
Systemic symptoms such as organomegaly and endocrine manifestations, in the presence of a peripheral neuropathy, may alert the clinician to POEMS syndrome (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes).
A 30-year-old man was admitted for the recent onset of a demyelinating polyneuropathy. Clinical and laboratory investigations disclosed lower limb edema, hepatosplenomegaly and lymphadenopathy, gynecomastia associated with hyperprolactinemia, hypothyroidism, adrenal and gonadotropic insufficiencies, and bilateral papilledema. Monoclonal gammopathy IgA λ was present. POEMS syndrome was suspected. Serum vascular endothelial growth factor (VEGF) level was 953 pg/ml (normal < 115). Pelvis radiography (Figure 1) showed an expansile osteolytic lesion mainly in the left iliopubic ramus, contrasting with preserved or thickened cortical margins and thick sclerotic intralesional walls. Three other small lytic lesions with a sclerotic rim were observed. Biopsy of the largest bone lesion showed a massive infiltration by atypical plasma cells (Figure 2), which were clonal lambda on immunostaining (Figure 3). POEMS was confirmed and, because there were > 2 bone lesions, chemotherapy was started, as well as cementoplasty of the large osteolytic lesion1,2.

Osteolytic lesion in the left iliopubic ramus with marked thick sclerotic walls.
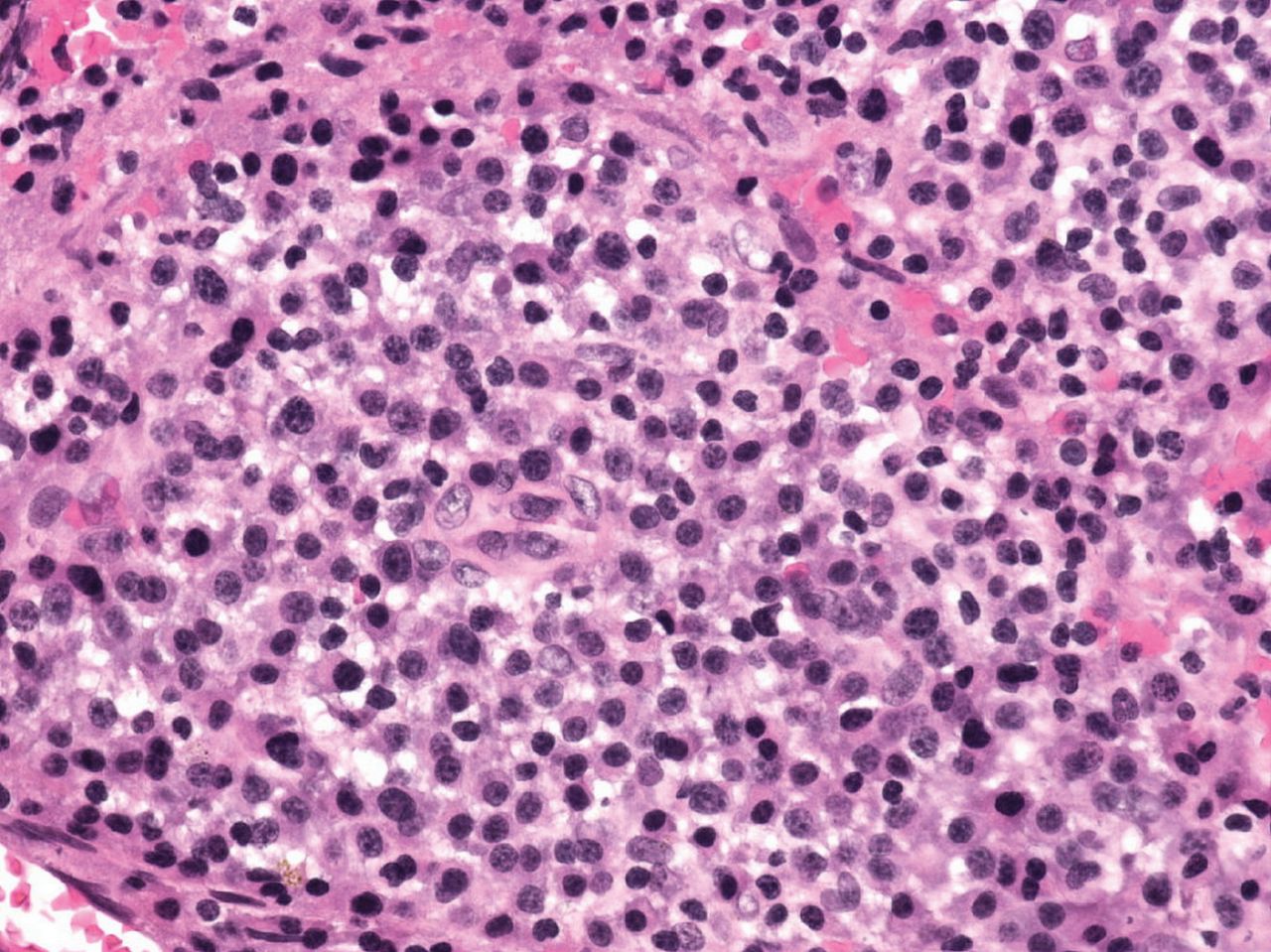
Biopsy showed a massive infiltration by atypical plasma cells (original magnification ×400).

{kind=link}
{kind=link}
{kind=link}
Plasma cells showed clonal lambda on immunostaining (original magnification ×400).
In the presence of a peripheral neuropathy, systemic symptoms such as organomegaly and endocrine manifestations should suggest POEMS syndrome3 and lead to bone radiograph, VEGF serum level measurement, and a search for monoclonal gammopathy.
REFERENCES
- 1.
- 2.
- 3.