
Abstract
Objective. Vertebral fractures occur in patients with juvenile idiopathic arthritis (JIA), but data on their frequency and causes are scarce. Our cross-sectional study evaluated prevalence of compression fractures and associated factors in a high-risk pediatric population with severe JIA.
Methods. Children and adolescents with a history of treatment-resistant polyarticular-course JIA for ≥ 5 years or systemic arthritis for ≥ 3 years were recruited. Clinical examination, dietary recall, laboratory measurements, bone mineral density (BMD) measurement by dual-energy X-ray absorptiometry, and spinal radiography were performed.
Results. Our study included 50 patients (41 girls), of whom 6 (12%) had systemic arthritis, with a median age of 14.8 years (range 7.0–18.7 yrs) and median disease duration of 10.2 years (range 3.9–16.8 years). Ninety-four percent had used systemic glucocorticoids (GC); the median total duration of GC treatment was 7.1 years (range 0–15.5 yrs). The median weight-adjusted cumulative GC dose for the preceding 3 years was 72 mg/kg (range 0–911 mg/kg). The median bone age-corrected lumbar spine and whole-body areal BMD Z-scores were −0.8 and −1.0, respectively. Twenty-two percent had vertebral fractures, mostly thoracic. Compression fractures were associated with high disease activity, high body mass index (BMI), and high recent cumulative GC dose, but not with disease duration or BMD. Thirty percent had sustained at least 1 peripheral low energy fracture. Twenty-six percent were deemed to have significantly compromised bone health.
Conclusion. Severe JIA is associated with a significant risk of vertebral compression fractures. Associated factors include high disease activity, high BMI, and high recent GC exposure. Further studies are needed to establish optimal prevention and treatment guidelines.
- VERTEBRAL FRACTURE
- OSTEOPOROSIS
- BONE MINERAL DENSITY
- SPINE
- JUVENILE IDIOPATHIC ARTHRITIS
There is increasing evidence that secondary osteoporosis may be a significant problem in children with various chronic illnesses, including hematologic malignancies, neuromuscular diseases with motor disability, diseases requiring solid organ transplants, and chronic inflammatory diseases such as Crohn’s disease and various chronic rheumatologic conditions1,2,3,4,5,6,7,8. Juvenile idiopathic arthritis (JIA) includes all forms of chronic arthritis of unknown origin with onset before 16 years of age. The current classification9 identifies different subtypes with a wide range of severity and variable course. Patients with JIA have been reported to have lower bone mineral density (BMD)10,11,12,13,14 and more fractures than their healthy peers15, even without prior prolonged glucocorticoid (GC) exposure8. The predisposing factors include chronic inflammation, hormonal and nutritional disturbances, GC therapy, and limited weight-bearing physical activity16.
Vertebral fracture is a serious complication of impaired bone strength and a sign of evident osteoporosis. Some studies have reported vertebral compression fractures in children with JIA6,7,8,17,18. In these reports, the prevalence has been variable and the clinical and treatment-related determinants of compression fractures have remained largely unknown. As the data are still limited, we investigated the prevalence of compression fractures and associated factors in a high-risk pediatric population with severe polyarticular or systemic JIA.
MATERIALS AND METHODS
We carried out the study at Heinola Rheumatism Foundation Hospital, a tertiary center for complicated pediatric rheumatology in Finland. The total JIA patient population of the hospital is roughly 700 yearly, patients with polyarticular or systemic disease representing about 60%. We recruited children and adolescents with a history of refractory disease with continuous disease activity or recurrent flares requiring permanent antirheumatic medication since the diagnosis of JIA. Patients were diagnosed according to the revised criteria9. The inclusion criteria were (1) age < 19 years; (2) polyarticular JIA (polyarthritis, extended oligoarthritis, or psoriatic arthritis with ≥ 5 affected joints) for ≥ 5 years; or (3) systemic arthritis for ≥ 3 years. Patients with systemic JIA overall have higher risk for compression fractures than patients with polyarticular JIA7,8 and therefore a requirement for shorter disease duration was used. In order to avoid selection bias, consecutive patients were recruited; all who fulfilled the inclusion criteria were recruited and none were excluded. Altogether, 55 patients were recruited; 5 declined due to lack of interest and 50 consented. The cross-sectional study protocol included clinical assessment, questionnaires, radiographs of the spine and left hand, and bone densitometry during a study visit. The study was approved by the Helsinki University Hospital Ethics Committee and written informed consent was obtained from all participants and/or their parents.
Clinical characteristics
Medical records were reviewed for disease and treatment characteristics. The total duration of GC treatment was determined and the cumulative systemic GC dose, as prednisolone equivalents, was calculated for the preceding 3 years to determine recent GC exposure. Patients were clinically evaluated by a pediatric rheumatologist. Height, weight, body mass index (BMI; kg/m2), number of active joints (including swollen joints and tender joints with limited range of motion), and other signs of disease activity were recorded. Pubertal maturation was assessed according to Tanner19. Global assessment of overall well-being [assessed by parents or patients aged > 15 yrs, on a visual analog scale (VAS)], physician’s global assessment of disease activity, and Childhood Health Assessment Questionnaire (CHAQ) were determined before imaging studies. Inactive disease on medication was defined according to Wallace, et al20. Questionnaires on the patient’s physical activity6, back pain, and fracture history were filled out by patients and/or their parents. Fractures were regarded as high-energy fractures when the patient was involved in a fall from a height ≥ 3 meters or was involved in accidents with motor vehicles; other fractures were regarded as low-energy fractures. Present diet was assessed by a 3-day dietary recall21 (completed by 34 patients) and average daily intakes of calcium (Ca) and vitamin D were calculated by a registered dietician with the Diet32 program (version 1.4.4.1; Aivo Finland Corp., Turku, Finland).
Imaging studies
Spinal radiographs (anteroposterior and sagittal projections) were obtained. All radiographs were assessed by 2 experienced radiologists (STS, LK) who were blinded to patients’ clinical diagnosis and status. The radiologists first independently analyzed the visibility and morphology of each vertebra. The final conclusions were reached by consensus, and in cases with discrepant/borderline findings the milder alternative was reported. Compression fractures were classified using a pediatric grading system1 as anterior wedge deformities (only the anterior part of the vertebra compressed) or compression deformities (the middle and/or posterior part of the vertebra also compressed). Abnormal changes were further classified as mild (Grade 2a; 20%–49% anterior height reduction) or severe (Grade 2b; ≥ 50% anterior height reduction) wedge deformities; or mild (Grade 3a; vertebral middle and/or posterior height reduction 20%–29%) or severe (Grade 3b; vertebral middle and/or posterior height reduction ≥ 30%) compression deformities1. None of the patients had vertebrae with isolated posterior height reduction. Bone age was determined from a plain radiograph of the left hand by a pediatric endocrinologist (OM) according to Greulich and Pyle22; it was considered delayed (in 42% of the patients) or advanced (in 6%) when it differed from calendar age by > 1 year22.
Areal bone mineral density (aBMD; g/cm2) for lumbar spine (LS; L2 to L4) and whole-body (WB) was assessed with dual-energy X-ray absorptiometry (DEXA; Lunar Prodigy, GE Lunar, Madison, WI, USA) and compared with reference values23. The values were corrected for bone age; adjusted Z-score values ≤ −2.0 were considered abnormal24. Correction for bone age rather than height age was considered appropriate as delayed puberty is a common complication of a chronic illness and pubertal status of children of the same age and height can vary considerably25. Further, as compression fractures result in height loss, mathematical correction of BMD values for height would result in inappropriately good BMD values in those with compression fractures. Body composition was assessed with the same DEXA device and height-, age-, and bone age-adjusted bone mineral content/lean tissue mass (BMC/LTM) ratios were calculated according to Högler, et al26; similar to the original study26, BMC/LTM Z-score values between −1.0 and +1.0 were considered normal. Bone age and DEXA were not obtained for 1 patient with severe carpal deformities, extreme growth failure, and multiple compression fractures. Two additional patients had lumbar compression fractures and their lumbar BMD results were excluded from data analyses.
Laboratory measurements
Blood samples were drawn between 8 and 11 AM after an overnight fast. Erythrocyte sedimentation rate (ESR), hemoglobin, and serum/plasma concentrations of C-reactive protein, calcium, inorganic phosphate (Pi), alkaline phosphatase (AP), parathyroid hormone (PTH), creatinine (Cr), 25-hydroxyvitamin D (25-OHD), insulin-like growth factor-1 (IGF-1), and IGF binding protein-3 were determined from peripheral blood by standard methods and compared with reference values. Girls over 8 years and boys over 10 years of age were also assessed for gonadotrophin and sex steroid concentrations (follicle-stimulating hormone, luteinizing hormone, and estradiol or testosterone). Urine Ca to Cr ratio (U-Ca/Cr) was determined and values < 0.7 mmol/mmol were considered normal. Vitamin D status was defined based on 25-OHD value according to Misra, et al27 as severe deficiency (< 12.5 nmol/l), deficiency (< 37.5 nmol/l), insufficiency (37.5 to < 50.0 nmol/l), or sufficiency (≥ 50 nmol/l).
Statistical analysis
Descriptive data are reported as median (range or interquartile range; IQR) or as mean with standard deviation. The unpaired 2-tailed Student t test was used to compare means, and the nonparametric Mann-Whitney U test to compare non-normally distributed variables. The chi-square test or Fisher exact test was used to compare nominal data (Statview 5.0.1 for Macintosh; SAS Institute, San Francisco, CA, USA). A p value < 0.05 was considered statistically significant. Pearson’s correlation test was used to test associations between clinical, treatment-related, and biochemical variables and BMD values; and Mann-Whitney U test to screen for factors associated with compression fractures. After screening, a multivariate logistic regression model was used to identify and determine OR with 95% CI for significant associations with compression fractures (SPSS version 17.0; SPSS). Factors included in logistic regression analysis were dichotomized based on distribution of values in the cohort or by clinically relevant cutoffs.
RESULTS
Patients and disease characteristics
The study included 50 patients (41 females; median age 14.8 yrs, range 7.0–18.7 yrs) with systemic arthritis (n = 6), seronegative polyarthritis (n = 27), seropositive polyarthritis (n = 1), extended oligoarthritis (n = 14), or psoriatic arthritis (n = 2; Table 1). Their median disease duration was 10.2 years. Forty-eight patients (96%) had signs of active disease during the preceding 6 months20; the 2 patients taking medication at remission had had active disease during their total disease duration of 10 and 14 years. The median height Z-score was −1.2; 13 patients (26%) had short stature (height Z-score < −2.0). After correction for bone age, the height Z-score was < −2.0 in 7 patients (14%). The median BMI Z-score was +0.8; 10 patients had a Z-score > +2.0. Ca and vitamin D supplements were used by 47% and 59% of patients, respectively, and the total intakes were adequate in 85% and 62%. Forty-six percent of patients participated normally in physical education at school; 80% had a leisure time sport activity (minimum duration 30 min) at least twice a week. The 5 patients who declined to participate did not differ significantly from the participants in regard to diagnosis (all 5 had seronegative polyarthritis), age at diagnosis (mean 1.7 vs 3.8 yrs; p = 0.11), duration of disease (13.4 vs 10.5 yrs; p = 0.089) or GC treatment (10.7 vs 7.2 yrs; p = 0.067), or anthropometric measures.
Demographic data and clinical characteristics of the 50 study subjects with JIA. Data are shown as median with interquartile range (IQR; 25th and 75 th percentile values) unless otherwise indicated.
Medications
Patients were using mostly multiple disease-modifying antirheumatic drugs (Table 2). Altogether, 45 patients (90%) were currently receiving biologic drug treatment, mostly tumor necrosis factor-α (TNF-α) antagonists; only 3 had never received biologic therapy. At the time of the study, 26 patients (52%) were receiving systemic GC therapy. All except 3 patients (94%) had used systemic GC for > 1 year; the median total duration of GC treatment was 7.1 years (IQR 4.5, 10.3). The median cumulative GC dose for the preceding 3 years was 3.2 g (IQR 0.4, 6.0) and the median weight-adjusted cumulative dose was 72.0 mg/kg (IQR 6.8, 130.5). All study patients had received multiple local joint GC injections (up to several hundred), 22 patients had used ocular steroids, and 5 patients had used inhaled steroids. Six patients were receiving growth hormone therapy at the time of the study.
Medications used by the 50 patients at the time of the study.
Six patients had received bisphosphonates (mean duration 23 mo, range 3–37 mo) due to compression fractures (n = 4); multiple peripheral fractures and low BMD (n = 1); or low BMD, active disease, and high-dose GC treatment (n = 1). Two patients had discontinued bisphosphonate therapy 7–10 months (mean 8.5 mo) before the study; 3 patients were still receiving intravenous pamidronate and 1 patient once-weekly alendronate. One patient had received alendronate for 1 month, 4.5 years earlier; this bisphosphonate exposure was considered insignificant regarding the bone health measures. Three patients received calcitonin at the time of the study; the effect of calcitonin on BMD was also considered insignificant28 and these patients’ DEXA values were included in further analyses.
Biochemistry
B-ESR (range 2–129 mm/h) was elevated in 34% of the patients. P-Ca, Pi, and PTH were normal in all but occasional patients with mild hypocalcemia (n = 2), hypophosphatemia (n = 2), hyperphosphatemia (n = 1), and slightly subnormal (n = 1) or supranormal (n = 1) fP-PTH. The median S-AP value was −1.1 SD (range −2.6 to +5.4 SD). Five patients had mild hypercalciuria (U-Ca/Cr 0.71–1.22 mmol/mmol). The median S-25-OHD was 53 nmol/l (range 20–95 nmol/l); 62% were vitamin D sufficient, 24% insufficient, and 14% deficient. There was no significant difference in the mean concentration of S-25-OHD between winter (October–March) and summer (April–September) months (54 vs 55 nmol/l, respectively). S-IGF-1 concentration was subnormal in 7 patients. Concentrations of gonadotropins and sex steroids were in accord with pubertal status and none had evidence of hypogonadism.
Bone health characteristics and associated factors
BMD values of 5 bisphosphonate-treated subjects were omitted from the analyses and a DEXA result was not obtained for 1 patient. The median aBMD Z-scores for the remaining 44 subjects assessed with DEXA (all adjusted for bone age) were −0.8 for LS and −1.0 for WB; the Z-scores were ≤ −2.0 in 4 (9%) and 8 (18%) patients, respectively, when the expected number was 1 (2.5%) patient (p = 0.36 and p = 0.023, respectively). The median Z-score for BMC/LTM was normal when adjusted for height, calendar age, or bone age (Table 3). The subjects with low (≤ −2.0) WB BMD Z-score did not differ from the others in disease duration, disease activity-related measures, or height Z-score, but they were older at disease onset (p ≤ 0.001), older at the time of the study (p = 0.009), and had lower BMI (p = 0.038) at study assessment, and their S-25(OH)-D concentration tended to be lower (45 vs 57 nmol/l, respectively; p = 0.051). Subjects with low (≤ −2.0) LS BMD Z-score were older at disease onset (p < 0.001) but their height Z-scores and other characteristics were comparable to the others. The duration or cumulative dose of GC did not correlate with BMD values. Compared with girls, boys had significantly lower BMC/LTM corrected for height (−1.2 vs +0.2 SD; p = 0.022) and bone age (−1.2 vs +0.2 SD; p = 0.014), but their aBMD Z-scores did not differ. Postpubertal patients had lower bone age-adjusted BMC/LTM (p = 0.045), but otherwise they had similar BMD results compared to prepubertal and pubertal subjects.
Areal bone mineral density (aBMD), obtained by dual-energy x-ray absorptiometry, and whole-body bone mineral content/lean tissue mass (BMC/LTM) ratios in 44 patients (data not available for 1 patient; 5 bisphosphonate-treated patients excluded). Data are median (interquartile range).
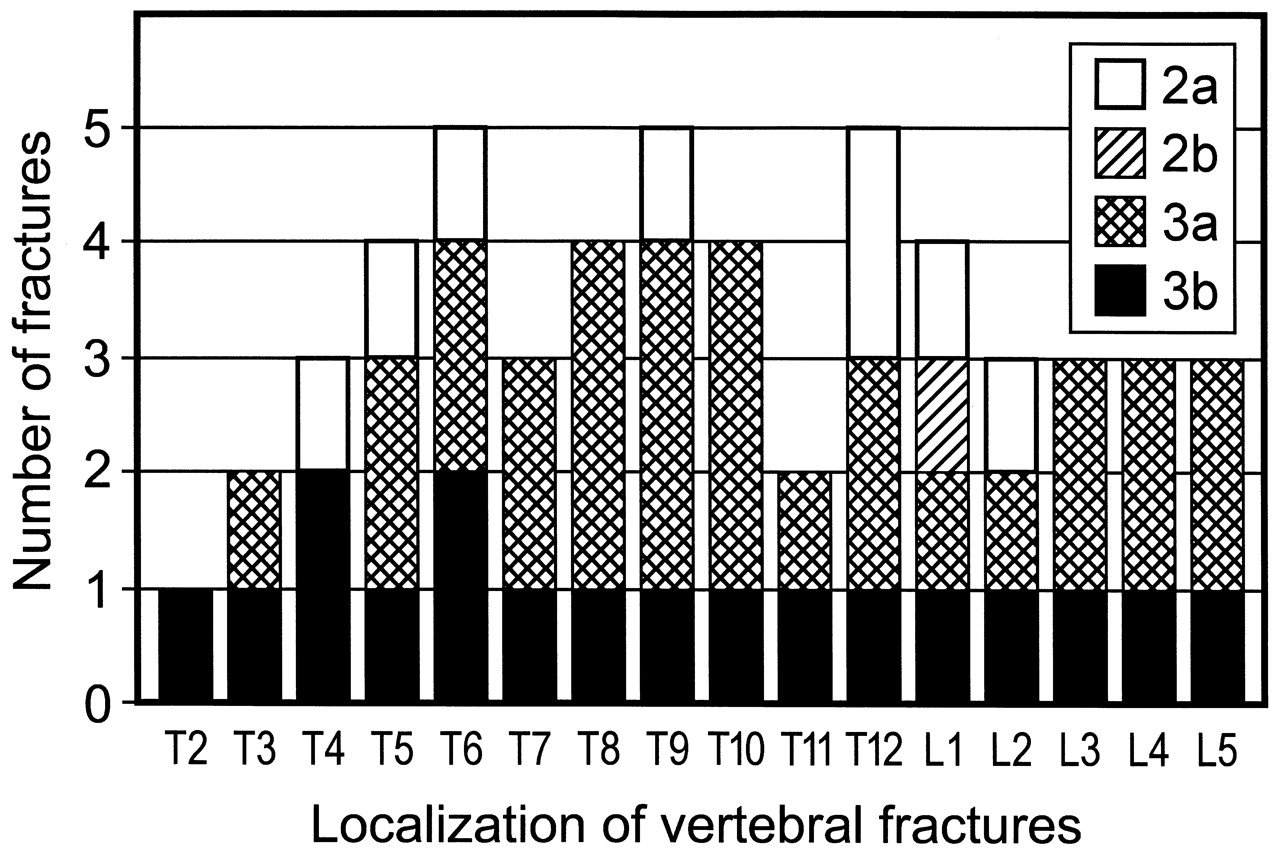
Altogether 11 patients (22%) had vertebral compression fractures, mostly located in the thoracic spine (Figure 1). Five of them were known to have had vertebral compressions at some point after diagnosis of JIA; all 5 had received bisphosphonates. Eight of the 11 patients had more than 1 (from 2 to 16) fractured vertebrae. Patients with fractures were older at diagnosis of JIA, had shorter disease duration, and were heavier than those without fractures. Further, they had more active disease, as evidenced by higher CHAQ score, physician’s global VAS, patient’s global VAS, and ESR values (p < 0.05 for all); they also tended to have more swollen and active joints but these differences were not significant. Most of the 11 patients with vertebral fractures had systemic arthritis (5 patients, 45%) or seronegative polyarthritis (4 patients, 36%). Two patients (18%) had psoriatic arthritis. One of them, despite various combination therapies and multiple biologics, had had an exceptionally active disease since age 2 years, with severe uveitis and growth retardation; she had Grade 3b fractures from T2 to L5. Two patients with compression fractures had never had back pain and 5 had back pain less than once monthly. Only 1 had back pain daily and 3 patients weekly. Subjects with spinal fractures had significantly higher total and weight-adjusted recent cumulative GC exposure, and also higher current weight-adjusted GC dose than patients without fractures (Table 4). LS and WB aBMD values, BMC/LTM ratio adjusted for height, age or bone age, history of back pain or peripheral fractures, and biochemical measures did not differ between the patients with and those without compression fracture.

{kind=link}
Distribution and classification of vertebral fractures on spinal radiographs in the 11 patients with spinal compression fractures.
Factors associated with vertebral fractures in the 50 patients with juvenile idiopathic arthritis.
Factors found to be associated with compression fractures were further tested with logistic regression. Of the associated variables, cumulative weight-adjusted GC dose, CHAQ score, and BMI Z-score were chosen for further analysis in order to include 1 significant variable representing anthropometry, disease activity, and GC treatment (Table 4). None of the bone mass measures showed a p value < 0.1 and they were not included in the model (Table 4). Cumulative GC dose > 75 mg/kg (48% of the patients) was associated with a 7-fold increased risk (OR 7.2, 95% CI 1.37–38.0, p = 0.016), CHAQ > 0.5 (consistent with moderate disease activity; 22% of the patients) with a 7-fold risk (OR 7.2, 95% CI 1.58–32.9, p = 0.013), and BMI Z-score > +2.0 (28% of patients) with an almost 5-fold risk (OR 4.7, 95% CI 1.13–19.21, p = 0.052) for compression fractures. Cumulative GC dose was correlated with CHAQ score r = 0.29). In backward stepwise analysis the most significant associations with compression fractures were with CHAQ (OR 16.4, 95% CI 2.3–115.6, p = 0.005) and BMI Z-score (OR 1.89, 95% CI 1.07–3.36, p = 0.029), which together explained 45% of the fracture risk.
The visibility in the thoracic area was compromised in 7 patients and only part of the thoracic spine could be evaluated (that is, 2 to 11, on average 7, vertebrae). One of these patients had vertebral fractures in other spinal areas. When the 6 fracture-negative patients with incomplete spinal evaluations were excluded, the prevalence of vertebral fracture was 25%. The reported 22% prevalence of vertebral fracture in the whole cohort thus should be regarded as the minimum estimate for this high-risk patient population.
Fifteen patients (30%) had sustained a total of 24 significant low-energy long-bone fractures, excluding finger and toe fractures and refractures, at a median age of 9.6 years (range 0–15.4 yrs). Ten patients had sustained only 1 fracture, and the others 2–4 fractures, each after separate trauma. The patient with 4 fractures had fractured tibia, femur, calcaneus, and sacrum. Four patients were diagnosed with stress fractures and the other fractures resulted from low-energy trauma such as falling when walking or running; none were due to non-accidental injuries or to a primary skeletal disorder. Patients with and without peripheral fractures did not differ in duration or cumulative dose of GC, BMD values, age, height or BMI, disease duration, or disease activity measures.
Altogether 13 patients (26%) were considered to have significantly compromised bone health, as shown either by compression fractures (11 patients) or by low BMD (Z score ≤ −2.0 associated with a significant fracture history (as defined by International Society for Clinical Densitometry24; at least 2 long-bone fractures of upper extremities or 1 long-bone fracture of lower extremities) (2 patients).
DISCUSSION
Our study evaluated the prevalence and risk factors of vertebral compression fractures in a high-risk population comprising 50 patients (median age 14.8 yrs) with a history of treatment-resistant JIA. We found an alarmingly high number of children and adolescents (26%) with significantly compromised bone health — 22% (95% CI 10.28%–33.72%) of the study subjects had spinal compression fractures on radiographs. Other recent studies have also reported high prevalence of vertebral fractures among pediatric populations with various chronic illnesses1,2,3,4,6,7,8. Several possible risk factors for vertebral fractures have been suggested, but the findings in previous studies have been inconsistent.
Many studies evaluating vertebral fractures in children have been carried out in patient populations exposed to GC6,8,18. GC have deleterious effects on bone metabolism and Ca homeostasis29. GC increase the overall fracture risk in adults30 and in children31. Very little is known about prevalence of vertebral fractures in children and adolescents with JIA. Most of the cohorts studied have been heterogenous and also included patients with connective tissue diseases and vasculitis; our cross-sectional study, carried out in a single institution, included only subjects with JIA. In our selected cohort with severely affected patients, the prevalence was higher than in any previous study. Valta, et al6 found asymptomatic vertebral fractures in 10% of 62 patients with JIA treated with systemic GC for at least 3 months. Fractures did not correlate with weight-adjusted cumulative GC dose, disease characteristics, or aBMD. Nakhla, et al7 and Huber, et al8 studied vertebral fractures in children with chronic rheumatic diseases, including subjects with JIA, connective tissue diseases, and systemic vasculitis. Nakhla, et al found compression fractures in 19% of 90 patients; 10 (19%) of the 52 children with JIA had vertebral fractures, and half of those with fractures had systemic disease7. Risk factors for fractures included male sex and cumulative GC dose; disease activity and biochemical measures were not assessed. Huber, et al studied vertebral fractures within 30 days of start of GC therapy in 134 children8; fractures were diagnosed in 7%. Their cohort included 50 patients with JIA, of whom 2 with systemic arthritis had vertebral fractures. As shown by these studies and our observations, the prevalence of compression fractures in children with JIA is variable and dependent on cohort characteristics. Similar to our previous studies6,32, the total duration of GC exposure was not found to be associated with compression fractures, while recent GC exposure, calculated as the cumulative value for the preceding 3 years, was associated with compression fractures in logistic regression analysis.
In addition to GC, other factors also predispose to compression fractures, as fractures have been detected even in patients not exposed to steroids1,3,7. Chronic inflammation disturbs the balance between bone formation and bone resorption, triggering bone loss. Various cytokines, including TNF-α, interleukin 1 (IL-1), and IL-6, are likely to play a role in the process33. Our study population consisted of children and adolescents with severe and longlasting JIA; many were resistant even to multiple biologic therapies. An important observation in our study is that patients with spinal fractures had clearly more active disease, as indicated by higher CHAQ and disease assessment VAS scores and higher ESR, than those without fractures. It is difficult to separate the effects of inflammation and GC, as high doses of GC coincide with high disease activity during the early phase of the disease or during relapses. Similarly, high BMI may reflect high GC exposure and may not be an independent risk factor, although some studies suggest that overweight per se is a risk factor for compromised bone health34,35. Huber, et al8 found compression fractures in several patients with rheumatic disease within 30 days of the onset of GC treatment, providing further evidence for the significant role of the underlying inflammatory disease in the development of spinal fractures. In our study cohort, high CHAQ score, reflecting disease activity, and high BMI Z-score were even stronger predictors than recent GC exposure, and together explained 45% of the fracture risk.
In our cohort, patients with spinal fractures were older at the time of diagnosis of JIA (p = 0.029) and had shorter disease duration (p = 0.021) than those without spinal fractures, suggesting that the fractures are more likely to occur early in the disease process; consistent observations have been made in some other studies1,32. Although the data are very limited, there is evidence of remodeling capacity of vertebrae during childhood growth, especially when the underlying disease activity decreases. Varonos, et al18 showed improvement in vertebral morphology after changing patients from daily to alternate-day GC therapy. As the median disease duration in our study subjects was quite long (10.5 years), some previous fractures may already have healed. Longitudinal, longterm prospective studies are needed to elucidate the incidence and natural course of spinal fractures in JIA.
In general, fractures are common in children: up to one-half of children sustain fractures36,37,38; in contrast, vertebral compression fractures are very rare in healthy children4. In a large retrospective cohort study using the UK General Practice Research Database, the overall fracture risk in patients with childhood-onset arthritis was found to be higher than in controls15. In our cohort, 30% of participants had a history of peripheral fractures. Without a proper control group it is difficult to conclude whether this is consistent with increased bone fragility. Severely affected patients with JIA may have fewer opportunities for high-risk activities, and therefore actually have fewer fractures in spite of poorer bone health. In any case, patients with JIA seem to be particularly prone to vertebral fractures.
Several studies have shown low BMD in GC-treated and non-GC-treated patients with JIA10,11,12,13,14. The BMD values in our study subjects were surprisingly good, even after exclusion of patients with previous bisphosphonate treatment: the median Z- scores for the LS and WB aBMD were −0.8 and −1.0, respectively, and for the height-adjusted BMC/LTM ratio, +0.1. The aBMD values were not adjusted for height as this would have resulted in inappropriately good values in subjects with height loss due to compression fractures. However, it is possible that in some patients low BMD values were partly due to short stature. After height adjustment, the aBMD Z-scores would have been even better than when adjusted for bone age alone. Our results are thus in good agreement with previous studies showing that BMD is not a reliable tool in predicting the risk for spinal fractures1,6,39. In our study only 1 patient with compression fractures had an aBMD Z-score < −2.0. Data from studies on adults with a history of JIA have shown that persisting active disease is associated with an increased risk of osteopenia and osteoporosis, while attainment of normal BMD or bone mineral content is possible if remission is achieved40,41,42.
Our study has limitations inherent to the cross-sectional design, small cohort, absence of a control group, and the methodology used to assess BMD and spinal fractures. The subjects represented a selected patient population with severe JIA. Thus our findings cannot be extended to the general JIA patient population, but due to the relative homogeneity of the cohort, the results are valuable in elucidating the skeletal complications associated with severe JIA. The small cohort prevented more extensive statistical analysis to identify independent risk factors for compression fractures. DEXA analysis had limited value due to the high number of subjects with previous bisphosphonate treatment and presence of vertebral fractures in the LS BMD measurement area. Spinal fractures were diagnosed with radiography, which remains the “gold standard” for diagnostics. The visibility of vertebrae on radiographs may be compromised, especially in the thoracic spine; this was also true in some cases in our study. The true vertebral fracture prevalence may thus be even higher than reported here. In an extensive literature review we found no vertebral fracture grading systems that have been properly validated for pediatric use. With our study cohort, we felt that a classification adapted for a pediatric population1 was more appropriate than the more commonly used Genant method, which is based on adult data only43; the cutoff value for compressions, 20%, is similar in both methods. To avoid these limitations, future studies should use other methods such as peripheral quantitative computed tomography (pQCT), which may be more useful and accurate when evaluating bone mass44; however, pQCT measures peripheral skeleton and it is not known whether pQCT is superior to DEXA in predicting spinal fractures. More accurate spinal imaging methods may also be needed for vertebral fracture assessment.
We found a high prevalence of compression fractures in children with severe JIA. High disease activity and high BMI showed significant association with fractures. As vertebral fractures often are asymptomatic1,2,4,6,32,39 and not always associated with low BMD, they are probably underdiagnosed in children and adolescents with JIA. In adults, vertebral fractures predict subsequent vertebral fractures45. Whether this applies to childhood vertebral fractures remains unknown. Prospective longterm studies across the entire disease duration are needed to evaluate the incidence, disease- and lifestyle-related determinants, and natural course of vertebral fractures and their potential consequences for adult bone health. New treatment methods for JIA have improved possibilities to reduce disease activity and GC exposure and to achieve remission; future studies will show whether they prevent fractures and impaired bone health. Similar to adults46, guidelines are needed for the use of bisphosphonates in prophylaxis and treatment of vertebral fractures in children and adolescents with severe JIA.
Acknowledgment
Arja Nenonen and Heli Viljakainen are gratefully acknowledged for their assistance and expertise with laboratory evaluations and statistical analyses, respectively.
Footnotes
-
Supported by research funds from the Rheumatism Foundation Hospital and Helsinki University Hospital, the Foundation for Pediatric Research, the Academy of Finland, and the Sigrid Juselius Foundation.
- Accepted for publication September 15, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.