
Abstract
Objective. In pigmented villonodular synovitis (PVNS), some cases recur and progress to osteochondral destruction. The aim of our study was to clarify the occurrence of osteochondral destruction according to the location of PVNS during the clinical course.
Methods. Seventy-two patients with PVNS (43 female, 29 male) with a mean age of 40 years (range 3–87 yrs) had been referred to our institutions. Factors influencing the occurrence of osteochondral destruction were investigated.
Results. Mean followup was 60 months (range 12–190 mo). Adjacent bone change occurred in 24 (42%) of 57 patients, who were evaluated at the time of the first consultation. Eight (89%) of 9 patients with hip lesions initially had bone lesions, significantly more frequently than those with other lesions (p = 0.038). Duration of symptoms was significantly correlated with the occurrence of bone lesions in diffuse knee lesions (p = 0.005). During followup, patients with location in the knee had a significantly higher incidence of osteoarthritic change (73%) compared to those with foot and ankle involvement (p = 0.027). Re-operation was more frequently required for knee lesions due to the high recurrence rate (32%). Patients who required re-operation had significantly more marked osteoarthritic change in knees (p = 0.001) during followup than those who did not.
Conclusion. For PVNS arising in knees, repeated recurrences followed by re-operation resulted in the progression of osteoarthritic change. PVNS arising in hips, feet, and ankles developed bone lesions initially, probably due to the limited volume of these joints. The indications for re-operation for recurrent knee lesions require careful consideration regarding progression of osteoarthritic change.
- PIGMENTED VILLONODULAR SYNOVITIS
- OSTEOARTHRITIS
- BONE EROSION
- RECURRENCE
- SURGERY
Pigmented villonodular synovitis (PVNS) is a rare synovial proliferative disease that usually arises in the large joints such as the knee and hip1. The denotation PVNS was proposed by Jaffe, et al in 19411 and further subdivided as either diffuse or localized2. The pathogenesis had long been unclear, while recent findings that have demonstrated clonal chromosomal abnormalities suggest a neoplastic mechanism3. The estimated incidence of this disease is 1.8 per million per year4. PVNS often presents with diffuse articular involvement and induces a destructive change in juxtaarticular bone, especially of hips5,6,7 and foot and ankle8,9, although less marked destructive changes were observed in knee joints10. No reports have analyzed whether bone erosive change due to PVNS progresses or occurs as a new-onset condition during the followup period.
PVNS shows 2 distinct types: localized and diffuse. The optimal suggested surgical treatment for these subtypes is marginal excision for the localized type and total synovectomy for the diffuse type11,12,13,14. Extensive synovectomy alone is not feasible for cases with extensive bone destruction and degenerative change of articular cartilage7,13, arising in hips, shoulders, feet, or ankles, necessitating total joint replacement or arthrodesis in addition to total synovectomy in such cases. Although total joint replacement is a viable option for patients who have PVNS with extensive bone destruction, it is sometimes problematic. The age of patients with PVNS is lower than that of patients with degenerative joint disease such as osteoarthritis (OA), and these patients are more likely to require revision for the joint replacement due to aseptic loosening or recurrence of the disease, and sometimes even amputation15. Prevention of not only recurrence but also osteochondral destruction should be the aim of treatment of patients with PVNS.
Surgeons treating patients with PVNS usually pay particular attention to surgical technique, adjuvant therapy, minimal invasiveness, and rate of recurrence according to the technique chosen. Patients, though, are especially concerned about the possibility of joint destruction during the course of the disease. Surgeons should provide information to patients concerning the incidence of bone destruction and cartilage degeneration, one of the most significant complications of this disease. The aim of our study was to analyze the occurrence of osteochondral destruction of the involved joints by PVNS at the initial visit and during the followup. Possible factors associated with the occurrence of osteochondral destruction were analyzed.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the medical records of 92 consecutive PVNS cases initially diagnosed in our institutions between 1987 and 2008. Twenty cases were excluded; 5 had been correctly diagnosed with proliferative synovitis after hemorrhage or synovial hemangiomas, and 10 arising in or along the tendon sheath of the wrist or ankle joints were considered as having giant cell tumor of the tendon sheath. Two had PVNS in soft tissue locations. Three had been followed for less than a year. Finally, the study was composed of 72 consecutive patients with 58 diffuse and 14 localized PVNS treated at our 4 institutions.
Followup data were obtained for all patients with a clinical, radiological, and histological evaluation at our institutions. All 72 cases were histologically reevaluated as PVNS. These data were recorded: age, sex, involved joints, time from onset of symptoms to presentation to the initial physician, existence of hemoarthrosis, previous surgical treatment, adjacent bone destruction at the time of referral to our institutions, methodology of treatment, recurrence after surgical treatment at our institutions, re-operation after relapse, and progression of osteochondral destruction.
Forty-three patients were female and 29 were male. The knee joints were affected in 35 patients, foot and ankle joints in 19, hip in 9, wrist and carpal joint in 4, elbow in 3, and shoulder in 2. Fifty-eight patients had diffuse and 14 had localized disease (Table 1). Sixty-two patients were referred to our institutions without previous treatment and 10 were referred due to recurrence after surgery elsewhere. Preoperatively, all patients with hip lesions (n = 9) had symptoms of pain and/or diminished range of motion, and 18 (34%) and 12 (34%) patients with knee lesions had symptoms of joint swelling and pain, respectively. These symptoms affected the patients’ activities of daily living to some extent. Sixty-six patients had surgical treatment in our institutions, and 6 were conservatively followed up radiologically. The time from onset of the initial symptoms to the first referral to physicians ranged from 1 week to 15 years (mean 2.9 yrs). Age at the time of presentation ranged from 3 to 76 years (mean 40 yrs). No patient had a family history of PVNS. The length of the followup period in patients with surgical treatments was calculated from the date of surgery or the date of first visit (patients without surgery) until the date of the last examination. Mean length of followup was 60 months (range 12–190 mo).
Demographic details of the 72 patients.
Radiological examination
All patients were examined with plain anteroposterior and lateral radiographs, magnetic resonance imaging (MRI), and/or computed tomography (CT) of affected joints at the time of the initial referral. In particular, MRI was used to confirm the extent of infiltration by PVNS for determination of adequate surgical treatment. Radiographs and/or CT images were reviewed independently by 2 orthopedic surgeons for the evaluation of osteoarthritic change and bone destruction. Presence of bone lesions was assessed with plain radiographs and/or CT images, and lesions > 5 mm in diameter were evaluated as positive. Osteoarthritic change of the involved joint was graded using the Kellgren-Lawrence (K–L) scale, a 5-level OA severity score (0 indicating normal; 1 doubtful; 2 mild or minimal; 3 moderate; and 4 severe) based on a pictorial guide16 depicting the degree of osteophyte formation, joint space narrowing, sclerosis, and joint deformity. Osteoarthritic change was defined as being present with a score ≥ 2. Cases with OA with a score of 3 or 4 at the initial referral were excluded from the OA progression analyses. Progression of osteoarthritic change was defined as an increase in the K–L grade. For evaluation of osteochondral destruction, intra- and interobserver variability was calculated.
Treatment modalities
Six patients were followed up only conservatively due to their young age or rejection of surgical treatment. Two of them had a history of treatment at the prereferral hospital. Localized type of PVNS was simply resected en bloc. Of 27 patients with diffuse knee lesions, 23 were treated surgically; 16 were treated with both anterior and posterior total synovectomies, and 4 with anterior and 1 with a posterior approach alone based on the location of the diffuse PVNS. Prosthetic replacements after total synovectomies were performed for 2 patients with knee lesions who had grade 3 OA according to the K–L classification. Of 17 foot and ankle cases, 15 cases were treated with surgery, total synovectomy in 8, and total synovectomy followed by arthrodesis of talocrural or subtalar joints in 7. Eight of 9 patients with hip lesions were treated with a total synovectomy through a lateral approach under a great trochanteric osteotomy in 7 and the anterior approach in 1 patient. One patient required total hip replacement following total synovectomy. Resected specimens were examined routinely for pathology. None of the patients were treated with adjuvant therapy, such as radiation or chemotherapy. Postoperatively, 3 (33%) of 9 patients with hip lesions still complained of pain in the affected joints, and 7 (20%) of 35 patients with knee lesions had a diminished range of motion that interfered with activities of daily living. Recurrence was evaluated by MRI every 4–6 months postoperatively. Plain radiographs were available to evaluate OA progression and/or bone destruction.
Statistical analysis
We determined differences in non-normally distributed data (age, time from onset of symptoms to presentation to the initial physicians) between the bone destruction (+) group and (–) group or the osteoarthritic change (+) group and (–) group using the Mann-Whitney U test. We determined differences in the proportion of occurrences of osteochondral destruction between the groups (sex, involved joints, hemoarthrosis) using the chi-square or Fisher probability test. P values < 0.05 were considered statistically significant. All analyses were performed using SPSS 17.0 for Windows software (SPSS Inc., Chicago, IL, USA).
RESULTS
Bone destruction at the first visit to our institutions could be evaluated in 57 of 72 patients with plain radiographs (Table 1). Of evaluable patients, 24 (42%) had bone lesions (Figure 1). Of 29 patients with knee lesions evaluated, 6 had bone lesions (21%). Eight (89%) of 9 patients with hip lesions, and 7 (58%) of 12 with foot and ankle lesions had bone lesions. Of 8 patients with localized knee lesions, none had bone lesions. There was 8% and 0% of interobserver variability in detecting OA progression and bone destruction, respectively. No intraobserver difference was observed. Statistical analysis of all cases revealed that location of the disease was significantly associated with the occurrence of bone lesions (p = 0.001). Duration of symptoms was a significant factor associated with bone lesions (p < 0.001). Of patients with diffuse knee lesions, those with bone lesions had a significantly longer duration of symptoms (6.4 ± 5.1 yrs) than those without them (1.4 ± 1.3 yrs; p = 0.005). Of patients with foot and ankle lesions, there was no significant difference in the duration of symptoms between patients with bone lesions (4.3 ± 2.9 yrs) and those without them (4.0 ± 4.2 yrs; p =0.93). Of 35 patients with knee lesions, 16 (46%) had a history of hemoarthrosis, which was not associated with the presence of osteochondral destruction at the time of the first referral (p = 1). As expected, patients with diffuse lesions had a significantly higher rate of bone lesions as compared with those with localized lesions (p = 0.002). Other clinical variables had no significant influence on the initial appearance of bone lesions (Table 2).
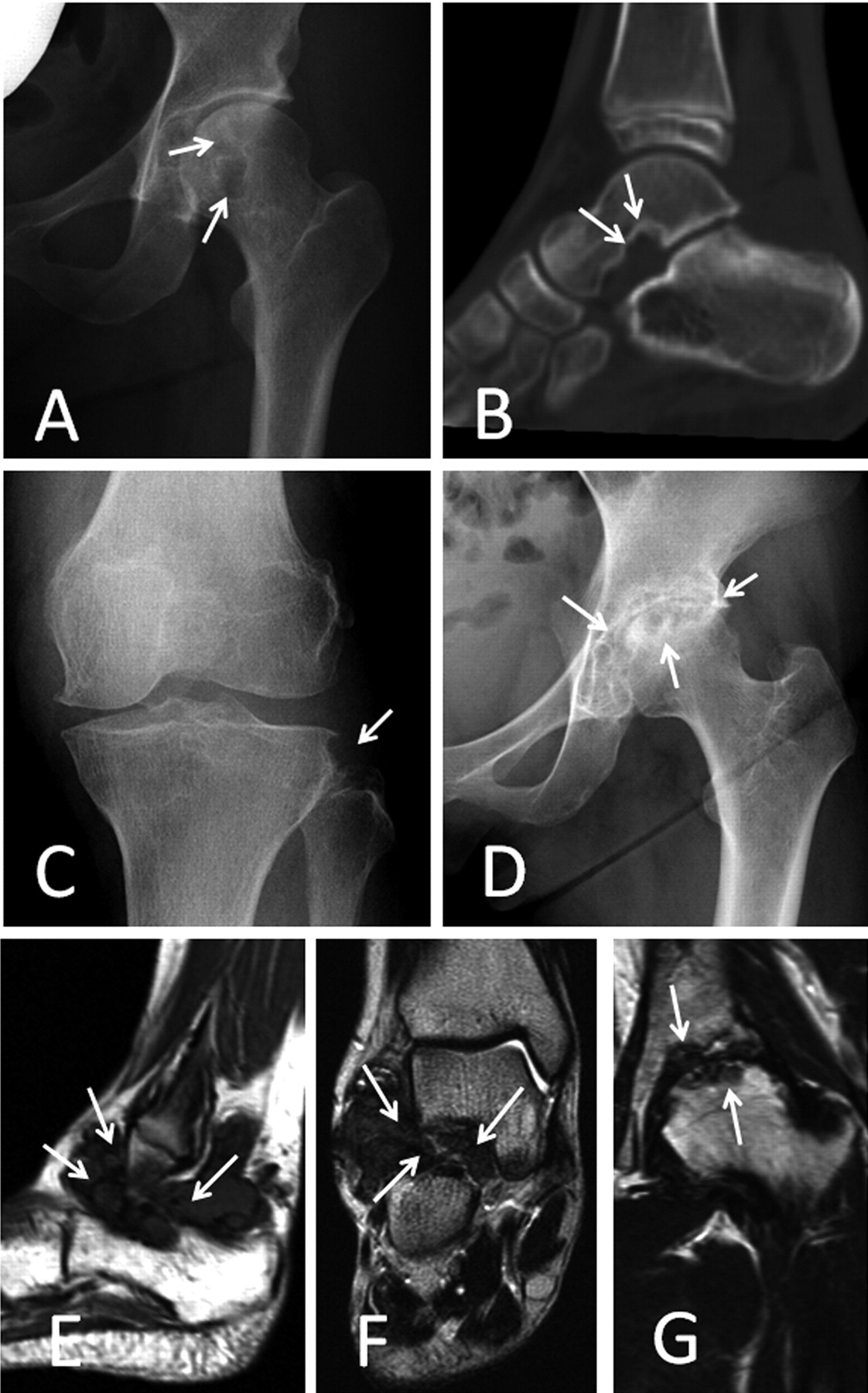
Bone lesions at the time of the first visit. A. Woman age 29 years; radiograph shows cystic bone erosion of the left femoral head and neck (arrows). B. Girl age 8 years; sagittal CT image shows bone erosion with marginal sclerosis of the right talus (arrows) in talo-calcaneal joint. C. Woman age 61 years; radiograph shows bone erosion of the left lateral tibial condyle (arrow). D. Woman age 37 years; radiograph shows advanced destructive osteoarthritic change of left hip joint (arrows). E and F. Same case as shown in panel B. Both sagittal T1-weighted and coronal T2-weighted MR images show PVNS tissues that invade talo-calcaneal joint (arrows). G. Same case as shown in panel D. Coronal T2-weighted MR image shows PVNS that invades both acetabulum and femoral head (arrows).
Factors influencing bone destruction at first visit.
Of 66 patients who received surgical treatment in our institutions, tumors recurred in 14 (21%). Of 31 patients with operated knee lesions, 10 (32%) showed recurrence. Focusing on the diffuse type, 10 (43%) had recurrence of knee lesions. There was no significant difference in recurrence between patients with the anterior/posterior surgical approach and those with only the anterior approach (p = 0.58). Three (20%) of 15 patients with foot or ankle lesions experienced recurrence, and no significant difference in the recurrence rate was observed between patients with and those without arthrodesis (p = 1). On the other hand, no patient with hip lesions had recurrent lesions. Concerning the location, although a higher recurrence rate was observed in patients with knee lesions, there was no significant difference (p = 0.13). There was no relationship observed between histopathological features of PVNS and disease recurrence or progression.
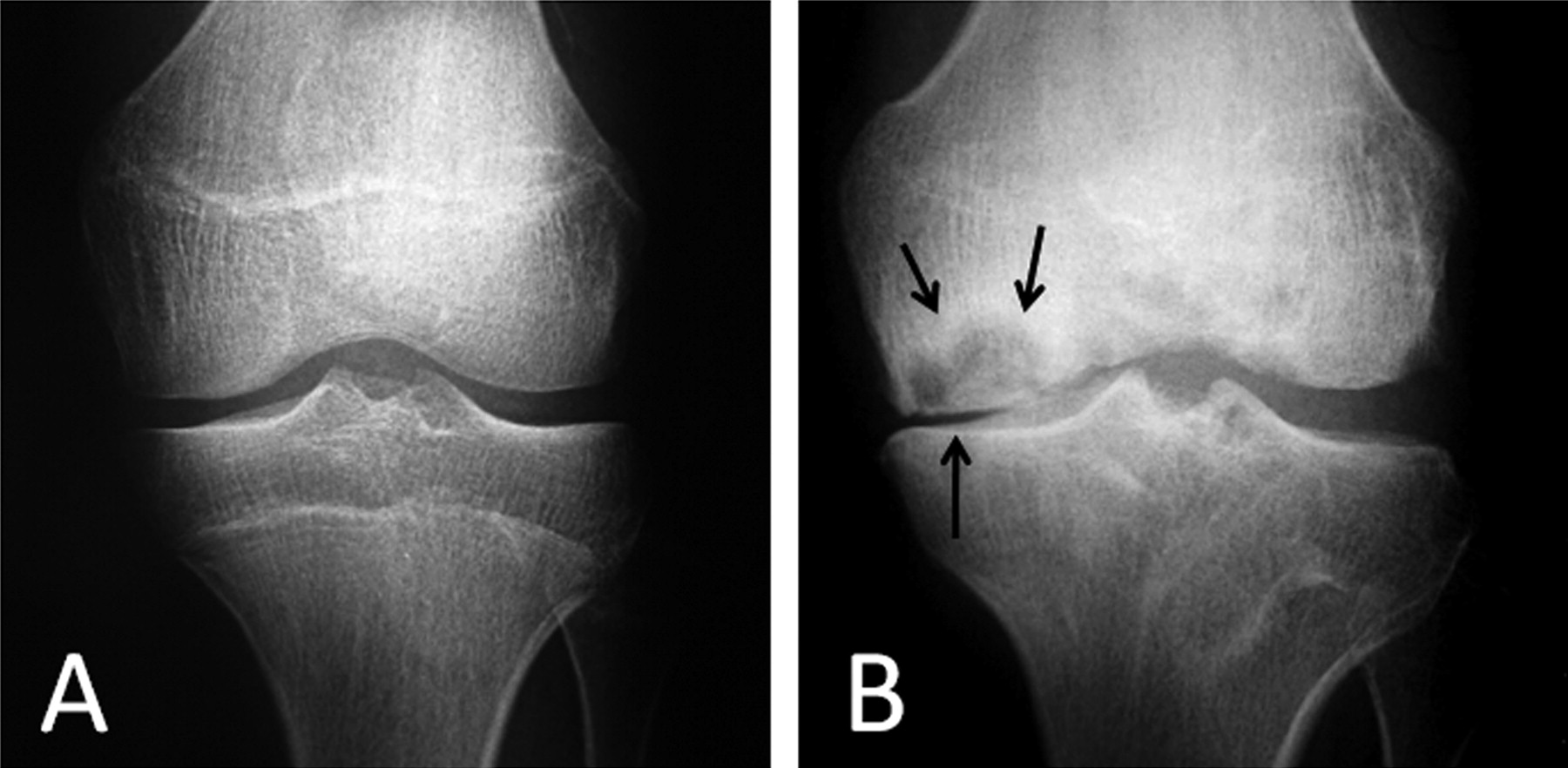
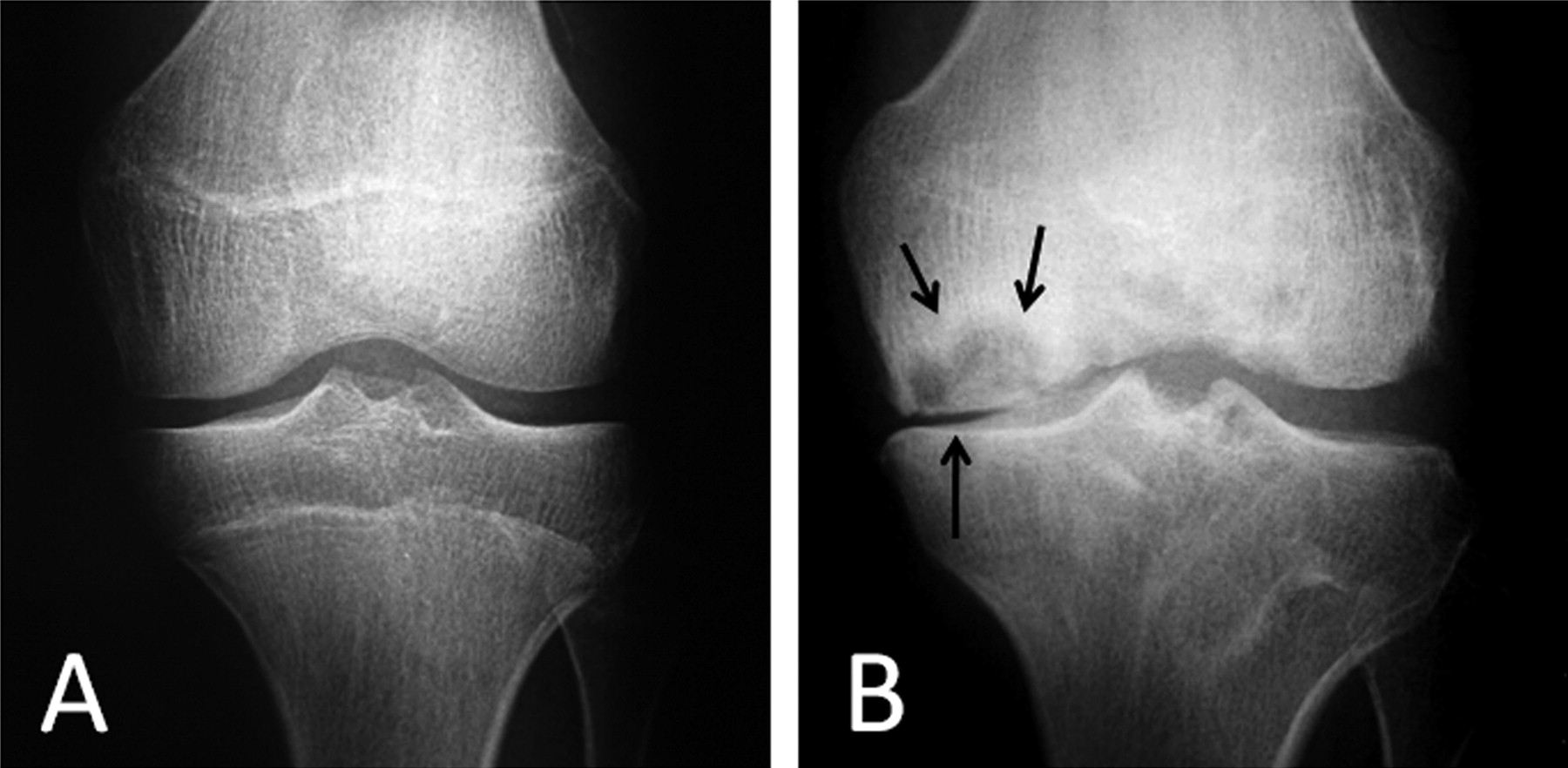
Progression of OA and bone destruction during followup was evaluated in 57 and 58 patients, respectively, after exclusion of patients with total hip arthroplasty, total knee arthroplasty, arthrodesis of foot or ankle, osteochondral destruction at the time of the first visit, and with unknown data (Table 3). Nineteen patients (26%) had progression of OA (Figure 2) and 14 (19%) had progression of bone destruction. Of 18 patients with evaluated diffuse knee PVNS, 13 (73%) had progression of OA and 10 (56%) had bone destruction. Among 6 patients with evaluated hip lesions, 2 (33%) had progression of OA and 1 (17%) had bone destruction. Among 11 patients with evaluated foot or ankle lesions, 3 (27%) had progression of OA and 3 (27%) had bone destruction. Patients with diffuse knee PVNS had a significantly higher rate of OA progression (p = 0.027) compared to those with foot and ankle locations. In contrast, no significant difference was observed in bone destruction (p = 0.14). Given that patients with diffuse knee lesions had a higher recurrence rate (43%), re-operation for the recurrent lesions was analyzed as a possible factor associated with OA and bone destruction. Re-operation for recurrence was a significantly poor prognostic factor in the progression of osteoarthritic change (p = 0.001). Although recurrence was a poor prognostic factor for OA progression (p = 0.005), it had a less significant influence compared with re-operation (Table 4). Interestingly, of 8 patients surgically treated at the prereferral hospital, 6 (75%) had OA progression and 3 (38%) had progression of bone destruction. There were no factors significantly associated with progression of bone destruction.
{kind=link}
{kind=link}
Recurrence followed by re-operation resulted in osteoarthritic change. A. Young man age 16 years; radiograph showing no osteoarthritic change when he underwent total synovectomy with the anterior approach. B. Four years after initial operation. During this period, PVNS recurred twice, followed by open synovectomy each time. Remarkable osteoarthritic change (arrows) was observed on radiography.
Osteochondral destruction during followup.
Variables associated with progression of osteochondral destruction during followup in knee joints.
DISCUSSION
Several previous studies described the bone lesions in PVNS. Ottaviani, et al17 noted that in previous studies, bone lesions were reported in 3% to 87%4,5,13,14,18,19,20,21,22, and occurred most frequently in the hip in their study (66%) and 1 other trial (87%)5. A larger articular cavity in the knee could in part explain the lower rate of bone lesions in that joint. Indeed, the ratio of intraarticular pressure/articular volume is low for the knee joint (222 mm Hg for a mean volume of 104 ml)23,24, intermediate for the ankle joint (142 mm Hg for a mean volume of 20.9 ml)25, and high for the hip (200 mm Hg for a mean volume of 12 ml)26. In our current study, the rate of bone lesions at the initial visit was consistent with this concept: 21% for knees, 89% for hips, and 58% for ankles. Considering that the incidence of PVNS is very low and the symptoms are not severe, this disease cannot be detected in advance of formation of bone lesions. On another clinical point, physicians should become aware of the disease when bone lesions are observed in patients with mild symptoms, particularly of hips and feet and ankles.
Dorwart, et al27 reported that bone changes begin with erosion of the articular cartilage, often near the chondro-osseous junction, with subsequent extension of the process through the cartilage and the underlying cortical bone into the cancellous bone. This gives rise to the juxtaarticular cysts evident radiographically, which are surrounded by fibrous tissue. In that review27, 146 joints showed PVNS involvement, and 74 (51%) showed bone changes. Of 81 knees, 21 (26%) had cystic bone lesions. Of 40 hips, 37 (93%) had bone lesions, in agreement with our results. Ankle and foot case studies have found that the percentages of bone lesions were similar to those noted in our study (i.e., 58%): from 67% to 87.5%8,9,27.
In this manner, osseous erosion in PVNS is commonly observed in joints in which the synovia cannot expand due to the presence of a tight capsule and firm ligament. This may induce an increase in the intraarticular pressure, resulting in invasion by the synovial fluid and synovial proliferative tissues into the bone through the vascular foramina28. Considering that hips, in which bone destruction is often observed, have a wide range of multidirectional motion, extensive articulation might promote invasion of synovial tissues into the adjacent bone. Long duration from the onset of symptoms to diagnosis will allow pigmented villonodular synovial tissues more opportunity to invade the bone, as confirmed statistically by the results in our study.
Surgery is the most common treatment for PVNS. Concerning the various forms, total synovectomy is classically proposed29,30. The main principle of surgical treatment was to resect all the diseased tissue with normal synovial tissues including joint capsule on inspection using open techniques involving the anterior, posterior, or both compartments. The localized disease type was treated by marginal resection. Arthroscopy is preferred, when possible, in the localized form and appears to give results similar to open surgery in this situation, with less morbidity29,30,31,32. Considering that the final goal of the surgical treatment for PVNS should be to maintain the function of the involved joint, and the benign experience of this disease, surgery-related morbidity should be avoided.
Several longterm followup studies have evaluated the clinical outcome of PVNS including recurrence rate in different locations and types of PVNS4,14,18. Despite its benign histological appearance, PVNS has a high but variable recurrence rate of 8% to 60%10,11,18,22,29,30,31,32,33,34,35. Previous reports suggest different factors responsible for recurrence, the most important of which include a history of previous surgery for PVNS of that joint, diffuse type of disease, large joints, and adequacy of the synovectomy. These factors were in agreement with the results of our study, in which a high recurrence rate was observed in knee lesions and diffuse type disease. A question arises whether reexcision for the recurrent lesion is absolutely required. Sharma and Cheng36 reported that reexcision can salvage relapses; however, higher surgical morbidity may be associated with another operation. Recent imaging modalities have improved the detection capabilities for recurrent lesions. Chin, et al10 reported that MRI has been shown to be effective for detection of diffuse PVNS tissue preoperatively and for monitoring patients postoperatively37,38,39,40,41. In their series, MRI appeared to be highly sensitive but less specific for detecting residual PVNS postoperatively because of the confounding presence of surgery-induced changes within the knee. The benefits of MRI are highlighted by the fact that 3 of their 7 recurrent cases were asymptomatic and would not have been detected otherwise. Reports that document recurrences solely on the basis of clinical and radiographic followup are therefore likely to underestimate the number of recurrences11,30,32. However, we again raise the question of whether recurrent lesions need to be detected by novel imaging modalities followed by reexcision, particularly in cases without symptoms.
Although a role for PVNS in the development of bone destruction at the initial visit has been reported4,5,13,14,17,18,19,20,21,22,42, no studies have revealed the occurrence of osteoarthritic change and progression of bone destruction during followup of PVNS. Given that the purpose of re-operation for recurrent lesions should be the maintenance of joint function, clarification of the factors influencing osteochondral destruction during followup is most important in deciding the treatment modality. Our study revealed for the first time that re-operation for recurrent lesions is a significant adverse factor associated with deterioration of osteochondral lesions. Knee joints, which have a large articular volume, have fewer bone lesions compared with other joints with smaller volume. Moreover, degrading enzymes for articular cartilage are expressed less in joints of PVNS than those in rheumatoid arthritis43. Accordingly, the indications for aggressive re-operation for recurrent knee lesions should be applied with particular caution, because the treatment itself may impair the function of the involved joint.
Our study has several limitations. In the past, re-operations in our institutions for recurrent lesions of the knee were most commonly open total synovectomies, an invasive surgery causing more osteoarthritic change than arthroscopic synovectomy. Arthroscopic operation should be attempted for recurrent lesions, as for primary lesions, to mitigate osteoarthritic change. The second limitation is the lack of data for adjuvant therapy. External radiotherapy44,45,46,47 and isotopic synoviorthesis have been reported10,35. The use of more extensile approaches and adjuvant radiotherapy (external beam or intraarticular radiocolloid injection) reportedly improves local control10,48,49, which may affect the osteoarthritic change and bone destruction during followup. However, while there is little doubt that radiation may be effective for small lesions in the foot50, less success has been achieved in restoring function in patients with knee or especially hip disease47. These adjuvant therapies may adversely affect joint degradation. The third limitation is the small number of cases evaluated; given the rarity of this disease, multicenter longterm followup studies will be required to confirm these results.
PVNS with lesions of hips, feet, and ankles frequently develops bone lesions initially, probably due to the limited volume of these joints. Physicians should be aware of the possibility of this disease in patients with bone lesions who have mild and prolonged symptoms in affected joints. For PVNS arising in knees, repeated recurrences followed by re-operation resulted in progression of the osteoarthritic change. Indications for re-operation for recurrent lesions of the knees require careful consideration regarding the progression of osteoarthritic change.
Acknowledgment
We thank Eri Ishihara for secretarial assistance.
Footnotes
-
Supported in part by the Ministry of Education, Culture, Sports, Science and Technology of Japan, Grant-in-Aid 20591751 for Scientific Research ©.
- Accepted for publication September 29, 2011.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.