
Abstract
Objective. Kawasaki disease (KD) is an acute febrile disease in infants and young children. Five percent to 8% of cases will be complicated with coronary dilatation or aneurysm, although introduction of high-dose intravenous immunoglobulin (IVIG) therapy has provided remarkable results for reducing the frequency of cardiac involvement. We describe the results of an open-label trial of infliximab, an anti-tumor necrosis factor-α monoclonal antibody, for suppressing the progression of coronary artery lesions in cases of KD refractory to extensive IVIG therapy. Plasma exchange (PE) was available as a rescue therapy for patients refractory to infliximab.
Methods. Twenty eligible patients fulfilled the diagnostic criteria for KD, and were primarily treated with IVIG up to 4 g/kg. “Refractory to IVIG” was defined as persisting or reemerging fever > 38°C and positive fractional changes of C-reactive protein, white blood cell counts, or neutrophil counts 48 hours after IVIG infusion. These cases were treated with infliximab, 5 mg/kg, which should begin within 10 days of disease onset. PE for patients refractory to infliximab was performed with 5% albumin.
Results. There was rapid improvement of inflammatory symptoms as well as normalization of the inflammatory markers. Sequential examination by echocardiography up to disease Day 30 revealed that the inflamed and mildly dilated coronary artery at the beginning of the study regressed to normal size in the convalescent phase. Two out of 20 patients showed incomplete improvement of inflammatory symptoms after infliximab treatment, and were provided with PE therapy, with no complications.
Conclusion. Eighteen of 20 patients were effectively treated with infliximab, and 2 cases were effectively treated with PE to prevent progression to coronary artery lesions. No adverse event such as anaphylactoid reaction, heart failure, severe infectious diseases, or tuberculosis was observed in this trial.
- KAWASAKI DISEASE
- PROINFLAMMATORY CYTOKINE
- INFLIXIMAB
- INTRAVENOUS IMMUNOGLOBULIN THERAPY
- PLASMA EXCHANGE
Kawasaki disease (KD) is an acute febrile disease in infants and young children that is characterized by 6 typical clinical symptoms — persistent high fever, polymorphous rash, bilateral conjunctival congestion, lip cracking/bleeding and strawberry tongue, acute nonpurulent cervical lymphadenopathy, and indurative edema of extremities1.
Increased levels of tumor necrosis factor-α (TNF-α), interleukin 1ß (IL-1ß), and IL-6 in the active phase of the disease are rapidly normalized after therapy with high-dose intravenous immunoglobulin (IVIG), suggesting that proinflammatory cytokines are responsible for the progression of the disease, and that removal of these cytokines from the circulation will be a major strategy of treatment2.
Stimulated by reports of investigations of infliximab therapy by Burns, et al3,4, we undertook an open-label intervention case series study of the efficacy of infliximab for suppressing the progression of coronary artery lesions (CAL) in cases of KD that had been intractable to extensive IVIG therapy. In our study we offered plasma exchange (PE) as a rescue therapy for patients refractory to infliximab.
MATERIALS AND METHODS
Patients and therapy
Twenty patients eligible for the study were 2 to 10 years of age and fulfilled the diagnostic criteria for KD in Japan (2002 version)5. Patients were treated primarily with IVIG 2 to 4 g/kg; refractoriness to IVIG was defined as persisting or reemerging fever > 38°C, and as positive fractional changes of C-reactive protein (CRP), white blood cell (WBC) counts, or neutrophil counts at 48 hours after IVIG infusion6. Infliximab treatment should begin within 10 days of disease onset.
Patients were excluded if they had infectious diseases including lung tuberculosis, recent therapy with corticosteroids or biologic response modifiers, vaccination with bacillus Calmette-Guerin within 6 months before disease onset, low cardiac function, or liver/renal dysfunction.
Infliximab, 5 mg/kg in 100 ml saline, was intravenously administered in an open-label manner. PE for patients refractory to infliximab was performed with 5% albumin as replacing agent for 3 consecutive days7,8.
The study protocols and amendments were approved by the appropriate institutional review board.
Evaluation
Patients were assessed for improvement 48 hours after infliximab infusion. Additionally, after 30 days a followup coronary artery examination was carried out by echocardiography.
Patients who did not show improvement of fever and fractional changes of CRP, WBC counts, and neutrophil counts 48 hours after receiving infliximab were given PE as soon as possible6.
The primary efficacy endpoints were the proportions of children showing decrease of fever, improvement of inflammatory markers, and intact coronary artery.
RESULTS
Population characteristics
The baseline demographics of the 20 patients are summarized in Table 1. Although patients were treated with high-dose IVIG, they showed high fever, persistent clinical symptoms, and increased levels of inflammatory markers. Echocardiography revealed increased echogenicity or mild dilatation of the coronary artery in all patients.
Baseline characteristics of patients with Kawasaki disease (KD). Data are mean (range) unless otherwise indicated.
Efficacy and adverse events
Changes of body temperature are shown in Figure 1. Eighteen patients showed rapid decreases of fever within 24 hours after infliximab infusion. These 18 patients showed gradual decreases in the number of symptoms within 3 days after infliximab administration (Figure 2A). The laboratory examinations also indicated that infliximab treatment provided favorable antiinflammatory effects within 2 to 3 days (Figure 2B, 2C).
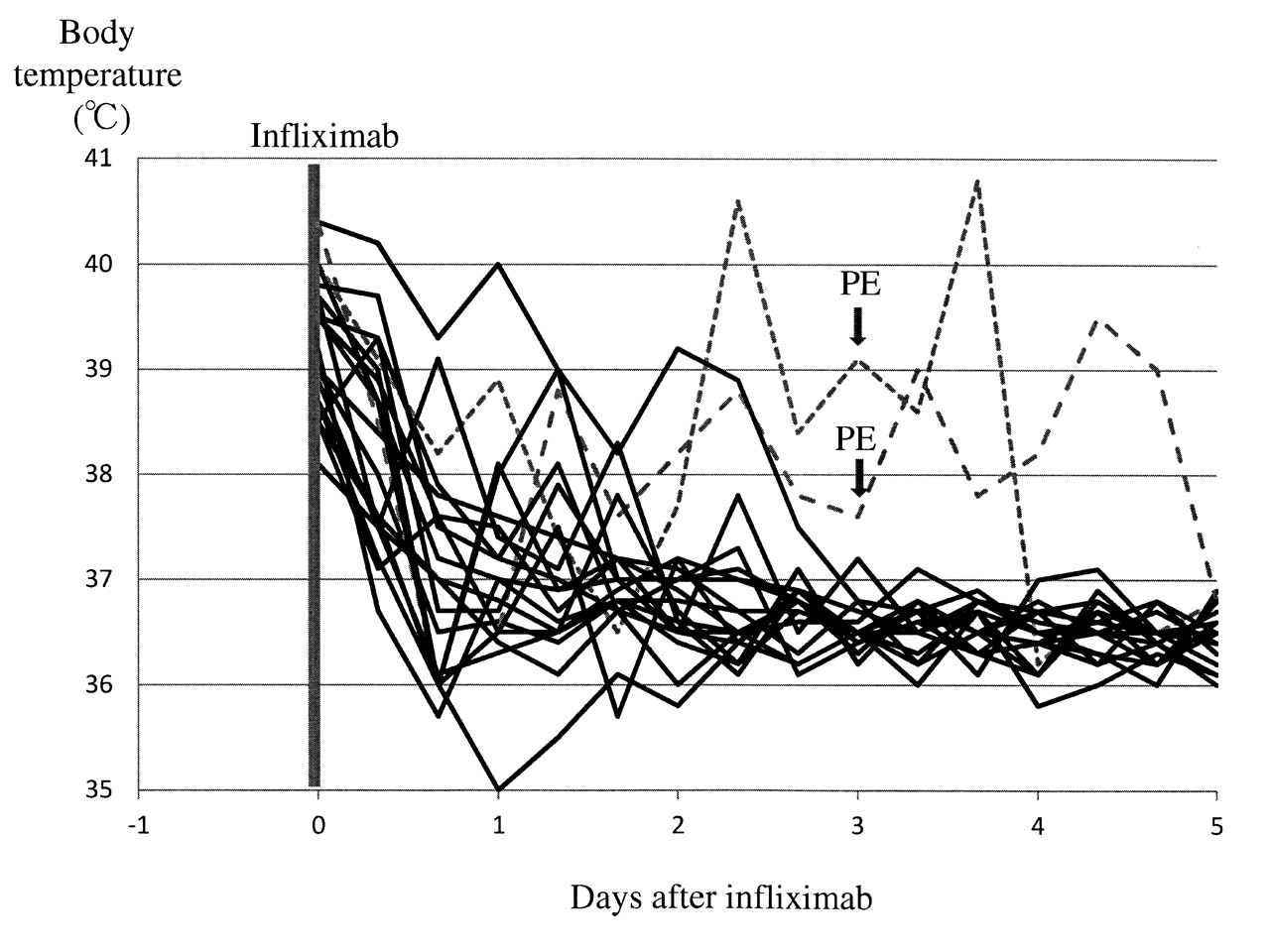
Course of patients’ body temperature: maximum temperature in 1 day was monitored every day before and after infliximab infusion. Eighteen patients showed rapid decreases of fever within 24 hours after infliximab infusion. However, fluctuations of body temperature were noted in 2 patients. PE: plasma exchange.

{kind=link}
{kind=link}
Clinical data results. A. Symptoms: 18 patients with 5 or 6 major symptoms of Kawasaki disease at enrollment showed gradual decreases of these symptoms within 3 days after infliximab administration. B. White blood cell (WBC) counts: treatment resulted in rapid decreases of WBC within 2 to 3 days in those who responded to infliximab, assessed by fever and clinical symptoms. C. C-reactive protein (CRP): treatment provided rapid decreases of CRP within 2 to 3 days in those who were responders to infliximab, assessed by fever and clinical symptoms.
Two other patients were refractory to infliximab, with persistent high fever, and they underwent PE with effective outcomes.
Only 1 patient showed CAL at 30 days after onset of therapy, but the patient had complete regression of CAL by cardiac catheter examination 1 year later.
In this case series, no adverse events (anaphylactoid reaction, heart failure, severe infectious diseases, or tuberculosis) were recorded during and after the infliximab treatment.
DISCUSSION
Our open-label case series of infliximab therapy for 20 children with KD refractory to IVIG demonstrated rapid improvement of inflammatory symptoms as well as normalization of inflammatory markers. Sequential examination by echocardiography up to disease Day 30 revealed that patients’ coronary arteries that were inflamed and mildly dilated at enrollment to the study regressed to normal size in the convalescent phase. However, 2 of 20 patients showed incomplete improvement of the inflammatory symptoms and signs after infliximab treatment. These patients then underwent PE to block the progression to CAL, with effective results. No adverse events were observed.
The major goal of this trial in patients with KD was to prevent progression of CAL. The first-line treatment for KD at present is IVIG. However, 4% to 8% of patients are refractory to IVIG treatment, thus leading to the search for second-line treatments that should be applied within 10 days, before occurrence of irreversible CAL. Additional IVIG therapy9, methylprednisolone pulses10,11, and PE therapy7,8 have also been recommended.
Both TNF-α and IL-1ß in active KD have been closely related to vascular endothelial cell damage and resulting CAL12. Burns, et al first reported that infliximab was effective in treating patients with refractory and long-lasting KD in prevention of inflammatory responses3. However, 17 patients enrolled in that study differed in disease-day at treatment, 12 of 17 patients eventually developed CAL, and 1 patient died. Thus, there could be unknown factors influencing the efficacy of infliximab for blocking the formation of CAL. Further, Burns, et al also showed that considering the formation of CAL, infliximab treatment was superior to treatment with additional IVIG for KD that was intractable to the first IVIG4.
In the serum of the patient with disease refractory to infliximab, infliximab was still detected 48 hours after infusion, suggesting that unknown factors or cytokines other than TNF-α were responsible for the unresponsiveness and disease progression.
To prepare an alternative back-up therapy was ethically essential in this kind of trial for childhood disease. We provided PE therapy for children with disease that was intractable under the infliximab trial. Although time-consuming and expensive, PE had been shown to be effective for complete elimination of proinflammatory cytokines7,8. Two cases unresponsive to infliximab in the present trial were successfully treated with 3 days of PE therapy. In other studies, after the administration of infliximab, no patients developed infectious status13 or cardiac complications14.
Infliximab treatment for KD refractory to IVIG therapy in our study showed a positive risk-benefit profile, and was found to be suitable for the limited treatment period that was available. As back-up therapy for cases of KD refractory to infliximab, PE would be prepared before starting infliximab in our clinical setting.
- Accepted for publication November 10, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.