
Abstract
Objective. Peptidylarginine deiminase type 4 (PADI4) and methyl-CpG binding domain 4 (MBD4) are closely related with rheumatoid arthritis (RA). We hypothesized that PADI4 and MBD4 polymorphisms may contribute to RA susceptibility.
Methods. We studied PADI4 rs2240340 G/A, PADI4 rs874881 C/G, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C gene polymorphisms in 329 patients with RA and 697 controls in a Chinese population. Genotyping was done using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS).
Results. When the PADI4 rs2240340 GG homozygote genotype was used as the reference group, the AA genotype was associated with a significantly increased risk of RA. In the recessive model, when PADI4 rs2240340 GG/GA genotypes were used as the reference group, the AA homozygote genotype was associated with a significant increased susceptibility to RA. PADI4 rs874881 C/G was in complete linkage disequilibrium with PADI4 rs2240340 G/A. MBD4 rs140693 G/A and MBD4 rs2005618 T/C polymorphisms were not associated with the risk of RA. In stratification analyses, a significantly increased risk for RA associated with the PADI4 rs2240340 AA genotype was evident among older patients and patients who were anticitrullinated protein antibody (ACPA)-positive compared with the PADI4 rs2240340 GG/GA genotype.
Conclusion. These findings suggest that the functional single-nucleotide polymorphism PADI4 rs2240340 G/A variant allele is associated with RA development, especially among older patients and ACPA-positive patients. However, our results were obtained from a moderate-sized sample, and therefore this is a preliminary conclusion. Validation by a larger study from a more diverse ethnic population is needed to confirm these findings.
- PADI4 POLYMORPHISM
- MBD4 POLYMORPHISM
- RHEUMATOID ARTHRITIS
- MOLECULAR EPIDEMIOLOGY
Rheumatoid arthritis (RA) is characterized by synovitis, progressive erosions, and cartilage destruction. RA is a chronic inflammatory disease with genetic and environmental predisposing factors1,2. RA affects ∼1% of the world population, and women are affected more than men3. It is estimated that ≤ 55% of the population variance in RA is genetic4.
Anticitrullinated protein antibodies (ACPA) have been specifically observed in the sera of patients with RA, and are a powerful, specific marker for RA5. ACPA appears early in RA, suggesting that it may have a specific role in the pathogenesis of the disease6. Peptidylarginine deiminases (PADI) post-translationally modify peptidylarginine to citrulline in the presence of calcium ions, and can change the conformation and functional properties of target proteins after citrullination7. PADI4 is one of several isoenzymes permitting post-translational conversion of arginine residues to citrulline, and this may be related to the production of ACPA8. PADI4 has been identified as one of the RA susceptibility genes, and has been reported to be associated with the level of ACPA in patients with RA9. PADI4 is mainly distributed in the cells of various hematopoietic lineages, and is expressed at high levels in the inflamed synovium of patients with RA. PADI4 is responsible for fibrin citrullination and is involved in apoptosis10. The PADI4 gene is located on chromosome 1p36, and has been associated with RA in Japanese and European populations11. One large-scale genome-wide, case-control study found that a PADI4 polymorphism was distinctly associated with RA9. Suzuki, et al showed that the PADI4 susceptibility haplotype had significantly increased mRNA stability compared with the nonsusceptibility haplotype9. This might be due to increased levels of the PADI4 enzyme, with consequent increased protein citrullination, which may diminish immune tolerance, leading to production of ACPA and disease9. Further analyses have revealed a functional haplotype that affects the stability of transcripts of PADI4 and which is also associated with levels of ACPA in the sera of patients with RA9. A recent metaanalysis revealed associations of PADI4 rs2240340 G/A with RA in the East Asian population12. However, associations at this locus are largely limited to Asians13.
Methylated CpG sites are recognized by a family of protein factors containing the methyl-CpG-binding domain (MBD). The MBD4 gene encodes a protein containing a methyl-CpG-binding domain and can remove enzymatically thymine (T) or uracil (U) from a mismatched CpG site in vitro14. MBD4 plays an important part in “genomic surveillance” and the progress of apoptosis by interacting with the MLH1 repair protein15 and the Fas ligand protein16. Three studies have examined a single-nucleotide polymorphism (SNP) in MBD4 and observed an association with an altered risk of lung cancer17,18 and squamous carcinoma of the esophagus19. MBD4 rs140693 G/A tagging SNP is associated with the risk of developing lung cancer in a Chinese population18. One study suggested that MBD4 polymorphisms were related to RA in Chinese patients in Taiwan, including MBD4 rs2005618 T/C SNP20. However, further investigations were not conducted.
Functional variations in PADI4 and MBD4 genes may contribute to the development of RA. We therefore undertook genotyping in a hospital-based case-control study in a cohort of 329 patients with RA and 697 controls in a Chinese population.
MATERIALS AND METHODS
Study subjects
We obtained approval of the study protocol from the Ethics Committee of Nanjing Medical University (Nanjing, China). All patients provided written informed consent to be included in the study.
Three hundred twenty-nine patients with RA who fulfilled the criteria for RA set by the American College of Rheumatology in 198721 were consecutively recruited from the Changzhou Second Hospital – Affiliated Hospital of Nanjing Medical University, the Changzhou First Hospital, and the Changzhou Traditional Chinese Medical Hospital (all located in Changzhou, China), between September 2010 and October 2011. The controls were patients without RA, matched for age (± 5 yrs) and sex, and recruited from the same institutions during the same time period; most of the controls were admitted to the hospitals for treatment of trauma.
Each patient was interviewed by trained personnel using a pretested questionnaire to obtain information on demographic data and related risk factors for RA. After the interview, 2 ml of peripheral blood was collected from each subject.
Isolation of DNA and genotyping by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS)
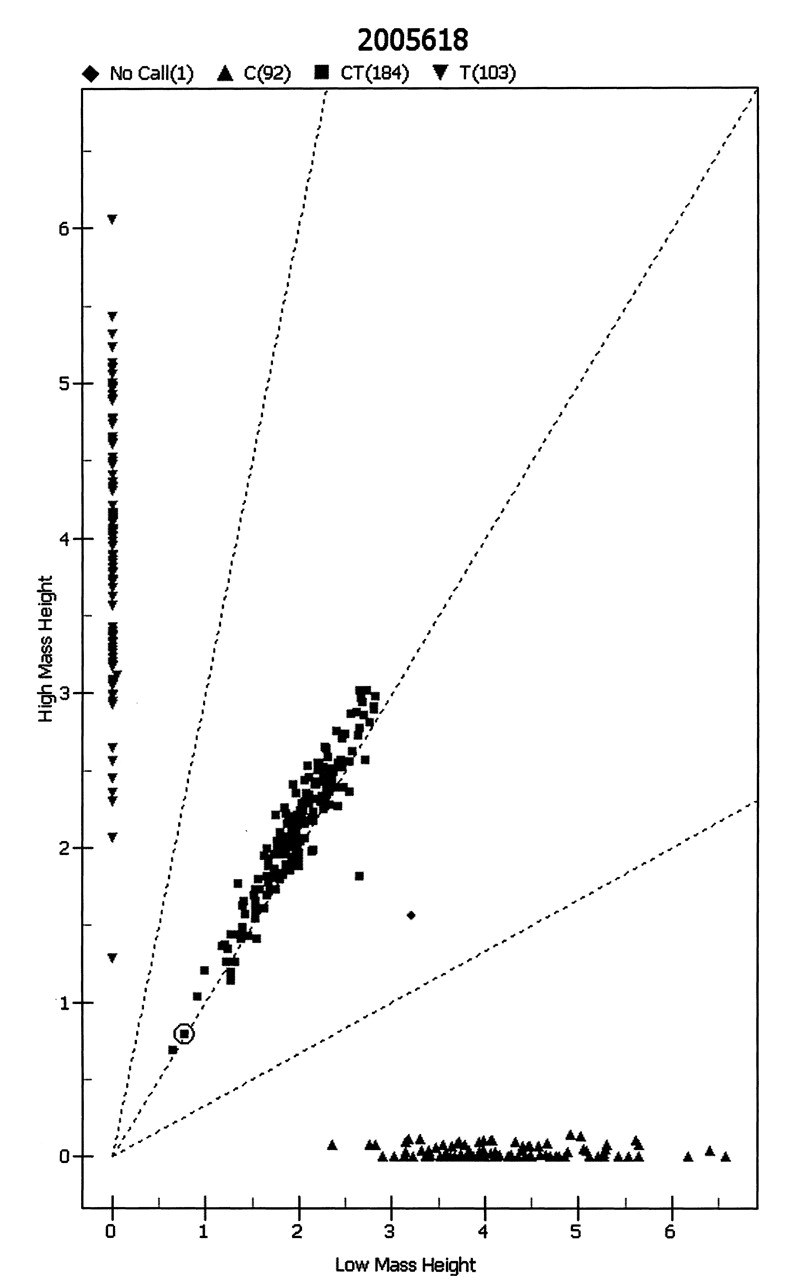
Blood samples were collected using vacutainers and transferred to test tubes containing ethylenediamine tetraacetic acid (EDTA). Genomic DNA was isolated from whole blood using the QIAamp DNA Blood Mini Kit (Qiagen, Hilden, Germany). Genotyping was done by MALDI-TOF MS using the MassARRAY system (Sequenom, San Diego, CA, USA) as described22. Cases and controls at a proportion of ∼1:2 were assayed. Completed genotyping reactions were spotted onto a 384-well spectroCHIP (Sequenom) using a MassARRAY Nanodispenser (Sequenom), and analyzed by MALDI-TOF-MS. Genotype calling was done in real time with MassARRAY RT software (version 3.1; Sequenom), and analyzed using MassARRAY Typer software (version 4.0; Sequenom; Figures 1–4). For quality control, repeated analyses were undertaken on 10% of randomly selected samples.

Genotyping of peptidylarginine deiminase Type 4 rs2240340 G/A polymorphism by MALDI-TOF MS.
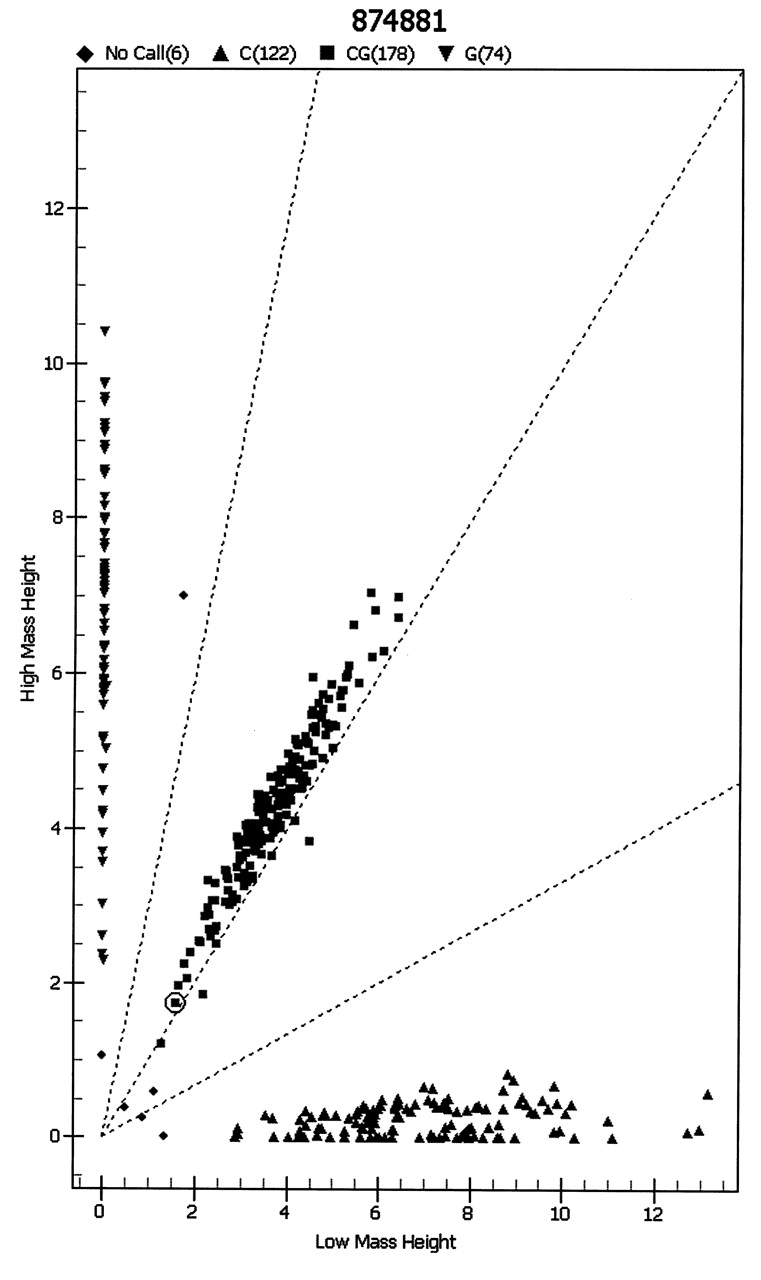
Genotyping of peptidylarginine deiminase Type 4 rs874881 C/G by MALDI-TOF MS.
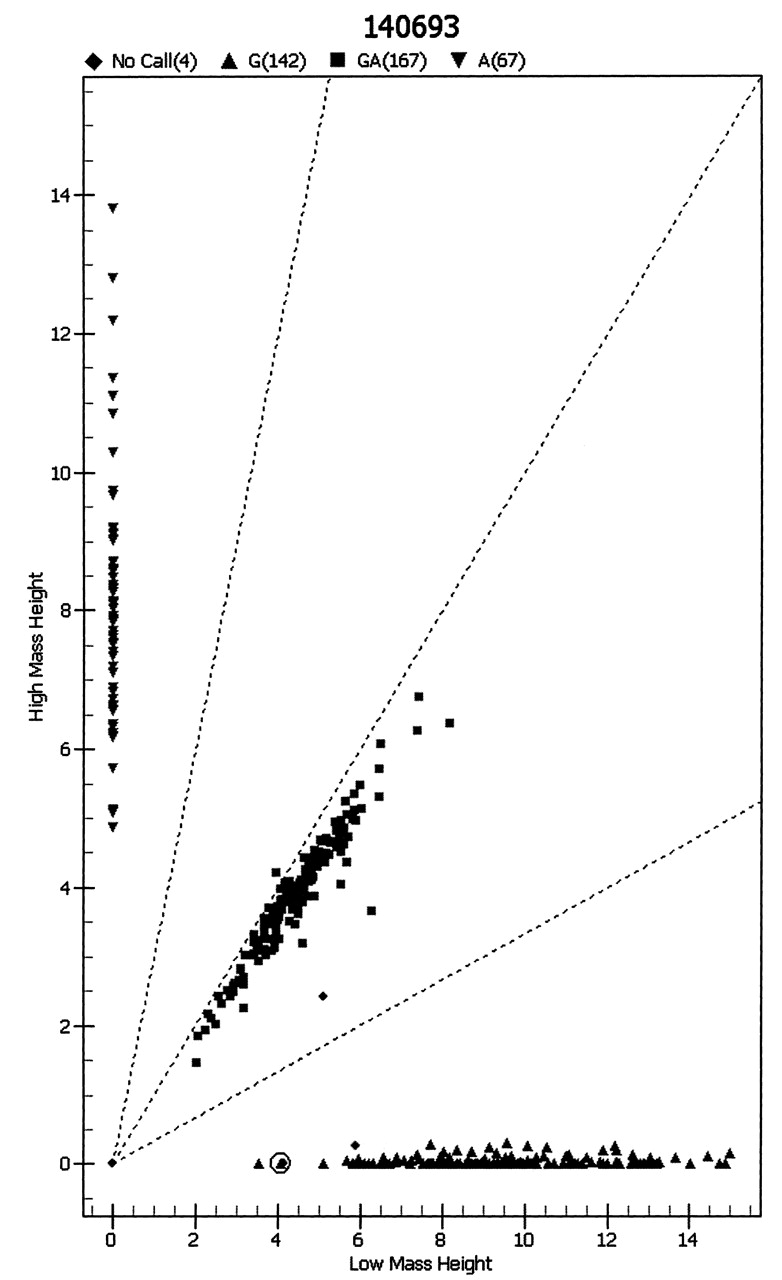
Genotyping of methyl-CpG binding domain 4 rs140693 G/A polymorphism by MALDI-TOF MS.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Genotyping of methyl-CpG binding domain 4 rs2005618 T/C polymorphism by MALDI-TOF MS.
Statistical analyses
Differences in demographics, variables, and genotypes of the PADI4 rs2240340 G/A, PADI4 rs874881 C/G, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C polymorphism variants were evaluated using a chi-squared test. Associations between PADI4 rs2240340 G/A, PADI4 rs874881 C/G, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C genotypes and risk of RA were estimated by computing odds ratios (OR) and 95% confidence intervals (CI) using logistic regression analyses, and by using crude OR. Hardy-Weinberg equilibrium (HWE) was tested by a goodness-of-fit chi-squared test to compare observed genotype frequencies to expected frequencies among controls. All statistical analyses were done with SAS software (version 9.1.3; SAS Institute, Cary, NC, USA).
RESULTS
Characteristics of the study population
Among 329 patients and 697 controls who provided DNA samples, genotyping for the PADI4 rs2240340 G/A polymorphism was successful in 324 (98.5%) patients and 695 (99.7%) controls. The demographic and clinical characteristics of all subjects are summarized in Table 1. Subjects were adequately matched for age and sex (p = 0.829 and 0.190, respectively). The genotype distributions of PADI4 rs2240340 G/A, PADI4 rs874881 C/G, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C in all subjects are illustrated in Table 2. The observed genotype frequencies for the polymorphism in controls were in HWE for PADI4 rs2240340 G/A (p = 0.751), PADI4 rs874881 C/G (p = 0.803), MBD4 rs140693 G/A (p = 0.643), and MBD4 rs2005618 T/C (p = 0.511).
Patient demographics and risk factors in rheumatoid arthritis (RA), all subjects.
Logistic regression analysis of associations between PAD14 rs2240340 G/A, PAD14 rs874881 C/G, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C polymorphisms and risk of rheumatoid arthritis.
Associations between PADI4 rs2240340 G/A, PADI4 rs874881 C/G, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C polymorphism and risk of RA
The genotype frequencies of the PADI4 rs2240340 G/A polymorphism were 31.5% (GG), 46.9% (GA), and 21.6% (AA) in patients with RA, and 35.1% (GG), 48.8% (GA), and 16.1% (AA) in controls (p = 0.093; Table 2). When the PADI4 rs2240340 GG homozygote genotype was used as the reference group, the AA genotype was associated with a significantly increased risk for RA (OR 1.50, 95% CI 1.03–2.18, p = 0.037). In the recessive model, when the PADI4 rs2240340 GG/GA genotypes were used as the reference group, the AA homozygote genotype was associated with a significant 1.44-fold increased susceptibility to RA (OR 1.44, 95% CI 1.03–2.00, p = 0.034).
PADI4 rs874881 C/G was in complete linkage disequilibrium with PADI4 rs2240340 G/A (r2 = 1.00). Logistic regression analyses also revealed that PADI4 rs874881 C/G polymorphism was associated with the risk of RA (Table 2).
None of the MBD4 rs140693 G/A and MBD4 rs2005618 T/C polymorphisms achieved a significant difference in the genotype distributions between cases and controls. Logistic regression analyses revealed that MBD4 rs140693 G/A and MBD4 rs2005618 T/C polymorphisms were not associated with the risk of RA (Table 2).
Stratification analyses of PADI4 rs2240340 G/A, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C polymorphisms and risk for RA
Stratification analyses were done to evaluate the effects of PADI4 rs2240340 G/A, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C genotypes on RA risk according to age, sex, C-reactive protein status, and ACPA status (Table 3). A significantly increased risk for RA associated with the PADI4 rs2240340 AA genotype was evident among older patients (OR 1.85, 95% CI 1.16–2.96, p = 0.010) and anti-CCP-positive patients (OR 1.54, 95% CI 1.01–2.34, p = 0.043) compared with the PADI4 rs2240340 GG/GA genotype.
Stratified analyses between PAD14 rs2240340 G/A, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C polymorphisms and risk of rheumatoid arthritis.
DISCUSSION
We studied the association between the PADI4 rs2240340 G/A, PADI4 rs874881 C/G, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C polymorphisms and risk of RA in a Chinese population. We found that the PADI4 rs2240340 AA allele may increase the risk of RA, and that this effect was more evident in older patients and ACPA-positive patients.
PADI4 is significantly overexpressed in the blood of patients with RA regardless of their disease activity23. Expression of the PADI enzyme, citrullination of proteins, and production of anti-citrullinated protein antibodies occurs in the synovium of patients with RA, thus highlighting its importance in disease pathogenesis24. It had been noted that ACPA appear to be specific for RA25. PADI activity appears to be implicated in the generation of ACPA, which is highly specific to patients with RA12. Further analyses revealed a functional haplotype that affects the stability of transcripts of PADI4, and which is also associated with levels of ACPA in the sera of patients with RA9. Reports on the association of the PADI4 polymorphism with RA have provided inconsistent data. We found that the PADI4 rs2240340 AA allele may increase the risk of RA, particularly in patients who are ACPA-positive, indicating a gene-environment interaction. We also found that the PADI4 rs2240340 AA allele may increase the risk of RA, especially in older patients.
Several genetic studies have evaluated the association between PADI4 gene variants and RA. Functional haplotypes have been found to be strongly associated with RA in populations of Japanese descent9. The genetic association between PADI4 and RA was replicated in another Japanese group26 and in a Korean population27. However, many studies in white subjects (including cohorts from the UK, Spain, and France) yielded conflicting findings23,28,29,30,31,32,33. This may have been due to the different ethnic populations studied.
Ethnic differences may play a part in the conflicting results seen in association studies. Our replicated results, using the same genetic markers within subjects of different ethnic backgrounds as those in the original study, suggest that PADI4 confers susceptibility for RA in the Chinese population.
In a Chinese population involving 193 patients and 190 healthy controls in Taiwan, the MBD4 rs2005618 T/C polymorphism was associated with RA risk20. However, in our present study, we failed to find an association between MBD4 rs2005618 T/C and RA risk.
Several limitations of our study need to be addressed. First, this was a hospital-based case-control study, so selection bias was unavoidable and subjects were not fully representative of the general population. Second, the polymorphisms we investigated, based on their functional considerations, may not offer a comprehensive view of the genetic variability of PADI4 and MBD4. Third, a single case-control study is not sufficient to fully interpret the relationship between PADI4 rs2240340 G/A, PADI4 rs874881 C/G, MBD4 rs140693 G/A, and MBD4 rs2005618 T/C polymorphisms and susceptibility to RA because of the relatively moderate number of patients evaluated. Larger numbers of subjects are necessary to confirm our findings, especially for the negative results of MBD4 rs140693 G/A and MBD4 rs2005618 T/C polymorphisms and RA. Finally, we did not obtain detailed information about the outcomes of treatment, which restricted our analyses.
Our study provided strong evidence that PADI4 rs2240340 G/A functional polymorphisms may contribute to the risk of RA. However, our results were obtained from a moderate-size sample, and therefore represent a preliminary conclusion. Further gene-gene and gene-environment interaction studies are warranted to elucidate our findings.
- Accepted for publication February 29, 2012.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.