
Abstract
Objective. Results from studies of the association between angiotensin-converting enzyme (ACE) insertion/deletion (I/D) gene polymorphism and systemic lupus erythematosus (SLE)/lupus nephritis (LN) are controversial. We performed this metaanalysis to evaluate the relationship between ACE I/D gene polymorphism and SLE/LN and to explore whether the ACE D allele or DD genotype could become a predictive marker for risk of SLE/LN.
Methods. Association studies were identified from the databases of PubMed, Embase, Cochrane Library and CBM-disc (China Biological Medicine Database) as of May 1, 2011, and eligible investigations were synthesized using a metaanalysis method. Results were expressed with OR for dichotomous data, and 95% CI were calculated.
Results. Sixteen investigations were identified for the analysis of association between ACE I/D gene polymorphism and SLE, consisting of 1959 patients with SLE and 2078 controls. In the overall populations, there was a marked association between D allele or DD genotype and SLE susceptibility (D: OR 1.29, 95% CI 1.04–1.58, p = 0.02; DD: OR 1.60, 95% CI 1.17–2.19, p = 0.003), and DD homozygous was associated with LN risk (OR 2.78, 95% CI 1.26–6.11, p = 0.01). In the subgroup analysis, DD genotype associated with SLE risk was observed in Asians; no other association was found in Asians, whites, Africans, and Brazilians.
Conclusion. D allele and DD homozygous are significant genetic molecular markers to predict SLE susceptibility, and DD genotype is a valuable marker to predict the LN risk. More investigations are required to clarify the association of the D allele or DD homozygous with SLE/LN susceptibility.
- SYSTEMIC LUPUS ERYTHEMATOSUS
- LUPUS NEPHRITIS
- GENE POLYMORPHISM
- ANGIOTENSIN-CONVERTING ENZYME
- INSERTION/DELETION
- METAANALYSIS
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease1,2,3 mainly characterized clinically by involvement of joints, skin, and kidneys4,5. SLE is a severe disease that results from both genetic predisposition and environmental factors6. Lupus nephritis (LN) is one of the most common manifestations in SLE7 and remains a predominant cause of morbidity and mortality in SLE8. SLE is characterized by increasing vascular lesion risk9, and vascular lesions are encountered frequently in renal biopsy specimens of patients with SLE; the lesions can present in a variety of morphologic forms10. Some studies have found that gene polymorphism was associated with the risk of SLE11,12 and LN susceptibility13,14.
The activation of the renin-angiotensin-aldosterone system (RAAS) is part of the onset of SLE and LN15,16. Angiotensin-converting enzyme (ACE), a key zinc metallopeptidase, catalyzes the conversion of angiotensin I to angiotensin II, which is the main active product of the RAAS17. The ACE gene consists of either an insertion (I) allele or a deletion (D) allele and forms 3 possible genotypes: II, ID, and DD18. DD homozygous or D allele is associated with elevated circulating and tissue ACE activity compared to I allele. ACE is important in the development of SLE because its endproduct, angiotensin II, plays an integral role in the regulatory system responsible for endothelial control and vascular tone, systems that are commonly affected in patients with SLE19. Additionally, ACE inhibitors have been shown to alleviate the progression of SLE and LN19.
The ACE I/D gene polymorphism, correlating with circulating and cellular ACE concentration20, might be implicated in the etiology of SLE or LN and has been investigated in numerous epidemiologic studies. However, the available evidence is weak, due to sparseness of data or disagreements among the reported investigations. The evidence from metaanalysis may be powerful when compared with the individual investigations. Lee, et al21 conducted an interesting metaanalysis to explore the association of ACE I/D gene polymorphism with the SLE or LN risk and found that there was a lack of association of the ACE I/D polymorphism with SLE and LN. However, that study included only 10 reports. We performed this metaanalysis to investigate whether the ACE I/D gene polymorphism was associated with the onset of SLE or LN by collecting the reported investigations, and to update the conclusions from Lee, et al.
MATERIALS AND METHODS
Search strategy for the association of ACE I/D gene polymorphism with SLE risk
The relevant studies were searched from the electronic databases of PubMed, Embase, Cochrane Library, and CBM-disc (China Biological Medicine Database) on May 1, 2011. The retrieval strategy of (Systemic lupus erythematosus OR SLE) AND (Angiotensin converting enzyme OR ACE) was entered into these databases. Additional articles were identified through references cited in retrieved articles.
Inclusion and exclusion criteria for SLE vs control/LN vs control
Inclusion criteria: (1) the outcome had to be SLE/LN; (2) there had to be at least 2 comparison groups (SLE group vs control group/LN group vs control group); and (3) investigation should provide detailed data of the ACE genotype distribution. Exclusion criteria: (1) review articles and editorials; (2) case reports; (3) preliminary result not on ACE I/D gene polymorphism or outcome; and (4) investigating the role of ACE inhibitor on disease. If multiple publications from the same study group were found, we included only the most complete report in our final analysis.
Data extraction and synthesis
Two investigators independently extracted the following information from each eligible study: first author’s surname, year of publication, and number of cases and controls for ACE genotypes. Frequency of D allele was calculated for case group and control group, from the corresponding genotype distribution. The results were compared and disagreement was resolved by discussion.
Statistical analysis
Cochrane Review Manager Version 5 (Cochrane Library, UK) was used to calculate the available data from each investigation. The pooled statistic was counted using the fixed-effects model, but a random-effects model was conducted when the p value of the heterogeneity test was < 0.122. Results were expressed with OR (95% CI) for dichotomous data. A value of p < 0.05 was required for the pooled OR to be statistically significant. I2 was used to test the heterogeneity among the included studies. In order to avoid excessive comparisons, the OR was calculated by 3 methods: (1) allele comparison (D allele vs I allele); (2) comparing DD homozygous with the other 2 combinations (DD vs DI + II); and (3) comparing II genotype with the other 2 combinations (II vs DD + DI). A chi-square test using a Web-based program was applied to determine whether genotype distributions of the case group/control group reported conformed to Hardy-Weinberg equilibrium (HWE; p < 0.05 was considered significant). The gene distributions of the control group in the included studies were not in HWE, a situation that might result in heterogeneity17,23, and the study indicating that the genotype distributions in the control group significantly deviated from HWE was excluded from our sensitivity analysis24. The Begg adjusted rank correlation test25 and the Egger regression asymmetry test26 were used for exploring publication bias (p < 0.1 was considered significant) when the number of included studies was > 5. All descriptive data were expressed as mean ± SD.
RESULTS
Study characteristics for SLE vs control
Sixteen studies27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42 were used in our investigation. Three studies27,30,36 were published in Chinese and the others were reported in English. These data were extracted: first author’s surname, year of publication, and the number of cases and controls for ACE genotype (Table 1). Those 16 investigations contained 1959 case series and 2078 controls. The average distribution frequency of ACE D allele in patients with SLE was 55.85% and the average frequency in controls was 49.43%. The average distribution frequency of D allele in cases was slightly increased compared with that in the control group (SLE/control = 1.13).
Characteristics of the studies evaluating the effects of ACE genes on SLE risk.
Study characteristics for LN vs control
Seven studies27,30,31,39,40,41,42 were included into our metaanalysis for LN versus control (Table 2). Those investigations involved 417 patients with LN and 981 controls. The average distribution frequency of the ACE D allele in patients with SLE was 60.37%, and the average frequency in controls was 47.98%. The average distribution frequency of the D allele in the LN group was markedly increased compared with that in the control group (LN/control = 1.26).
Characteristics of the studies evaluating the effects of ACE genes on LN risk.
Association of the ACE I/D gene polymorphism with SLE risk (SLE vs control)
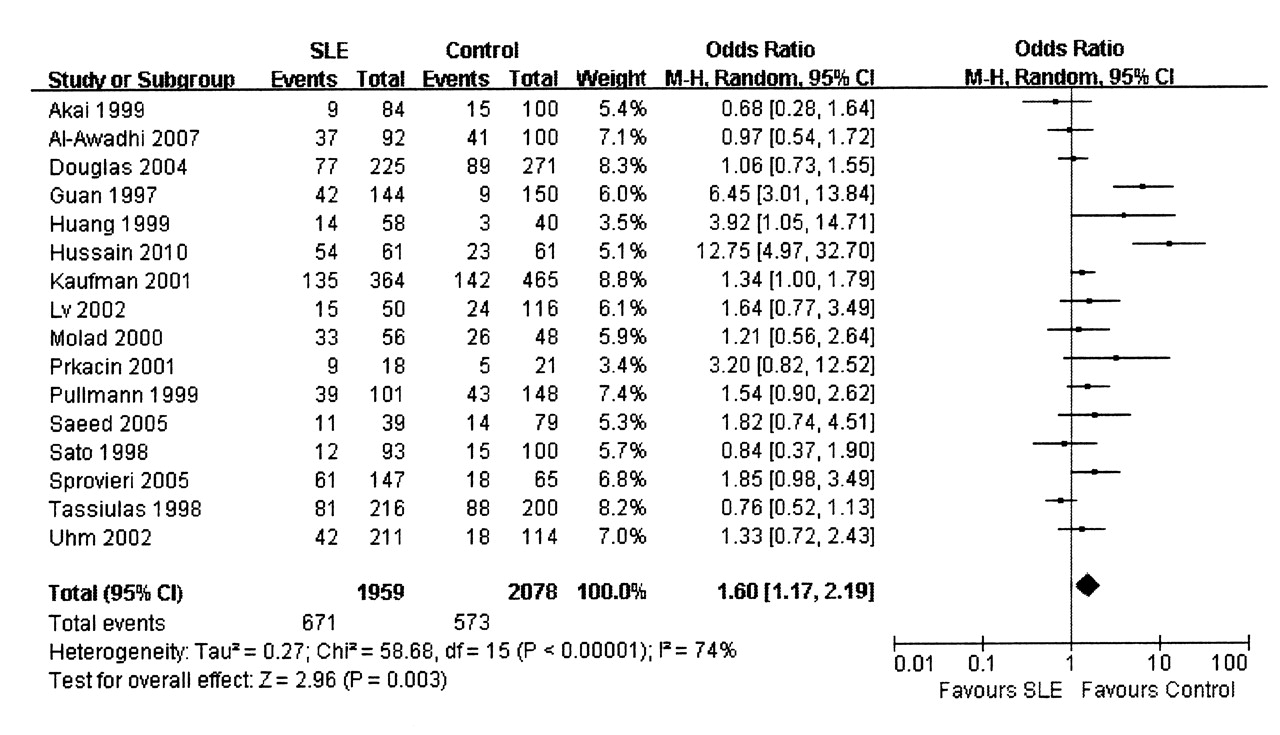
In our metaanalysis, we found that the D allele and DD genotype were associated with SLE risk (Figure 1 for D allele and Figure 2 for DD genotype), but the association of II homozygous with SLE susceptibility was not observed (Table 3). The genotype distributions of the control population in 1 study36 did not conform to HWE, and this investigation was excluded from our sensitivity analysis. In the analysis, the results were similar to those in the nonsensitivity analysis (Table 3).
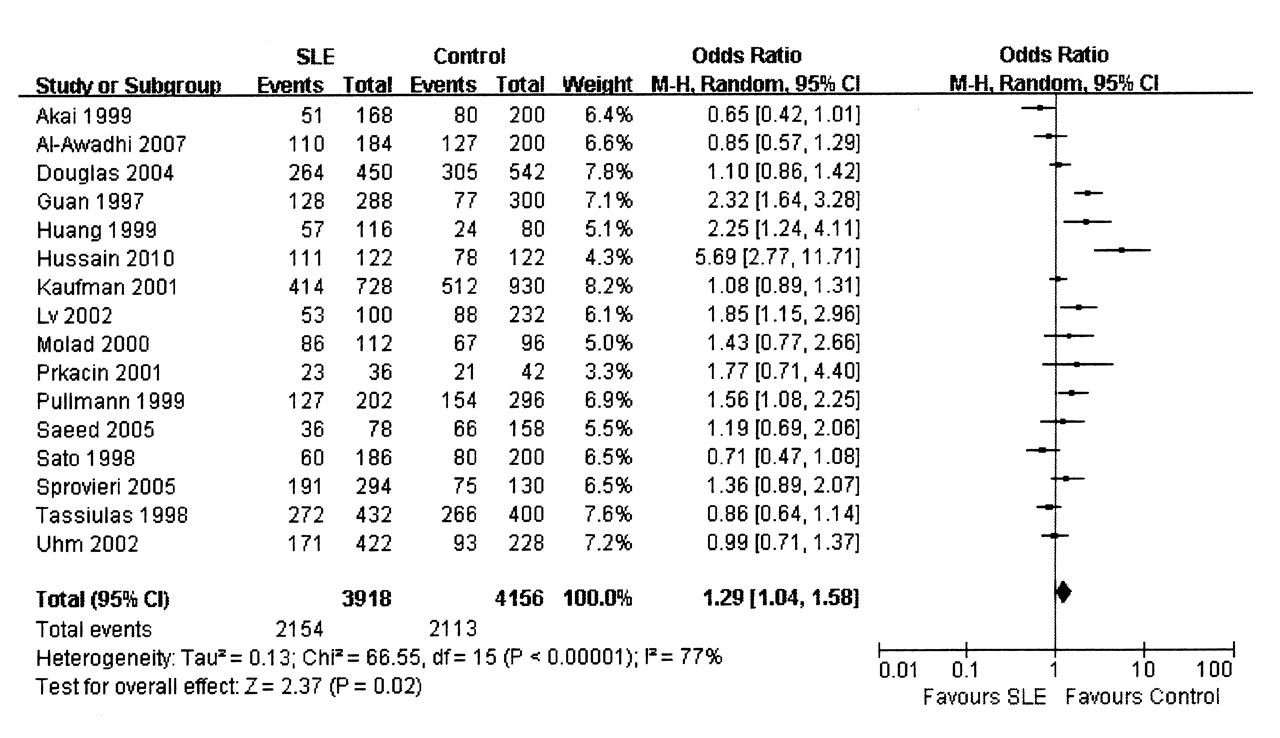
Association between D allele and risk for systemic lupus erythematosus (SLE). M-H: Mantel-Haenszel.
{kind=link}
{kind=link}
Association of DD genotype with risk for systemic lupus erythematosus (SLE). M-H: Mantel-Haenszel.
Metaanalysis of the association of ACE I/D gene polymorphism with risk of SLE.
We also performed a subgroup analysis according to different races. For Asians, we found that DD homozygous was associated with SLE risk, but the association for D allele or II genotype was not observed (Table 3). Sensitivity analysis according to HWE test was performed (1 report36 was excluded), and no association between ACE I/D gene polymorphism and SLE risk was observed (Table 3).
Subgroup analyses for whites, Africans, and Brazilians were also performed. We found that the ACE I/D gene polymorphism was not associated with the onset of SLE in whites, Africans, and Brazilians (Table 3). The gene distributions of the control group in all the included reports were in HWE, so the results from the sensitivity analysis were the same as those of the nonsensitivity analysis.
Association of ACE I/D gene polymorphism with LN susceptibility (LN vs control)
In our study of LN vs control, we found that DD genotype was associated with the risk of LN (OR 2.78, 95% CI 1.26–6.11, p = 0.01; Table 4) in overall populations. However, no associations for D allele and II genotype were found in this study for LN versus control (Table 4).
Metaanalysis of the association of ACE I/D gene polymorphism with risk of lupus nephritis.
Subgroup analysis according to different races was also performed. We found no association between ACE I/D gene polymorphism and LN risk in Asians and Brazilians (Table 4).
The gene distributions of control groups in all the included reports were in HWE, so the results from sensitivity analysis were the same as those of nonsensitivity analysis.
Evaluation of publication bias
In the comparison of SLE versus control, no significant publication bias was found for overall populations, Asians, and whites (overall populations: Begg p = 0.964, Egger p = 0.680; Asians: Begg p = 0.466, Egger p = 0.975; whites: Begg p = 1.000, Egger p = 0.227). In the comparison of LN versus control, there was no significant publication bias for overall populations and Asians (overall populations: Begg p = 0.548, Egger p = 0.643; Asians: Begg p = 0.806, Egger p = 0.429).
DISCUSSION
The genetic origin of SLE and LN had been a focus of research in recent years, and some investigations found that the genetic alteration could become an early diagnosis indicator to predict the susceptibility of some diseases43,44,45,46. The level of plasma ACE, constitutively expressed in several types of somatic cells, is linked to an I/D polymorphism of 287 bp in intron 16 of the ACE gene17,18. D allele and DD homozygous have been reported to be associated with higher plasma ACE levels23,47,48. The increased protein expression of ACE is responsible for the elevation of plasma angiotensin II level23,49. There was some significant evidence showing that ACE was involved in the risk of SLE and LN19,50,51. So the D allele or DD homozygous might be important molecular markers for the risk of SLE or LN. Most of the studies investigating the association between ACE I/D gene polymorphism and the risk of SLE/LN explored whether the ACE I/D gene polymorphism could become a valuable indicator to predict the risk of SLE/LN. However, data were insufficient. Further, findings on the association of ACE I/D gene polymorphism with the susceptibility of SLE or LN have been controversial since the first investigation was reported. We investigated whether the ACE I/D gene polymorphism could become a valuable indicator to predict the risk of SLE or LN, and tried to draw a more robust conclusion by metaanalysis.
Our results indicated that the ACE D allele or DD genotype could predict the onset of SLE for overall populations. Our results were similar to those in nonsensitivity analyses, and there was no publication bias. The conclusions of our study might be robust. We performed subgroup analyses to explore this association in whites, Africans, and Brazilians. In Asians, the DD genotype was associated with the risk of SLE. Further, the pooled OR for D allele was favorable to the SLE group in Asians, although the difference was not statistically significant. So DD homozygous and D allele might be risk factors for SLE risk in Asians. We also found that the pooled OR for D allele or DD homozygous in whites was favorable to the SLE group, although no statistically significant difference was found. D allele/DD genotype might be a risk factor for SLE in whites. In Africans and in Brazilians, no association of ACE I/D gene polymorphism and the risk of SLE was found. The number of included studies of Asians or whites was much larger than that of Africans or Brazilians (Asians: 9; whites: 6; Africans: 3; Brazilians: 1). Results for Asians or whites might be more convincing than those for Africans or Brazilians.
LN is a common and potentially severe complication of SLE52. We performed a metaanalysis for LN versus control. An association of the DD genotype with the onset of LN was observed. Further, the pooled OR for the D allele was favorable to the LN group, although no statistically significant difference was found. DD genotype/D allele might be a factor in LN risk susceptibility. The results from the sensitivity analysis were the same as those of the nonsensitivity analysis, and no publication bias was found. The results for overall populations might be robust to some extent. However, the number of included studies for Asians or Brazilians was small, and it was difficult to draw a convincing conclusion for Asians or Brazilians.
The HWE test was performed and the result that the genotype distributions in the control group significantly deviated from HWE was excluded from our sensitivity analysis. In our study, the genotype distributions of the control group in 1 report36 were not in HWE. This was a factor that could cause bias and was excluded from our sensitivity analysis. The disequilibrium of the genotype distributions of the control group might be caused by methodological weaknesses, such as biased selection of subjects, genotyping errors, or population stratification53. In our study, we also provided the results of HWE for the SLE group. We found that the case groups in Guan, et al27 and Hussain, et al42 were not in HWE, and the case group for overall populations/Africans in Kaufman, et al41 also was not in HWE. In the case of genetic association, deviation from HWE can be expected in cases, while it should not be strong in controls54. So the deviation from HWE of those studies reflected the positive association between ACE I/D gene polymorphism and risk for SLE.
In Guan27, Hussain42, and Kaufman41, the D allele and DD homozygous might be associated with the onset of SLE. Further, DD genotype was associated with the risk of LN, and the D allele was a risk factor for LN (although the difference was not statistically significant). We speculated that the mechanisms were as follows: the DD homozygous or D allele was associated with elevated circulating and tissue ACE activity, and the increased ACE could raise the risk of SLE and LN19,50,51. So the DD homozygous or D allele might be associated with susceptibility to SLE/LN.
There were also studies of the association of ACE I/D gene polymorphism and some diseases using the metaanalysis method. They found that ACE I/D gene polymorphism was associated with the susceptibility of some diseases correlating with the vascular system. Samani, et al55 conducted a meta-analysis to investigate the association between ACE I/D gene polymorphism and risk of myocardial infarction, and found that D allele and DD genotype were associated with the onset of myocardial infarction. Qin, et al46 performed a metaanalysis to explore the relationship between ACE I/D gene polymorphism and risk of IgA nephropathy, and found that the D allele and DD homozygous were associated with the onset of IgA nephropathy. Zintzaras, et al56 performed a metaanalysis to investigate the relation between ACE I/D gene polymorphism and coronary artery disease, and found that the D allele and DD genotype were associated with the onset of coronary artery disease. Sayed-Tabatabaei, et al57 conducted a meta-analysis and showed evidence of a positive association between the D allele of the ACE gene and common carotid intima-media thickness.
Our results indicated that there was an association between the D allele or DD genotype and SLE risk, and DD homozygous was associated with the risk of LN. The outcome might be robust. We speculated that the increased ACE level was associated with the risk of SLE/LN. However, those findings should be regarded cautiously because many other factors, such as language bias, small sample size of the included report, limited statistical power, heterogeneity of enrolled cases, variable study designs, and different interventions could have affected the results.
Language bias might affect our conclusion. We analyzed the gene distribution of ACE I/D polymorphism in English reports and Chinese reports separately (detailed data not shown). In the metaanalysis for English reports, we found that the DD genotype was associated with the risk of SLE but not with risk for LN, and that the D allele was not associated with risk for SLE/LN. In the analysis for Chinese reports, the D allele and DD genotype were associated with susceptibility to SLE/LN. As in Zintzaras, et al56 and Sayed-Tabatabaei, et al57, the D allele and DD genotype might be genetic markers to predict the risk of SLE/LN in Chinese people.
The sample size in some studies was small and might have affected the strength of our outcome. We excluded those reports with a sample size < 80. Finally, 9 reports27,28,29,31,32,35,37,39,41 for SLE and 227,31 for LN were included in the metaanalysis. We found that ACE I/D polymorphism was not associated with risk for SLE/LN in the analysis for overall populations and subgroup analysis according to different races (detailed data not shown). However, the number of included reports was small and the conclusion was not robust.
Our study supports the notion that the D allele or DD genotype is associated with risk for SLE, and there is an association between DD homozygous and risk for LN. However, more association investigations with larger sample sizes are required to clarify the role of the ACE I/D gene polymorphism in predicting the risk of SLE/LN.
Acknowledgment
The authors gratefully acknowledge the most helpful comments received from Prof. Liang Rong, Department of Pediatric Neonatology, Baylor College of Medicine, Houston, Texas, USA.
Footnotes
-
T-B. Zhou, Y-G. Liu, and N. Lin are joint first authors of this report.
- Accepted for publication November 21, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.