
Abstract
Objective. Psoriatic arthritis (PsA) is characterized by varied radiographic features. We describe a patient with PsA with severe radiographic damage that improved significantly following treatment with etanercept. The improvement was documented by several methods of radiographic assessment.
Methods. Etanercept was introduced in September 2005. Radiographs of the hands and feet were read using 3 methods: the modified Steinbrocker method, the van der Heijde (vdH) modification of the Sharp method, and the Ratingen scoring system.
Results. In July 2009, radiographs of the hands and feet showed improvement in erosion score and joint space narrowing, while bony proliferation remained the same [43 by modified Steinbrocker, 26 by the vdH Sharp score (12 for erosions and 14 for joint space narrowing), and 56 by the Ratingen (18 for erosion and 38 for proliferation].
Conclusion. The 3 radiographic methods were useful in demonstrating improvement in joint scores. The modified Steinbrocker method, which is the simplest, was able to reveal improvement in our patient.
- PSORIATIC ARTHRITIS
- REPAIR
- RADIOGRAPHY
- ANTI-TUMOR NECROSIS FACTOR AGENTS
Psoriatic arthritis (PsA) is characterized by varied radiographic features including bone resorption in the form of large eccentric erosions and pencil-in-cup changes along with features of bone formation such as periostitis and ankylosis1. Until recently these changes were considered irreversible. We describe a patient with PsA with severe radiographic damage that has improved significantly following treatment with etanercept. We demonstrate that the improvement could be documented by several methods of radiographic assessment.
A 49-year-old woman with psoriasis since the age of 25 years developed pain and swelling in her fingers, wrists, and ankles and was diagnosed with PsA at age 42 years. Prior to her first visit to the PsA Clinic in 1996, she had been treated with and failed several nonsteroidal antiinflammatory medications as well as intramuscular gold and oral methotrexate (MTX) 15 mg per week. At her first visit to our PsA Clinic she was noted to have asymmetric polyarthritis with dactylitis and 2 clinically damaged joints. Radiographs demonstrated erosions in 7 joints, fluffy periostitis, and bilateral grade 1 sacroiliitis. The diagnosis of PsA was confirmed and the dose of MTX was increased, first orally and later by subcutaneous injections, to a maximal dose of 25 mg per week. Despite this she continued to have active polyarthritis and accumulated joint damage. Followup was irregular as she lived at a distance from the Clinic. In May 2005 she was found to have 21 actively inflamed joints, 10 of which were swollen; she also had 11 clinically damaged joints with 7 flail joints. She had accumulated extensive radiographic joint damage, with fluffy periostitis and numerous erosive changes, mainly in the fingers and toes, including some joints with a total destruction in the form of pencil-in-cup change (Figure 1). Erythrocyte sedimentation rate (ESR) at that time was high at 72 mm/h.

2005: Severe radiographic joint damage prior to starting anti-TNF therapy; large erosions, pencil-in-cup deformity, and periostitis.
MATERIALS AND METHODS
Etanercept was introduced in September 2005 by subcutaneous injections at a dose of 25 mg twice a week. Within several weeks of initiation of etanercept therapy, there was marked improvement in the peripheral joints symptomatically, and on physical examination there were no signs of active arthritis. ESR decreased to normal levels. She was able to stop treatment with MTX.
RESULTS
Radiographic damage scores are presented in Table 1. Plain radiographs of the hands and feet from May 2005 (Figure 1) scored 61 on the modified Steinbrocker, 59 by the vdH Sharp score (36 for erosions and 23 for joint space narrowing), and 86 by the Ratingen system (45 for erosion and 41 for proliferation). Radiographs from 2007 (Figure 2) showed marked improvement in erosion and proliferation scoring, with scores of 58 by the modified Steinbrocker, 38 by vdH Sharp score (16 for erosions and 22 for joint space narrowing), and 63 by the Ratingen (26 for erosion and 37 for proliferation). The patient remained in remission without any significant change in physical examination findings at her next visit to the clinic in July 2009. At that visit, radiographs of the hands and feet (Figure 3) showed additional improvement in erosion score and joint space narrowing, while bony proliferation remained the same [43 by modified Steinbrocker, 26 by the vdH Sharp score (12 for erosions and 14 for joint space narrowing), and 56 by the Ratingen (18 for erosion and 38 for proliferation)].

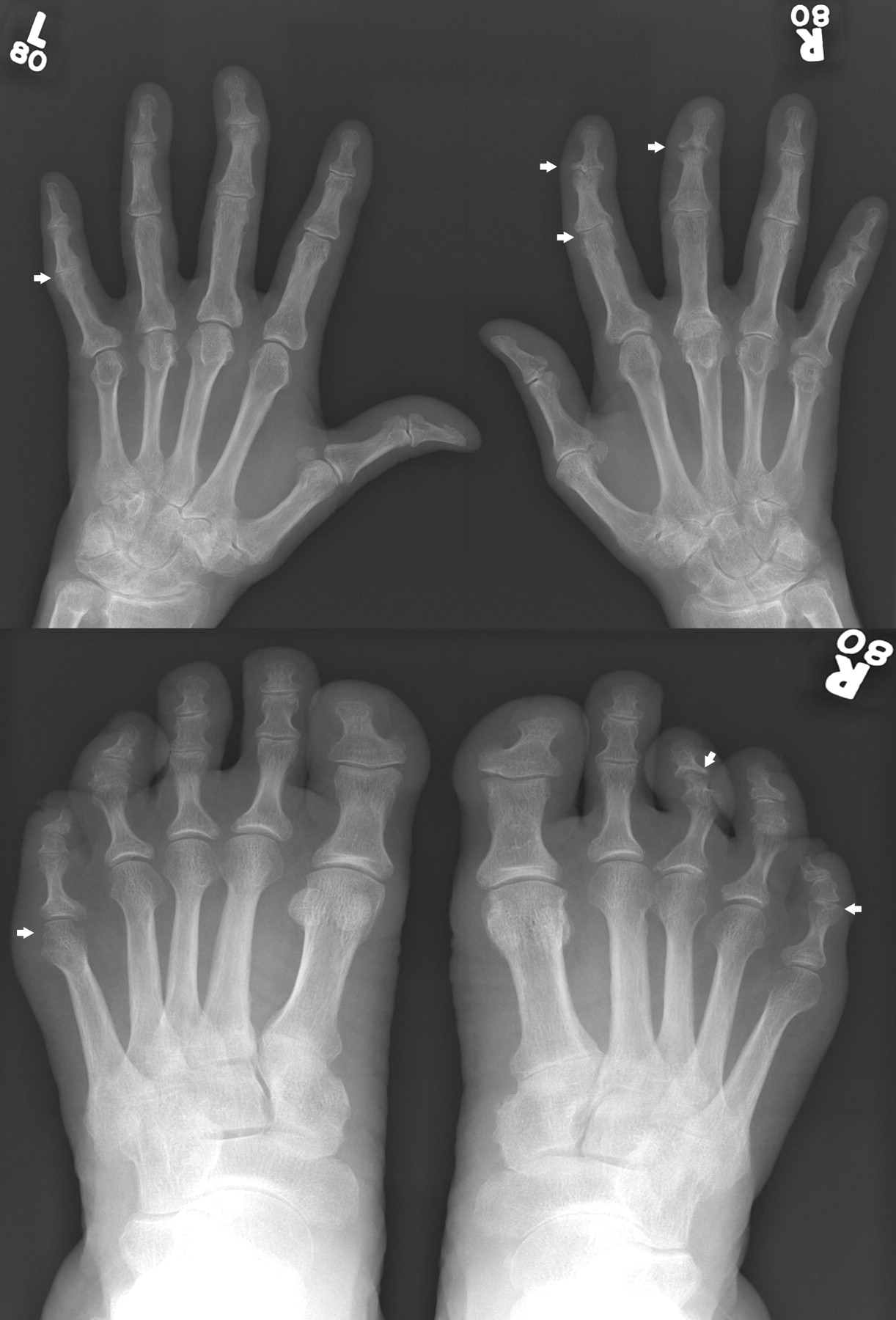
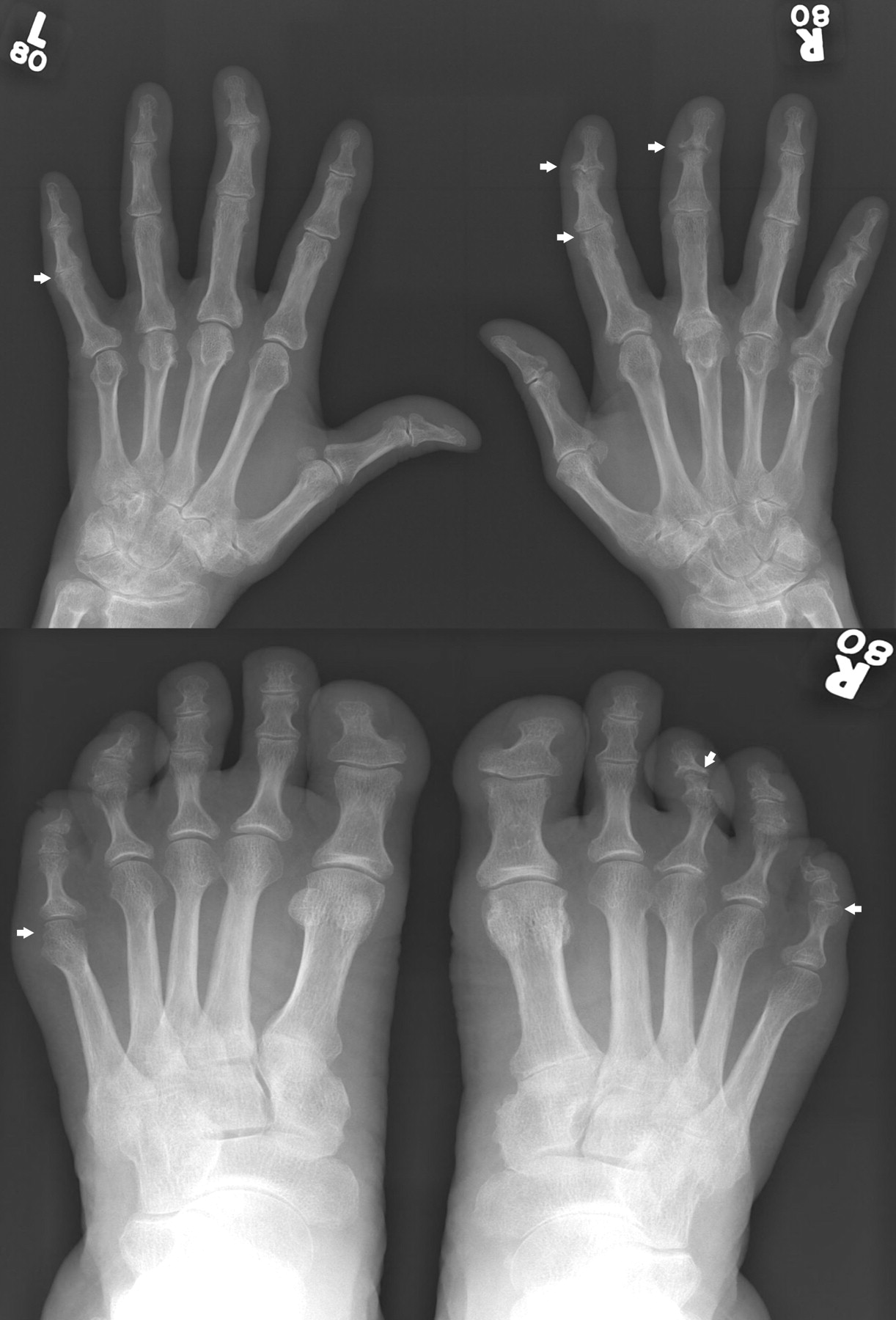
2007: Improvement in radiographic joint damage following 2 years of etanercept therapy is observed in the right hand, second and third distal interphalangeal (DIP) and proximal interphalangeal (PIP) joints; and in the left foot, fifth metatarsophalangeal (MTP) and PIP joints, and right foot, third DIP joint.
{kind=link}
{kind=link}
{kind=link}
2009: Additional radiographic improvement after 4 years of etanercept therapy. Further improvement in joint damage is observed in the right hand second DIP, which now looks almost normal, the third DIP, which seems to have developed cartilage space, and PIP joints, which no longer demonstrate erosions; and in the left foot, fifth MTP and PIP joints, which seem to have normalized, and right foot, third DIP joint, where the erosions have resolved.
Regression of radiographic joint damage following anti-tumor necrosis factor treatment.
DISCUSSION
PsA is characterized by inflammatory arthritis that often leads to significant structural damage. The radiographic features in PsA can be grouped into destructive and proliferative changes. Erosions are a typical destructive feature; they occur in up to 67% of patients at their first visit to the clinic5, and in 27% of patients within 5 months of onset of arthritis6. Widespread erosive changes can lead to the characteristic pencil-in-cup change. New bone formation is another typical feature of PsA, which may present as either periosteal reaction or ankylosis. Fluffy periostitis is included in the CASPAR criteria for classification of PsA7. These 2 seemingly opposing mechanisms, marked erosion and bone formation, can occur in the same patient and may present in different joints in the same finger.
Until the introduction of effective targeted therapy, particularly the anti-tumor necrosis factor (anti-TNF) agents, bone damage was considered irreversible. The concept of damage repair was introduced by the negative radiographic progression scores that were found in several clinical trials of anti-TNF agents8,9. This concept was supported by findings in several OMERACT studies10,11, as well as in cohort studies in rheumatoid arthritis (RA)12,13, suggesting that joint repair can occur. Thus, the concept of radiographic repair of joint damage following anti-TNF treatment is now being accepted as a real phenomenon.
In RA the prevalence of decreases in erosion scores following treatment with anti-TNF agents was reported to range from 7.2% to 10.7%11,12. Repair occurred particularly in clinically inactive joints and in patients with more severe joint damage. The studies have also showed that the repair process is localized, as some joints showed repair, whereas in others there was progression of damage.
In PsA, there is less information about damage repair; however, clinical trials with anti-TNF agents have shown that regression of joint scores does occur in a subset of the patients treated with these agents. A subanalysis of radiographic scores of the ADEPT trial, comparing adalimumab to placebo treatment, showed improvement in modified total Sharp score14. This change was most prominent among the patients treated with adalimumab, particularly among those with an elevated baseline C-reactive protein (CRP). Cumulative probability plots have shown that up to 10% of the patients with low CRP and approximately 20% of those with elevated CRP had improvement in the radiographic score after 24 weeks of treatment. Similar results were seen in subanalysis of changes in the modified total Sharp score study of etanercept15. Higher proportions of patients in the etanercept group had negative change in scores from baseline compared with the control group. The changes primarily reflected changes in the erosion score and not the joint space narrowing score.
Our patient, who had sustained severe radiographic joint damage, demonstrated a significant repair of the damage including refilling of bone erosions, resolution of periostitis, and reforming of almost intact joint structure, following treatment with an anti-TNF agent. This case emphasizes that resolution of severe radiographic damage can occur after effective treatment. It also highlights that the repair process may take several years. We note the utility of the radiographic methods in demonstrating improvement in joint scores. In particular, the modified Steinbrocker method, which is the simplest and is easier and less time-consuming, was able to reveal improvement that was documented in our patient. Further studies are needed to investigate the prevalence of this process among patients using anti-TNF agents and to determine the mechanisms that are involved.
Footnotes
-
Dr. Eder is supported by an Abbott Psoriatic Arthritis Fellowship and a Canadian Arthritis Network Fellowship; Dr. Chandran is supported by a Canadian Institutes for Health Research Clinical Research Initiative Fellowship. The Psoriatic Arthritis Program is supported by the Krembil Foundation and the Arthritis Society by a SPARCC/NRI grant.
- Accepted for publication December 3, 2010.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.