
Abstract
Objective. To clarify the influence of individual joint impairment on functional capacity through a retrospective study with a 3-year interval, using a large cohort of Japanese patients with rheumatoid arthritis (RA).
Methods. Subjects included 3457 patients with RA who participated in a large observational cohort study in both April 2004 and April 2007; 43 joints were assessed and classified into 10 joint areas. Impairment of each joint area was scored based on the presence of swelling or tenderness: score 0 (no swelling or tenderness in either joint), score 1 (swelling or tenderness in a unilateral joint), and score 2 (swelling or tenderness in bilateral joints). Score change was defined as the difference between scores from 2004 and 2007. The Japanese validated version of the Health Assessment Questionnaire is the J-HAQ; ΔJ-HAQ score was determined by subtracting J-HAQ score in 2007 from that in 2004. The relationship between score change and ΔJ-HAQ score, and the effect of joint impairment on ΔJ-HAQ score were assessed.
Results. Major joint areas that contributed to ΔJ-HAQ score included the wrist (31%), shoulder (21%), knee (13%), and ankle (10%). The shoulder, wrist, knee, and ankle in the worsening group were associated with a J-HAQ score increase of 0.13 to 0.18 compared to the improvement group.
Conclusion. Our study demonstrated that impairment of the shoulder, wrist, knee, and ankle significantly affects functional capacity in patients with RA. Care of these joints is suggested to be especially important for better functional outcomes.
- RHEUMATOID ARTHRITIS
- FUNCTIONAL DISABILITY
- JOINT INVOLVEMENT
- FUNCTIONAL OUTCOME
Rheumatoid arthritis (RA) is characterized by persistent polyarthritis and progressive joint damage that lead to functional disability. Suppression or improvement of functional disability is one of the major goals of RA treatment. Previous studies showed that Health Assessment Questionnaire (HAQ) score is associated with disease activity, joint distraction, disease duration, age, sex, muscle strength, work disability, and mortality1,2,3,4,5,6. RA disease activity has been shown to be significantly associated with decreased HAQ scores throughout the course of RA1,2.
Functional disability in patients with RA has both reversible and irreversible components7. The reversible component involves inflammation, indicating that it can be improved by medical intervention. The irreversible component is associated with joint destruction and deformity; this can be ameliorated by surgical treatment or physical therapy. Therefore, care of individual joints is as important as systemic treatment to avoid worse functional outcomes. The influence of joint impairment on functional disability may differ among individual joints. However, only a few studies with relatively small samples have been conducted on the effect of individual joint impairment on functional disability.
We retrospectively investigated the effect of individual joint impairment on functional capacity during a 3-year period using a large observational cohort of Japanese patients with RA.
MATERIALS AND METHODS
Cohort database
We have established an observational cohort of patients with RA who were treated at the Institute of Rheumatology, Tokyo Women’s Medical University, beginning in October 20008, the Institute Of Rheumatology Rheumatoid Arthritis (IORRA) cohort. All patients with RA diagnosed using American College of Rheumatology criteria9 were registered, and their clinical information was collected biannually (April and October) when they visited the outpatient clinic; each biannual survey is considered to be a phase. Clinical information consisted of 3 components: (1) physician evaluation, including the number of tender joints, number of swollen joints, and visual analog scale (VAS) score of disease activity (physician VAS); (2) patient information, including VAS for pain (pain VAS), VAS for general health (global VAS), disability level using the Japanese validated version of the Health Assessment Questionnaire (J-HAQ) score8, comorbidities, and medications taken during the period; and (3) patient laboratory data. Data collected from each component were integrated into 1 database for analysis.
Patients and assessment of joints
A total of 4842 and 5262 patients participated in the April 2004 and April 2007 IORRA phases, respectively. Study subjects included 3457 patients who participated in both these IORRA phases. In those patients, 43 joints were assessed: neck, bilateral shoulders, elbows, wrists, finger proximal interphalangeal (PIP) joints, interphalangeal joints of the thumb, metacarpophalangeal (MCP) joints, hips, knees, ankles, and metatarsophalangeal (MTP) joints.
Statistical analysis
The 43 joints were classified into 10 joint areas: neck, shoulder, elbow, wrist, MCP, PIP, hip, knee, ankle, and MTP. Right and left joints were regarded as a single area. Impairment of each of the 10 joint areas was scored based on the presence of swelling or tenderness: score 0 (no swelling or tenderness in either joint), score 1 (swelling or tenderness in a unilateral joint), and score 2 (swelling or tenderness in bilateral joints).
The change of joint impairment from 2004 to 2007 was evaluated by score change, which was defined as the difference between scores from 2004 and 2007. The score change was categorized into 4 groups: improvement (score change > 0), quiescence [both scores (2004 and 2007) = 0], no improvement [no score change (excluding quiescence)], and worsening (score change < 0). Thus, score change indicates the variation of joint impairment over years. ΔJ-HAQ score was defined as the value of subtracting J-HAQ score in 2007 from that in 2004. To investigate the relative contribution of score change to ΔJ-HAQ score and the effect of score change on ΔJ-HAQ score, we constructed a linear model, which had ΔJ-HAQ score as the objective variable and joint areas as the explanatory variables. The relative contribution of joint impairment to ΔJ-HAQ score was estimated using the analysis of variance table of this model, and the effect of joint impairment on ΔJ-HAQ score was evaluated using the parameter estimates of this model.
RESULTS
The basic characteristics of the 3457 patients who participated in this study are shown in Table 1. The mean age of the 84.6% women and 15.4% men was 57.4 years (range 18.0 to 88.0 yrs). Mean disease duration was 11.3 years (range 0 to 60.0 yrs). Rheumatoid factor positivity was 73.0%. Disease Activity Score 28 (DAS28) and J-HAQ score were 3.42 (range 0.01 to 8.69) and 0.73 (range 0.0 to 3.0), respectively. The data showed that 91.6% of patients were treated with disease-modifying antirheumatic drugs.
Baseline characteristics of 3457 patients with rheumatoid arthritis. The mean age of the 84.6% women and 15.4% men was 57.4 years. Mean disease duration was 11.3 years. Rheumatoid factor positivity was 73.0%. DAS28 and J-HAQ scores were 3.42 and 0.73, respectively; 91.6% of patients were treated with disease-modifying antirheumatic drugs.
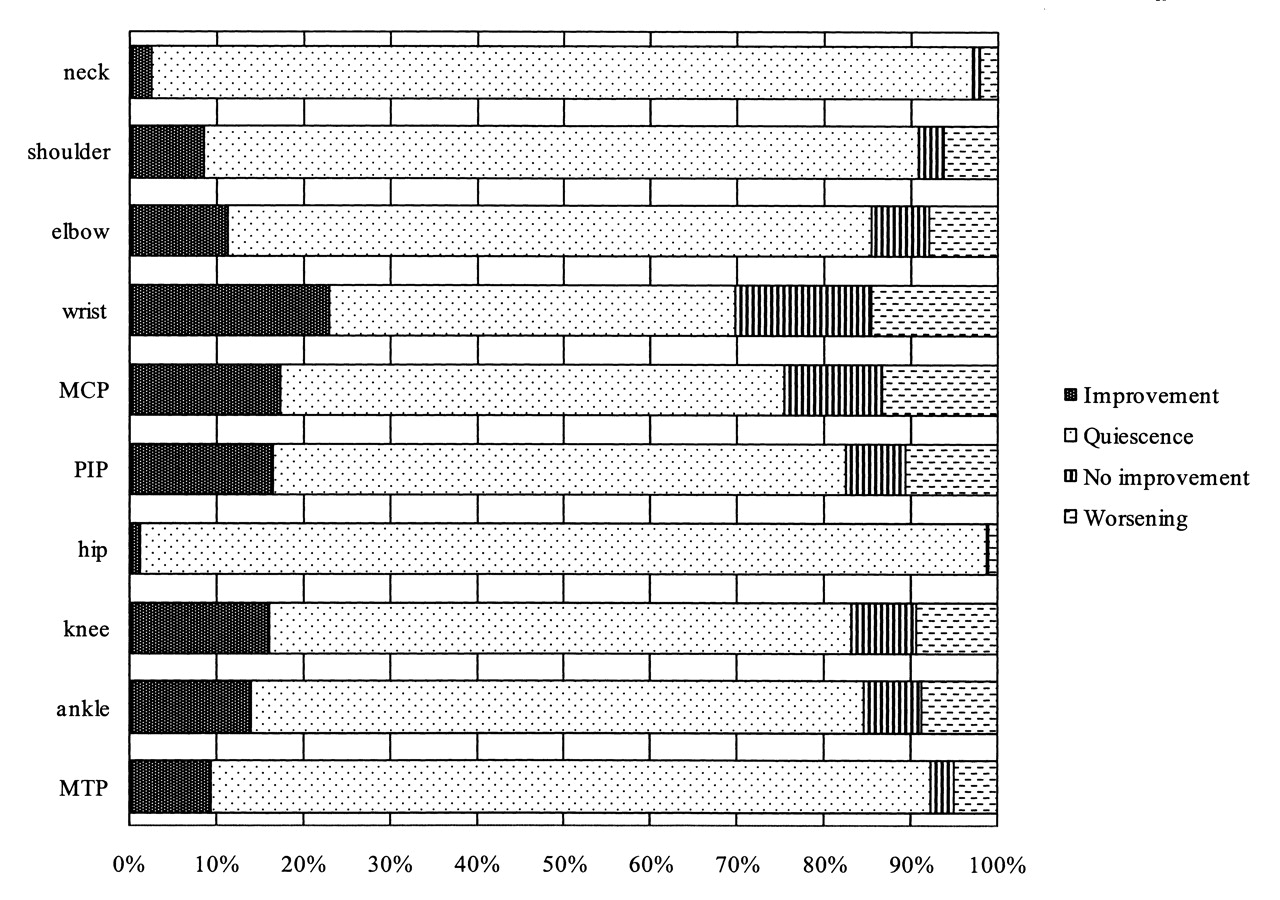
The change of joint impairment evaluated by score change of each joint area is indicated in Figure 1. Improvement was most frequently observed in the wrist (22.8%), followed by MCP (17.3%), PIP (16.3%), knee (15.9%), ankle (13.9%), elbow (11.1%), MTP (9.4%), and shoulder (8.4%), while worsening was also most frequently observed in the wrist (14.6%), followed by MCP (13.4%), PIP (10.6%), knee (9.4%), ankle (8.9%), elbow (7.9%), shoulder (6.4%), and MTP (5.0%). The score change in neck or hip was classified as quiescence in most patients. For each joint area, the proportion of patients categorized into the improvement group was higher than that categorized into the worsening group.

The change of joint impairment from 2004 to 2007 was evaluated by score change, defined as the difference of score of individual joint areas between 2004 and 2007. Score change was categorized into 4 groups: improvement, quiescence, no improvement, and worsening.
Relative contribution of score change on ΔJ-HAQ score
The major joint areas that most frequently contributed to ΔJ-HAQ score were the wrist (31%), shoulder (21%), knee (13%), and ankle (10%). The effect of score change in small joints (PIP, MCP, and MTP) on ΔJ-HAQ score was modest. Although only a small number of patients showed positive or negative score changes of the neck, such changes showed a relatively large effect on ΔJ-HAQ score (Figure 2).

{kind=link}
{kind=link}
The change of joint impairment from 2004 to 2007 was assessed by score change. ΔJ-HAQ score was defined as the value of subtracting the Japanese Health Assessment Questionnaire (J-HAQ) score in 2007 from that in 2004. The relative contribution of score change to ΔJ-HAQ score was examined using ANOVA.
Effect of score change on ΔJ-HAQ score
The effect of score change on ΔJ-HAQ score was evaluated for the shoulder, wrist, knee, and ankle joint areas. A multivariate analysis showed that worsening compared to improvement of the shoulder, wrist, knee, and ankle related to an increase of 0.18 (95% CI 0.11 to 0.25), 0.17 (95% CI 0.12 to 0.21), 0.13 (95% CI 0.07 to 0.18), and 0.13 (95% CI 0.07 to 0.18) in J-HAQ score, respectively (Table 2). During the study period, worsening of score change in each joint area was significantly associated with an increase of 0.13 to 0.18 in J-HAQ score.
The effect of change in joint impairment on ΔJ-HAQ evaluated by multivariate analysis. The shoulder, wrist, knee, and ankle in the worsening group were associated with a J-HAQ score increase of 0.18, 0.17, 0.13, and 0.13, respectively, compared to the improvement group.
DISCUSSION
Physical function is involved to some extent in most cases of RA. Suppression or improvement of functional disability is a major goal of RA treatment. HAQ score is the most widely used measure to assess physical function of patients, and J-HAQ score represents the validated Japanese version. In this retrospective study with a 3-year interval, we showed that the wrist, shoulder, knee, and ankle joints made the largest contribution to J-HAQ score change during the 3 years. Previously, our cross-sectional study showed that the shoulder, knee, elbow, wrist, and ankle most commonly contributed to J-HAQ score10; changes in most of these joint areas were shown to be associated with longterm functional prognosis.
Worsening of arthritis in the shoulder, wrist, knee, and ankle was demonstrated to lead to a 0.13 to 0.18 increase in J-HAQ score as compared to improvement of arthritis in those joints. The mean J-HAQ score of subjects at study entry was 0.73 (SD 0.74; Table 1). The minimally important difference (MID) for HAQ score improvement in RA clinical trials has been reported to range from −0.22 to −0.2411,12,13. However, Pope, et al showed that the MID of HAQ scores in clinical practice was −0.09 for improvement and 0.15 for worsening14. Thus, the 0.13 to 0.18 increases of J-HAQ scores demonstrated in the study deserve attention from a clinical point of view.
Our study revealed that impairment of the shoulder, wrist, knee, and ankle significantly affected functional outcome measured by HAQ score. Recently, a patient-centered approach has been widely applied in RA management15. Thus, our study may provide a more efficient guideline for a multidisciplinary RA team that includes rheumatologists, orthopedic surgeons, nurses, and physical and occupational therapists.
To date, only limited studies with relatively small sample sizes have been conducted to address the effect of impairment of individual joints on physical function. The HAQ score has been reported to be associated with radiographic damage of large joints16. Our previous cross-sectional study indicated that the shoulder, knee, elbow, wrist, and ankle made the largest contribution to HAQ score10. Recently, Häkkinen, et al evaluated 66 joints and investigated the associated total and subdimensions of the HAQ score17. These authors indicated that range of motion of the wrist, shoulder, and knee is associated with total HAQ score.
The studies described above as well as the current study failed to find any associations between HAQ score and small joints in the hands and feet. In our cross-sectional study10, the contribution of these small joints to HAQ score was modest. Impairment of small joints can be associated with particular subdimensions of HAQ score, although the previous studies did not indicate such an association in either RA17 or juvenile idiopathic arthritis18. For activities such as dressing, arising, eating, walking, hygiene, reach, and grip, coordination among joints is necessary18, although the contribution of small joints to these activities may be minor. The relatively large contribution of the neck to ΔJ-HAQ score is of particular interest, because only a small number of patients showed improvement or worsening, suggesting the important role of neck impairment on functional disability (Figure 1).
Our study has some limitations. First, it was not prospective. However, the study has an advantage of analyzing a large database and the effect of improvement or worsening of joint impairment on functional disability during 2 timepoints. Second, of the 4842 patients who participated in the IORRA survey in April 2004, we were unable to collect data for 1385 from the April 2007 survey, for a variety of reasons, including nonparticipation and incomplete data. This may have affected the results. Third, we did not specify the treatments including surgical procedures used during the study period. Therefore, reasons for the improvement or worsening of individual joints were not identified. Fourth, we did not assess range of motion of individual joints because such data were not included in the IORRA database. In some studies, the association of functional disabilities with joint motion was much stronger than that with tender or swollen joint counts17,19. In the early stages of RA, joint inflammation has been shown to be associated with functional disability, while loss of joint motion becomes increasingly important in prolonged RA3,18,19. However, some prospective studies reported that HAQ score was associated with swollen joint counts1,17,20. Other studies have reported an association between joint inflammation and functional disabilities21,22,23,24. Moreover, the relationship between joint tenderness or swelling and disabilities is relatively complex. Psychological and social effects and noninflammatory pain may contribute to this complexity.
Our results indicate that impairment of the shoulder, wrist, knee, and ankle joints affects functional capacity. Systemic treatments as well as care of these joints are important to prevent or improve functional disability in patients with RA.
Footnotes
-
The IORRA cohort was supported by nonrestricted research grants from 36 pharmaceutical companies: Abbott Japan Co. Ltd., Asahikasei Kuraray Medical Co. Ltd., Asahikasei Pharma Corporation, Astellas Pharma Inc., AstraZeneca K.K., Banyu Pharmaceutical Co. Ltd., Chugai Pharmaceutical Co. Ltd., Daiichi Fine Chemical Co. Ltd., Daiichi Sankyo Co. Ltd., Dainippon Sumitomo Pharma Co. Ltd., Eisai Co. Ltd., GlaxoSmithKline K.K., Janssen Pharmaceutical K.K., Japan Tobacco Inc., Kaken Pharmaceutical Co. Ltd., Kissei Pharmaceutical Co. Ltd., Kowa Pharmaceutical Co. Ltd., Mitsubishi Chemical Medience Corporation, Mitsubishi Tanabe Pharma Corporation, Nippon Chemiphar Co. Ltd., Nippon Shinyaku Co. Ltd., Novartis Pharma K.K., Otsuka Pharmaceutical Co. Ltd., Pfizer Japan Inc., Sanofi-Aventis K.K., Santen Pharmaceutical Co. Ltd., Sanwa Kagaku Kenkyusho Co. Ltd., Sekisui Medical Co. Ltd., Taisho Toyama Pharmaceutical Co. Ltd., Takeda Pharmaceutical Company Ltd., Teijin Pharma Limited, Torii Pharmaceutical Co. Ltd., Toyama Chemical Co. Ltd., UCB Japan Co. Ltd., Wyeth K.K., and Zeria Pharmaceutical Co. Ltd.
- Accepted for publication October 27, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.