
To the Editor:
We describe a 54-year-old woman with systemic sclerosis (scleroderma, SSc) of the limited subtype. Diagnosis in 1994 was based on tightness of the skin distal to the metacarpophalangeal joints, calcinosis, telangiectasia, esophageal dysmotility, and severe Raynaud’s phenomenon (RP) complicated by recurrent digital ulcers, gangrene and autoamputation. Her serology is significant for positive antinuclear antibody, and anticentromere antibody.
During her disease course, she received different regimens of vasodilators including nifedipine, losartan, and topical nitroglycerin in addition to aspirin, with inadequate response. In May 2010 she presented with a refractory ulcer in the right third digit. Despite increase in her vasodilator therapy and addition of pentoxifylline, it progressed to diffuse ulceration of the digit, extending proximal to the distal interphalageal joint. Magnetic resonance imaging revealed no evidence of osteomyelitis. It was decided to admit her to hospital for intravenous (IV) prostaglandin.
After she received a 3-day course of continuous IV alprostadil, the ulcer size and pain improved significantly. On Day 3 of the alprostadil infusion, she developed coffee-ground emesis and a diminished hemoglobin, from 127 to 96 g/l. Endoscopy revealed severe esophagitis, esophageal ulceration, and appearance of the stomach consistent with gastric antral vascular ectasia (GAVE). A previous endoscopy in February 2008 at the same institution had not shown any of these findings. She was treated with transfusion of 2 units of packed red blood cells, intravenous pantoprazole, and discontinuation of the alprostadil. The bleeding stopped and her hemoglobin stabilized at a level of 120 g/l. She was discharged in stable condition.
SSc is an autoimmune disease characterized by progressive fibrosis of the skin and internal organs associated with vascular dysfunction. RP is one of the cardinal features of SSc, which can be disabling and difficult to treat. IV prostaglandins have been shown to be effective in treating resistant digital ulcers related to RP1. The precise mechanism by which clinical benefit is produced is unclear. Prostaglandins produce inhibition of platelet aggregation, vasodilatation, and smooth-muscle proliferation through a G protein-coupled receptor linked to adenylate cyclase2; they promote fibrinolysis by reducing plasma concentrations of tissue-type plasminogen activator and plasminogen activator inhibitor-13. Additionally, longterm therapy reduces the level of factor VIII and von Willebrand factor4, causing further inhibition of the coagulation cascade, all of which may contribute to clinical benefit.
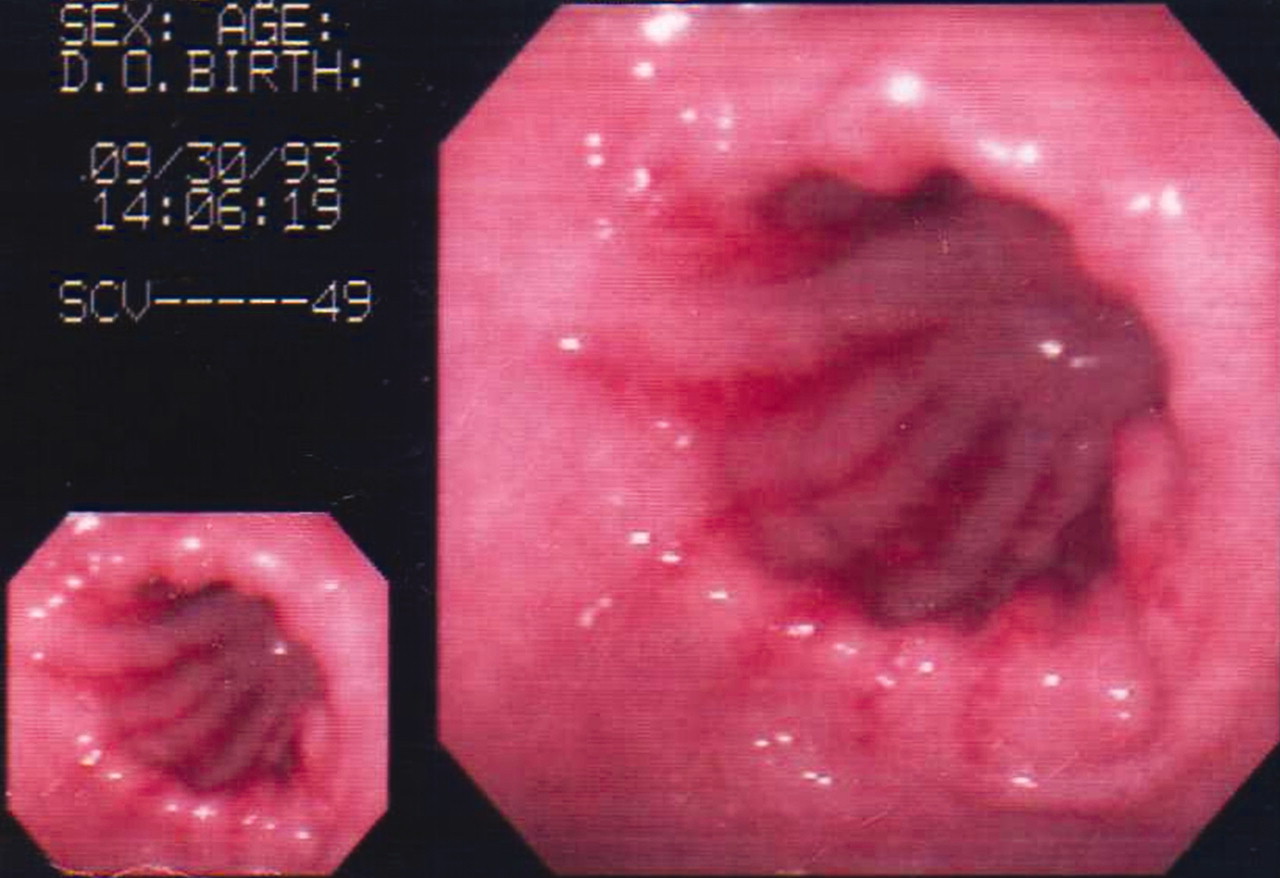
Involvement of the gastrointestinal (GI) tract in SSc patients is extremely common, reaching up to 90%5. The predominant causes of GI bleeding in SSc patients include mucosal telangiectasia, peptic ulcer disease, erosive gastritis, and GAVE. The occurrence of major GI bleeding is associated with an increased mortality6. GAVE is a rare and important cause of chronic anemia in SSc patients, with an estimated prevalence ranging from 2% to 5.7%7,8. Occasionally it can cause acute upper GI bleeding requiring endoscopic and surgical intervention. Patients usually have other vasculopathic manifestations including cutaneous telangiectasia, digital ulcers, systemic hypertension, pulmonary arterial hypertension, and/or renal crisis7. The distinctive endoscopic pattern of GAVE is classically described as erythematous streaks on the longitudinal rugal folds traversing the antrum of the stomach and converging on the pylorus. As these streaks resemble the stripes on the outside rind of a watermelon, this condition is also known as “watermelon stomach”7 (Figure 1). Endoscopic biopsy specimens demonstrate mucosal dilated capillaries containing fibrin thrombi, reactive epithelial changes, and fibromuscular hyperplasia of the lamina propria9. Similarities between the vascular changes of GAVE and SSc suggest that watermelon stomach may represent a component of the spectrum of vascular alterations in SSc10. Initial endoscopic evaluation can be unrevealing, but the findings during bleeding can be impressive. The time of presentation is usually variable, presenting early in the diffuse and late in the limited subtypes, and may be affected by other confounding factors like the use of nonsteroidal antiinflammatories, steroids, and proton pump inhibitors7.

{kind=link}
Endoscopic view of GAVE shows characteristic erythematous streaks resembling watermelon rind.
To our knowledge, this is the first case report of an association between IV prostaglandin and GAVE. IV prostaglandins may precipitate bleeding from high-risk vascular lesions in the GI tract of SSc patients through their vasodilatory effects, inhibition of platelet aggregation, and promotion of fibrinolysis. Identification of high-risk patients with chronic anemia or previous GI bleeding, close monitoring for occult blood loss, and early intervention is strongly recommended prior to use of these agents.
Acknowledgment
The authors thank Dr. Peter Lee for providing the photograph of GAVE.
Footnotes
-
Dr. Johnson has been awarded a Canadian Institutes of Health Research Clinician Scientist Award and is supported by the Norton-Evans Fund for Scleroderma Research.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.