a blinded manner.
Measurement of serum IL-21 by ELISA
The concentrations of serum IL-21 in individual patients and HC were determined by ELISA using a human IL-21 ELISA kit, according to the manufacturers’ instruction (Roche Diagnostics). Briefly, individual sera at 1:4 dilutions were subjected to ELISA analysis, and the concentrations of serum IL-21 in individual samples were calculated, according to the standard curve established using the recombinant IL-21 provided. The limitation of detection for IL-21 by the ELISA kit was 0.5 ng/l.
Statistical analysis
Data are expressed as the median and range or individual values. The difference between groups was analyzed by Mann-Whitney nonparametric U test using the SPSS 19.0 software. The relationship between variables was evaluated using the Pearson rank correlation test. Two-side p < 0.05 was considered statistically significant.
RESULTS
Patient characteristics
To determine the frequency of CXCR5+CD4+ TFH cells, a total of 26 patients with AS and 12 HC were recruited. Their demographic and clinical characteristics are shown in Table 1. The full spectrum of clinical indices for each patient is available from the authors on request. There was no significant difference in the distribution of age and sex between patients with AS and HC (Table 1). In comparison with that in HC, the majority of patients with AS were positive for HLA-B27 and had significantly greater numbers of WBC and higher ESR values. Further, patients with AS displayed variable values of BASDAI and significantly higher concentrations of serum CRP, IgA, and IgG, but not IgM.
The demographic and clinical characteristics of patients and healthy controls.
Higher percentages of peripheral blood TFH cells and higher concentrations of serum IL-21 in patients with AS
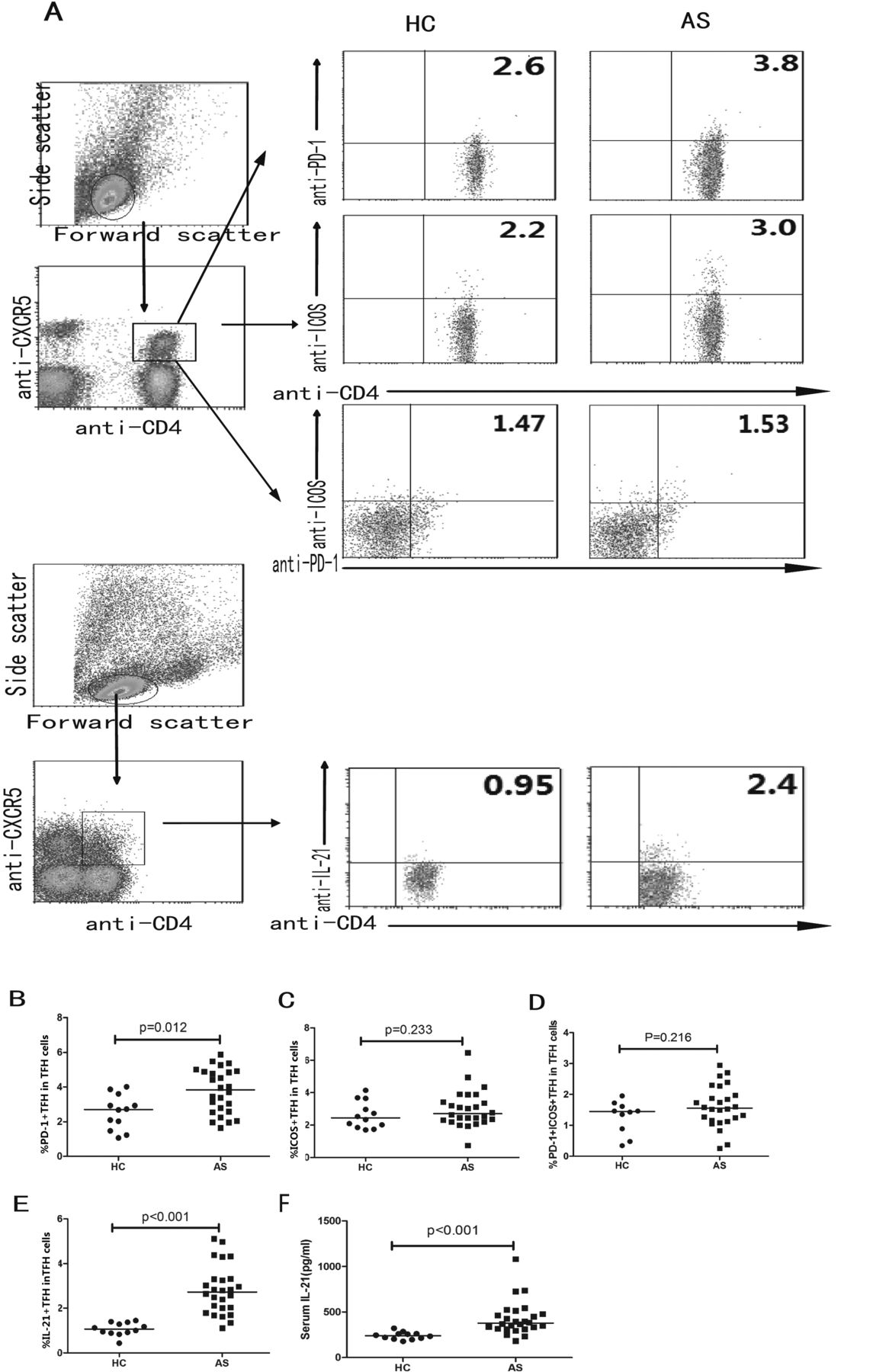
Next, we characterized the frequency of peripheral blood CD4+ T and CXCR5+CD4+ TFH cells by flow cytometry analysis and we found that there was no significant difference in the frequency of peripheral blood CD4+ T cells between the AS patient and HC groups (data not shown). However, the percentages of CXCR5+CD4+ T cells in patients with AS were significantly higher than those in the HC (p = 0.001, Figure 1). Further analysis revealed that percentages of peripheral blood PD-1+CXCR5+CD4+ or IL-21+CXCR5+CD4+, but not ICOS+CXCR5+CD4+ or PD-1+ICOS+CXCR5+CD4+, TFH cells were significantly higher in AS patients versus HC (p = 0.012, p < 0.001, p = 0.233, and p = 0.216, respectively, Figure 2). In parallel, concentrations of serum IL-21 in patients with AS were significantly higher versus HC (p < 0.001, Figure 2). Hence, a higher frequency of CXCR5+CD4+ TFH and higher concentrations of IL-21 are associated with the development of AS in this population.
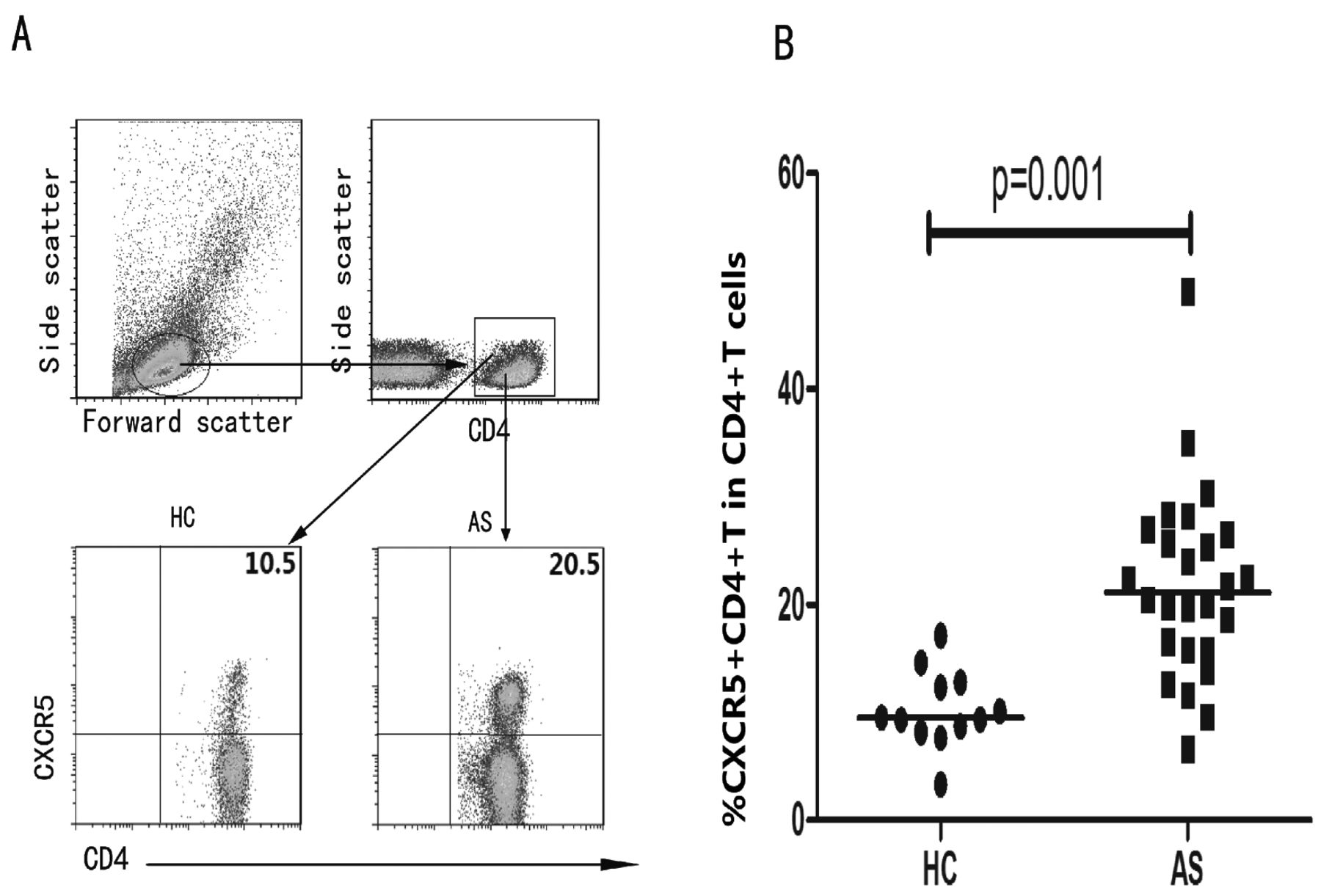
Flow cytometry analysis of the frequency of peripheral blood follicular Th cells. Peripheral blood mononuclear cells were isolated from individual patients and healthy controls (HC), and stained with anti-CD4 and anti-CXCR5 or isotype controls. Subsequently, the cells were gated on living CD4+ cells and the percentages of CXCR5+CD4+ TFH cells in total CD4+ T cells were determined. A. Flow cytometry analysis. B. Quantitative analysis. Data are representative charts or expressed as individual values from 12 HC and 26 patients with ankylosing spondylitis (AS) before treatment (0M). The horizontals indicate the median values of individual groups.

Flow cytometry analysis of the frequency of different subsets of follicular Th (TFH) cells. Peripheral blood mononuclear cells were isolated from individual subjects and stained with anti-CD4, antichemokine (C-X-C motif) receptor 5 (anti-CXCR5), antiinducible costimulator (anti-ICOS), antiprogrammed death 1 (anti-PD-1), as well as isotype controls. Cells were gated on CXCR5+CD4+ TFH cells, and the frequency of ICOS+CXCR5+CD4+, PD-1+CXCR5+CD4+, and PD-1+ICOS+CXCR5+CD4+ TFH cells in total CXCR5+CD4+ T cells was characterized by flow cytometry analysis. Some peripheral blood mononuclear cells were stimulated with phorbol myristate acetate and ionomycin in the presence of Brefeldin A, stained with anti-CD4 and anti-CXCR5, fixed, permeabilized, and further intracellularly stained with antiinterleukin 21 (IL-21) or isotype control, respectively. The frequency of IL-21+CXCR5+CD4+ TFH cells in total CXCR5+CD4+ TFH cells was characterized by flow cytometry analysis. In addition, the concentrations of serum IL-21 in individual subjects were measured by ELISA. A. Flow cytometry analysis. Panels B, C, D, E are quantitative analysis. F. Levels of serum IL-21. Data are representative charts or expressed as individual values of percentages of different subsets of CXCR5+CD4+ TFH in total number of CXCR5+CD4+ TFH cells or serum IL-21 from those subjects. The horizontal lines indicate the median values of different groups. HC: healthy controls; AS: ankylosing spondylitis.
Treatment significantly reduces concentrations of serum IL-21 and frequency of IL-21+CXCR5+CD4+ T cells in drug-responding but not in drug non-responding patients with AS
Patients with AS were being treated with NSAID, steroid, immunosuppressive agents, and TNF-α blockers, as well as physical therapy. We analyzed clinical measures and the frequency of TFH cells in 20 patients at 1 month posttreatment. We did not get complete data from the other 6 patients because of their unwillingness. Among the 20 patients tested, there were 15 drug-responders and 5 nonresponders at 1 month posttreatment. We found that treatment for 1 month reduced WBC, BASDAI, ESR, CRP, IgA, and IgG — but not IgM — in drug responders, accompanied by improved clinical symptoms; but not in drug nonresponders (Table 1). While treatment did not significantly change the frequency of total CXCR5+CD4+, PD-1+CXCR5+CD4+, ICOS+CXCR5+CD4+, or PD-1+ ICOS+CXCR5+CD4+ T cells, treatment did significantly reduce the frequency of IL-21+CXCR5+CD4+ TFH cells in drug-responding patients, as compared with those same drug-responding patients before treatment (p = 0.604, p = 0.319, p = 0.589, p = 0.272, p < 0.001; Figure 3A, 3B, 3C, 3D, and 3E, respectively). Similarly, the levels of serum IL-21 in those drug-responding patients 1 month after treatment were significantly lower than in the same patients before treatment (p < 0.001, Figure 3F). However, we did not detect significant changes in the frequency of different subsets of CXCR5+CD4+ T cells and the levels of serum IL-21 in those drug nonresponding patients between these 2 timepoints (data not shown). Thus, treatment inhibited CXCR5+CD4+ T cell activity in drug-responding patients with AS.

Treatment modulates the frequency of follicular Th (TFH) cells in drug-responding patients. In all followup, a total of 15 patients were drug responsive after 1 month of drug therapy. The frequency of CXCR5+CD4+ TFH in CD4+ T cells, and PD1+, ICOS+, PD1+ICOS+, IL-21+ CXCR5+CD4+ TFH in total CXCR5+CD4+ TFH cells in those patients, were determined by flow cytometry analysis before (0 month) and after treatment (1 month). The levels of serum IL-21 in those patients were determined by ELISA. AS: ankylosing spondylitis; PD: programmed death 1. See Figure 2 legend for other definitions.
Percentages of peripheral blood IL-21+CXCR5+CD4+ T cells are positively correlated with disease activities in patients with AS
To further test the importance of peripheral blood TFH cells in patients with AS, we analyzed the potential association of the percentages of different subsets of CXCR5+CD4+ T cells with the values of clinical measures by Pearson correlation analysis. We found that percentages of peripheral blood IL-21+CXCR5+CD4+ T cells were positively correlated with BASDAI values in those patients before treatment (r = 0.6, p = 0.0012; Figure 4). A similar correlation was observed in the drug-responding patients 1 month after treatment (r = 0.68, p = 0.005, Figure 4B), but there was no significant correlation between these measures in all patients 1 month after treatment and in drug nonresponding patients (data not shown). Interestingly, percentages of circulating PD-1+CXCR5+CD4+ T cells were negatively correlated with BASDAI values in those patients before treatment (r = −0.58, p = 0.0018, Figure 4C). However, there was no significant correlation between percentages of PD-1+CXCR5+CD4+ T cells and BASDAI values after treatment in both drug-responding (r = −0.071, p = 0.8, Figure 4D) and nonresponding patients (data not shown). There was no significant correlation among other measures tested in this population (data not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The correlation of the frequency of follicular Th (TFH) cells with the disease activity of those patients. The percentages of peripheral blood PD-1+ and IL-21+ CXCR5+CD4+ TFH cells in total CXCR5+CD4+ TFH cells of individual patients were plotted against the values of Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) before and after 1 month treatment in those patients, and the correlation between these 2 measures in those patients was analyzed. IL: interleukin; PD: programmed death 1. See Figure 2 legend for other definitions.
DISCUSSION
We found that the frequency of peripheral blood CXCR5+CD4+ TFH cells in patients with AS was significantly higher than that in HC. TFH cells are critical regulators of B cell development, germinal center formation, and antibody production32,33. We also found significantly higher levels of IgG and IgA antibodies in patients with AS, as compared with HC. Previous studies have shown that T, B, and NK cells as well as autoantibodies participate in the pathogenesis of AS5,6,7,8,9,10,11,12,13,14. In addition, Th17 cells participate in the process of several types of autoimmune diseases, and it is possible that increased numbers of CXCR5+ T cells may contain IL-17–secreting T cells16. The higher frequency of CXCR5+CD4+ T cells and associated higher levels of IgG and IgA antibodies in the patients with AS suggest that CXCR5+CD4+ T cells may contribute to the pathogenesis of AS.
Studies have shown that TFH cells express ICOS and PD-1, and produce IL-2117,18. ICOS+ TFH cells can positively regulate humoral responses and IL-21 production, while PD-1+ TFH cells predominantly receive negative signals, inhibiting humoral responses34,35,36,37,38. IL-21 is a crucial regulator of autoimmune diseases39,40,41. To further understand the role of TFH in the development and progression of AS, we characterized the frequency of ICOS+CD4+CXCR5+, PD-1+ICOS+CXCR5+CD4+, or PD-1+CD4+CXCR5+ T cells in this population and found that the percentages of PD-1+CXCR5+CD4+ or IL-21+CXCR5+CD4+ T cells were significantly higher than those in HC. However, unlike the findings of the 3 subsets (PD-1+, PD-1++, and PD-1+++) of PD-1–expressing TFH cells in human tonsils42, we did not find heterogeneous levels of PD-1 expression on TFH in human peripheral blood. The discrepancy may come from the different tissue locations of the TFH cells. Although the percentages of ICOS+CXCR5+CD4+ T cells in patients with AS were slightly higher than those in HC, there was no statistically significant difference. More importantly, the percentages of IL-21+CXCR5+CD4+ T cells were positively correlated with BASDAI values in the patients with AS.
These findings were in disagreement with a previous study on patients with spondyloarthritis, which showed that increased levels of plasma IL-21 and increased numbers of IL-21+ T cells were not significantly correlated with disease activity43. The discrepancy may stem from various populations of patients at different stages of disease; and the patients in our study fulfilled diagnostic criteria of the modified New York criteria for AS. The higher frequency of IL-21+CXCR5+CD4+ T cells and the correlation with the disease severity suggest that IL-21+CXCR5+CD4+ T cells may be major players in the pathogenesis of AS. PD-1 was highly expressed on TFH cells19. PD-1 has an inhibitory function on T cells and B cells, and was important in peripheral tolerance44. The increased frequency of PD-1+CXCR5+CD4+ T cells may stem from spontaneously compensative regulation of immune system so that increased frequency of PD-1+CXCR5+CD4+ T cells negatively regulates autoimmune responses in patients with AS. Indeed, higher levels of PD-1 expression also are detected in patients with RA and Sjögren syndrome45,46,47. More importantly, we also found that percentages of PD-1+CXCR5+CD4+ T cells were negatively correlated with BASDAI values in those patients with AS. Therefore, our novel data suggest that IL-21+CXCR5+CD4+ T cells may participate in the pathogenesis of AS and be used as a valuable measure for evaluating disease severity in patients with AS.
Currently, NSAID, painkillers, steroids, immunosuppressants, and TNF-α blockers are being used for the treatment of patients with AS in China48. We examined how therapy could affect TFH cells in these patients. We found that treatment with the therapy for 1 month significantly reduced ESR, WBC counts, levels of serum CRP, IgG, and IgA; and decreased the frequency of IL-21+CXCR5+CD4+ TFH cells and levels of serum IL-21 in 15 drug-responding patients, but not in 5 drug nonresponding patients. Our data are consistent with a previous report that TNF-α inhibitors markedly downregulate IL-21 expression in vitro on CD4+ T cells from patients with Crohn disease49. More importantly, treatment also significantly minimized BASDAI scores, which were positively correlated with the percentages of IL-21+CXCR5+CD4+ TFH cells in those drug-responding patients. These data clearly demonstrate that the therapy was effective in the control of disease activity in those patients. These findings also supported the notion that IL-21+CXCR5+CD4+ TFH participated in the pathogenesis of AS. Given the positive correlation between percentages of IL-21+CXCR5+CD4+ TFH and BASDAI values before and after treatment, measurement of peripheral blood IL-21+CXCR5+CD4+ TFH cells may be a valuable biomarker for evaluation of therapeutic efficacy in patients with AS, particularly in drug-responding patients.
Interestingly, we found that there was no significant change in clinical symptoms, laboratory measures, or the frequency of IL-21+CXCR5+CD4+ T cells in 5 drug non-responding AS patients. A previous study has shown that treatment with rituximab, an immunotherapy that targets B cells, improves clinical symptoms in AS patients with no history of TNF-α blocker treatment, but not in patients who do not respond to TNF-α blocker treatment14. Given that TNF-α blockers inhibit IL-21 production by CD4+ T cells, it is possible that higher frequency of IL-21+CXCR5+CD4+ T cells and higher levels of serum IL-21 are present in those patients who have failed TNF-α blocker treatment, leading to the ineffectiveness of rituximab. Therefore, therapeutic strategies may be promising for simultaneously targeting TNF-α, B cells, IL-21, and IL-21+CXCR5+CD4+ TFH cells in the treatment of patients with AS.
Our data show that percentages of IL-21+CXCR5+CD4+ T cells significantly increased and were positively correlated with disease severity in patients with AS. Treatment with meloxicam, thalidomide, and etanercept for 1 month dramatically reduced disease activity and frequency of IL-21+CXCR5+CD4+ T cells in the drug-responding patients, but not in the drug nonresponding patients. Therefore, percentages of IL-21+CXCR5+CD4+ T cells may be valuable biomarkers for evaluation of disease severity and therapeutic efficacy in patients with AS, particularly in drug-responding patients.
We recognize that our study had limitations of a small sample size and a lack of functional studies of TFH cells. Therefore, further studies of different subsets of TFH cells in the pathogenic process of AS with a bigger population are warranted.
Acknowledgment
We thank Medjaden Bioscience Limited for assisting in the preparation of this manuscript.
Footnotes
-
Supported by grants from the National Natural Science Foundation of China (No.30972610 and 81273240), the National High Technology Research and Development Program of China (863 Program, No. 2011AA02A106), Jilin Province Science and Technology Agency (No.20110716), and the Health Department Research Projects in Jilin Province (2009Z054) and Norman Bethune Program of Jilin University (2012206).
- Accepted for publication August 30, 2013.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.