
Regular, vigorous physical exercise confers numerous benefits. These include markedly postponing disability, prolonging life, strengthening bones, improving cardiac function and quality of life, reducing frailty, and retarding progression of aging markers in many organ systems1,2,3,4. Effects of exercise upon radiographic osteoarthritis (OA), particularly of the knee, have also been examined, partly because the original “wear and tear” hypothesis of OA development suggested that excessive weight-bearing exercise might cause accelerated joint damage and might result in more knee replacement surgery.
The “wear” component of this hypothesis has been generally disproven, although elements of the “tear” component remain in the context of contact sports5. Pain-free exercise does not appear to accelerate OA development, and has been postulated to have a protective effect. For example, after accounting for body mass index (BMI), the Framingham Study6,7,8 reported no association between exercise and knee OA. Rogers, et al2 showed a protective effect of exercise for knee OA. Manninen, et al9 found a dose-response protective exercise effect for knee arthroplasty, and Racunica, et al10 showed an exercise benefit to knee articular structures during development. Similarly, Jones, et al11 found healthier cartilage in exercising children. Recently, we observed a trend toward fewer knee arthroplasties in vigorous lifetime exercisers, principally long-distance runners over hard surfaces12. Epidemiologic studies of OA identify age, female gender, and obesity as major risk factors for knee OA, but they do not include exercise (absent trauma) as a risk factor1,13,14. Indeed, numerous reports describe exercise as currently perhaps the single most important treatment for OA.
Responding to issues related to longterm risks of exercise, our group initiated a prospective longitudinal study of exercise, disability, aging, joint destruction, and mortality in 1984. We developed primary datasets with standardized protocols, cohort membership fixed at baseline, and validated Health Assessment Questionnaire (HAQ) endpoints. We have maintained the original protocol consisting of annual HAQ assessments over 25 years, which has included serial radiographs that were read blindly by multiple observers. To our knowledge, this is the only longitudinal study of knee OA developed primarily to address these issues and which studies the prime ages of OA development.
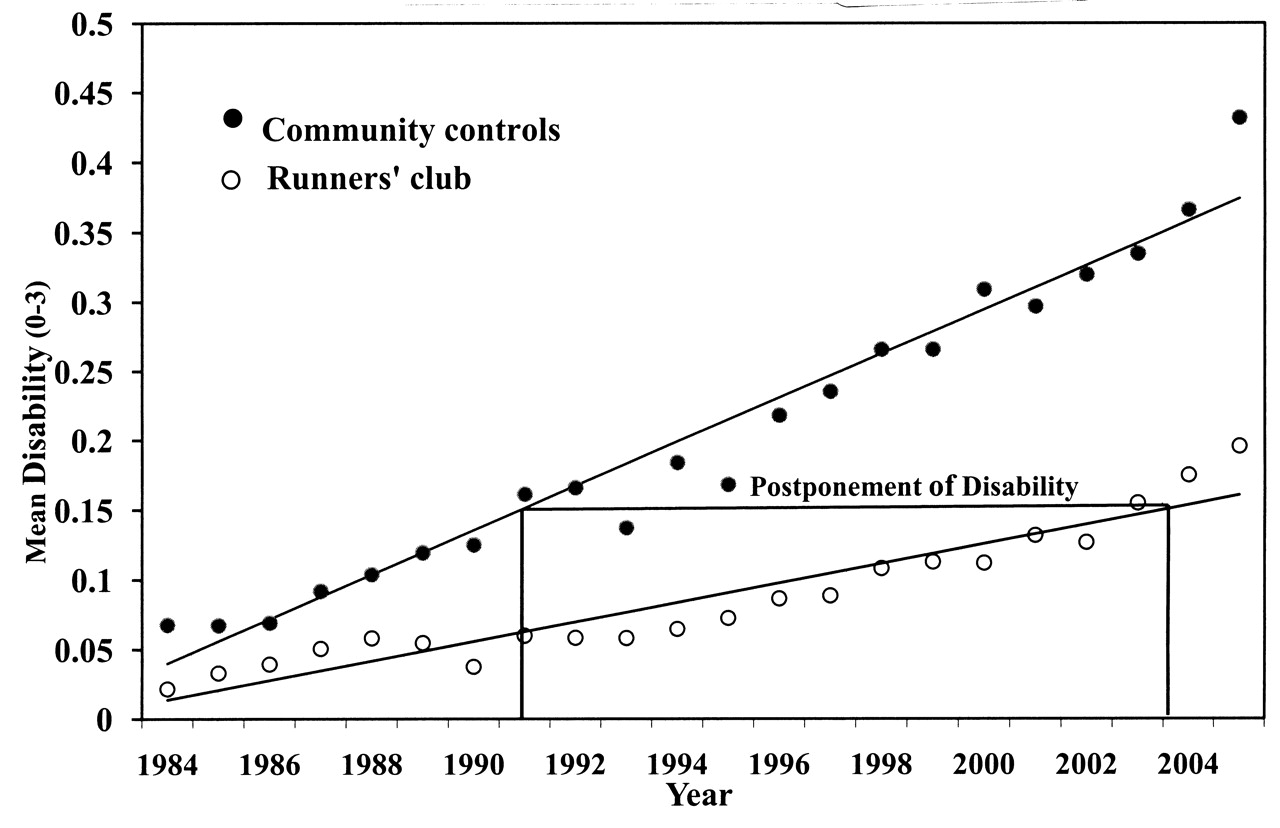
We recently reported radiographic findings after 21 years of study12,14,15. Current long-distance runners (n = 538) and community control (n = 423) cohorts had been matched for age at baseline in 1984 (58 yrs) and for education (16 yrs). After 21 years, exercise levels differed markedly between groups: 287 vigorous exercise minutes per week in the runners versus 138 minutes in the controls. We then studied a subsample of 51 runners and 62 controls who had radiographs of the knees and hips at 4-year intervals. Both groups at last observation were 79 years old and of normal weight (BMI 22 vs 24, respectively), and only 1% smoked12. After 21 years, the runners group had less than one-half the cumulative disability and about one-half the mortality rates of the controls (p < 0.001). Disability was postponed by 12 years in the exercise cohort (Figure 1).

{kind=link}
Progression of disability by group over 21 years. Regression lines are derived from linear mixed models and adjusted for age, sex, body mass index, smoking, and initial disability level. Time to reach a modest disability level of 0.15 was postponed by a full 12 years for the exercise cohort compared with controls1. Reprinted from Chakravarty EF, et al. Arch Intern Med 2008;168:1638–46; with permission.
Radiographic scores in the radiographic subsample12 trended (p = 0.21) in favor of exercise as protective against knee OA (knee replacement 0 vs 2, respectively; knee destroyed 1 vs 5; knee nearly destroyed 5 vs 11). The prevalence of radiographic OA was similarly lower in exercisers (20% vs 32%), as were total knee scores. Other studies have also reported similar findings1,3,10,11, suggesting a protective association of exercise for radiographic OA as well as disability. Importantly, we found very strong and statistically significant evidence for positive effects of exercise on disability (Figure 1).
In a recent issue of The Journal, authors of an article16 and an accompanying editorial17 concluded that exercise intensity adequate to break a sweat increases likelihood for knee replacement. This is an unconventional interpretation that is contrary to current evidence and biomechanics. The quadriceps provide a means to reduce static force on the articular surface, and quadricep weakness is a risk factor for the development of symptomatic knee OA. Similarly, there are numerous problems with their methodology. The mean observation period prior to knee replacement averaged only 1.6 years. The authors used unvalidated measures for physical activity and for disability. There were no radiographic data, and the timing of the endpoint, knee surgery, is subjective. There was also exclusion of social factors unrelated to disease severity, such as access to care, presence of comorbidities, smoking behavior, income level, insurance coverage, waiting list times, and others that may affect the decision to operate or to wait. Absent imaging of any kind, there were no data on incident or prevalent OA. Moreover, there are additional larger analytic issues.
The independent variable, “physical activity level,” is used as a surrogate for a biomechanical measure. It is defined by a cardiopulmonary symptom, “puffing and sweating” rather than the estimated impact or weight-bearing effects, both of which would be the variables needed to test the hypothesis of effect of exercise on OA. Analyses of “vigorous activity” might be expected to be the most sensitive, but results in this category were inconsistent across categories and were not regularly monotonic. As noted, the established risk factors for knee OA are age, female gender, and BMI. This is confirmed in this article16, with an (obese) BMI of 30 in those with knee replacements versus a BMI of 27 in those with no joint replacements, age 68 years (older) versus 63, and female gender 64% versus 60%. Thus, established risk factors more than sufficient to account for the observed results without attention to exercise were already present at baseline. There are no adequate methods to adjust for these major confounders and colinearities.
Further, the reported physical activity levels are inconsistent with the literature and with common sense. Those receiving knee replacements are older obese women, with reportedly higher physical activity levels than younger, leaner men! This brings into question the credibility of the measure. This may have resulted from self-report bias, such that the interpretation of the item is different for different subgroups (e.g., sweating in obese women), coding irregularities, or perioperative physical therapy. There are inconsistencies in the data between ascribed activity levels, participation in moderate to heavy physical exertion at work, and tendency to report physical function limitations. These again suggest difficulties in the coding process.
Hippocrates instructed physicians to “First, do no harm.” Rheumatologists share this duty. Simplified interpretation of limited data, especially when contrary to biomechanical sense and existing evidence, could result in a perception that less activity is protective for joints and could mislead patients to exercise less with substantial harm to the health of the public. There was a time cardiologists made this mistake when exercise following heart attacks was severely limited, on the speculation that the myocardial scar following a heart attack would be smaller if the patient was kept at complete bed rest for 6 weeks. Cardiologists now recommend increasing physical activity within days after myocardial infarction, resulting in better functional outcomes and fewer complications.
Rheumatologists also must “Do no harm” and advocate for increased, not decreased, activity. Linking “breaking into a sweat” and the risk of osteoarthritis16 may seem funny and tongue-in-cheek17, but there is little humor in this implication. Exercise is arguably the most important treatment for OA1,2,18,19. It strengthens the joint structures, retards disability, stabilizes the joint, improves metabolism in the articular cartilage, increases endurance, improves quality of life, and wards off comorbidities. It has few problems over a very wide range of lifetime activity1,2,3. Its value is recognized by medical and federal authorities, American College of Rheumatology guidelines, self-management programs, international health organizations, and the media18,19. Rheumatologists must aggressively advise colleagues and encourage patients to examine their physical function activities and to improve exercise activities whenever possible.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.