
Abstract
Objective. Systemic-onset juvenile idiopathic arthritis (systemic JIA) and macrophage activation syndrome (MAS), the most devastating complication of systemic JIA, are characterized by abnormal levels of proinflammatory cytokines. Interferon regulatory factor 5 (IRF5) is a member of the IRF family of transcription factors, and acts as a master transcription factor in the activation of genes encoding proinflammatory cytokines. Polymorphisms in the IRF5 gene have been associated with susceptibility to autoimmune diseases such as systemic lupus erythematosus (SLE) and rheumatoid arthritis. Our aim was to assess associations of IRF5 gene polymorphisms with susceptibility to systemic JIA and MAS.
Methods. Three IRF5 single-nucleotide polymorphisms (rs729302, rs2004640, and rs2280714) were genotyped using TaqMan assays in 81 patients with systemic JIA (33 with MAS, 48 without) and 190 controls.
Results. There were no associations of the IRF5 gene polymorphisms or haplotypes under study with susceptibility to systemic JIA. There was a significant association of the rs2004640 T allele with MAS susceptibility (OR 4.11; 95% CI 1.84, 9.16; p = 0.001). The IRF5 haplotype (rs729302 A, rs2004640 T, and rs2280714 T), which was reported as conferring an increased risk of SLE, was significantly associated with MAS susceptibility in patients with systemic JIA (OR 4.61; 95% CI 1.73, 12.3; p < 0.001).
Conclusion. IRF5 gene polymorphism is a genetic factor influencing susceptibility to MAS in patients with systemic JIA, and IRF5 contributes to the pathogenesis of MAS in these patients.
- INTERFERON REGULATORY FACTOR 5
- POLYMORPHISMS
- MACROPHAGE ACTIVATION SYNDROME
- JUVENILE IDIOPATHIC ARTHRITIS
Systemic-onset juvenile idiopathic arthritis (systemic JIA) is one of the most perplexing diseases in childhood, manifesting as spiking fever, rash, arthritis, pericarditis, and hepatosplenomegaly1.
The systemic symptoms frequently recur in conjunction with exacerbation of the arthritis symptoms. Some studies have observed that abnormal expression of the proinflammatory cytokines such as interleukin 6 (IL-6) and IL-1ß was characteristic of systemic JIA2,3.
The most devastating complication of JIA is macrophage activation syndrome (MAS), which is strongly associated with systemic JIA, but rarely with polyarthritis4. MAS is accompanied by serious morbidity and sometimes death. The increased levels of several proinflammatory cytokines such as interferon-γ (IFN-γ), tumor necrosis factor-α (TNF-α), and others correlate with the rapid development of clinical symptoms and the progression of abnormal laboratory measurements4,5. MAS closely resembles a reactive or an acquired form of familial hemophagocytic lymphohistiocytosis, considered to be caused by diminished natural killer (NK) cell function, and mutations of perforin (PRF1), UNC13D, and STX11 genes6. Because patients with systemic JIA have decreased levels of perforin in NK cells and diminished NK cell function, it was recently suggested that PRF1 mutations also play a role in the development of MAS in patients with systemic JIA7,8,9. Munc13-4 polymorphism was also associated with MAS in patients with JIA10. There is a clinical impression, however, that there are at least 2 subsets of patients with systemic JIA, one never experiencing MAS and the other with recurring MAS.
Interferon regulatory factor 5 (IRF5) is a member of the IRF family of transcription factors, and is known to have a crucial role in the Toll-like receptor (TLR) signaling pathway11. The activation of TLR is central to innate and adaptive immunity. IRF5 acts as a master transcription factor in the activation of proinflammatory cytokine genes. In IRF5-knockout mice, a severely impaired induction of IL-6, IL-12, and TNF-α was observed11. Recent investigations revealed associations of single-nucleotide polymorphism (SNP) in the IRF5 gene with susceptibility to systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA)12,13. Thus, IRF5 has a regulatory potential for proinflammatory cytokines in certain inflammatory diseases that manifest with abnormal expression of proinflammatory cytokines.
We hypothesized that polymorphisms in the IRF5 gene may constitute the genetic differences between the 2 tentative subsets of systemic JIA. We found a close relationship between IRF5 gene polymorphism/haplotype and susceptibility to MAS in patients with systemic JIA.
MATERIALS AND METHODS
Study population
Patients were eligible if they met the International League of Associations for Rheumatology classification criteria for systemic JIA14. A total of 81 children, 40 boys and 41 girls, enrolled in this study were followed at the Yokohama City University Hospital between December 2007 and December 2009. The mean age of the patients was 4.7 years at onset of systemic JIA. The observation period of patients without MAS was at least 25 months, with a mean observation period of 102.2 months (range 25–284 mo).
Patients were diagnosed as having MAS based on the clinical symptoms and laboratory abnormalities as suggested in the preliminary diagnostic guidelines for MAS complicating systemic JIA15, as follows: (1) clinical criteria including central nerve dysfunctions, hemorrhages, and hepatomegaly; and (2) laboratory criteria including decreased platelet counts (< 26.2 × 109/l), elevated levels of aspartate aminotransferase (> 59 U/l), decreased white blood cell counts (< 4.0 × 109/l), and hypofibrinogenemia (< 2.5 g/l). The diagnosis of MAS requires the presence of 2 or more criteria. Evidence of hemophagocytosis in bone marrow aspirates was sought only for confirmation of doubtful cases.
We conducted our study in accordance with the Declaration of Helsinki and with the approval of the Ethics Committee of the Yokohama City University School of Medicine. Written informed consent was obtained from each patient and/or their guardians.
Genotyping
Three SNP (rs729302, rs2004640, and rs2280714) in the IRF5 gene were selected based on previous research associating them with SLE and RA12,13. The patients with systemic JIA (n = 81) and 190 healthy controls were genotyped. Genomic DNA was isolated from peripheral blood using the QIAamp DNA Mini kit (Qiagen K.K., Tokyo, Japan). Genotyping was performed using the TaqMan SNP Genotyping Assays (AB assay ID: C_2691216_10 for rs729302, C_9491614_10 for rs2004640, and C_2691243_1 for rs2280714). These SNP were analyzed by real-time polymerase chain reaction (PCR) using the AB7500 Real Time PCR system (Applied Biosystems, Foster City, CA, USA) under the conditions recommended by the manufacturer. The TaqMan SNP Genotyping Assay for rs2004640 was performed by TaqMan gene expression master mix instead of by TaqMan genotyping master mix. Results of genotyping at rs2004640 by TaqMan gene expression master mix were consistent with results from direct sequencing, while results by TaqMan genotyping master mix were not consistent with results from direct sequencing. The rs41298401 SNP, located 6 base pairs downstream of rs2004640, influenced these conflicting results, presumably because rs41298401 is in the base sequence annealing with TaqMan probe and causes the annealing to be insecure.
Allele discrimination was done using SDS software version 1.4 (Applied Biosystems). Confirmation of which bases were present for 5 cases of each genotype at each of these SNP sites of the genomic DNA sample was carried out using direct sequencing in the Applied Biosystems 3730xl and Sequence Scanner version 1.0 under the conditions recommended by the manufacturer.
Statistical analysis
The SNPassoc package using the R-language version 2.8 (R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org) was used to evaluate associations between systemic JIA/MAS and these SNP, by logistic regression analysis16. Haplotype phases and haplotype frequencies were estimated using the Expectation-Maximization algorithm as implemented in the haplostat package (minimum haplotype frequency: > 0.05; www.docstoc.com)17. Haplotype blocks were assessed using Haploview (The Broad Institute, Cambridge, MA, USA; www.broadinstitute.org). Logistic regression analysis was also performed to evaluate the association between systemic JIA/MAS and the IRF5 haplotypes. Association between MAS and IRF5 gene polymorphism was analyzed by Kaplan-Meier curves with log-rank test.
RESULTS
Of the 81 patients with systemic JIA, 33 (13 boys and 20 girls) developed MAS during the followup period, according to the preliminary diagnosis guideline (Table 1)15. The mean lengths of followup were 97.8 months in patients with MAS and 102.2 months in patients without MAS (Table 2). MAS was recognized at a mean of 24.8 months (range 0–166 mo) after the onset of systemic JIA. However, the remaining 48 patients did not develop MAS during the followup. Age at onset of systemic JIA (p = 0.92, Welch’s t test) and sex (p = 0.54, Fisher’s exact test) were not associated with susceptibility to MAS in our study population (Table 2).
The frequency of clinical, laboratory, and histopathological features of macrophage activation syndrome (MAS) in the preliminary diagnostic guideline15. Total number of patients was 81.
Clinical characteristics of patients with systemic JIA with or without macrophage activation syndrome (MAS).
The genotype frequencies for the 3 SNP of the patients with systemic JIA and the healthy controls were both in Hardy-Weinberg equilibrium (p > 0.05). These results were consistent with the findings of a recent Japanese population study18. None of the gene polymorphisms under study was associated with susceptibility to systemic JIA (Table 3).
Association of polymorphisms in the IRF5 gene with susceptibility to systemic juvenile idiopathic arthritis (JIA).
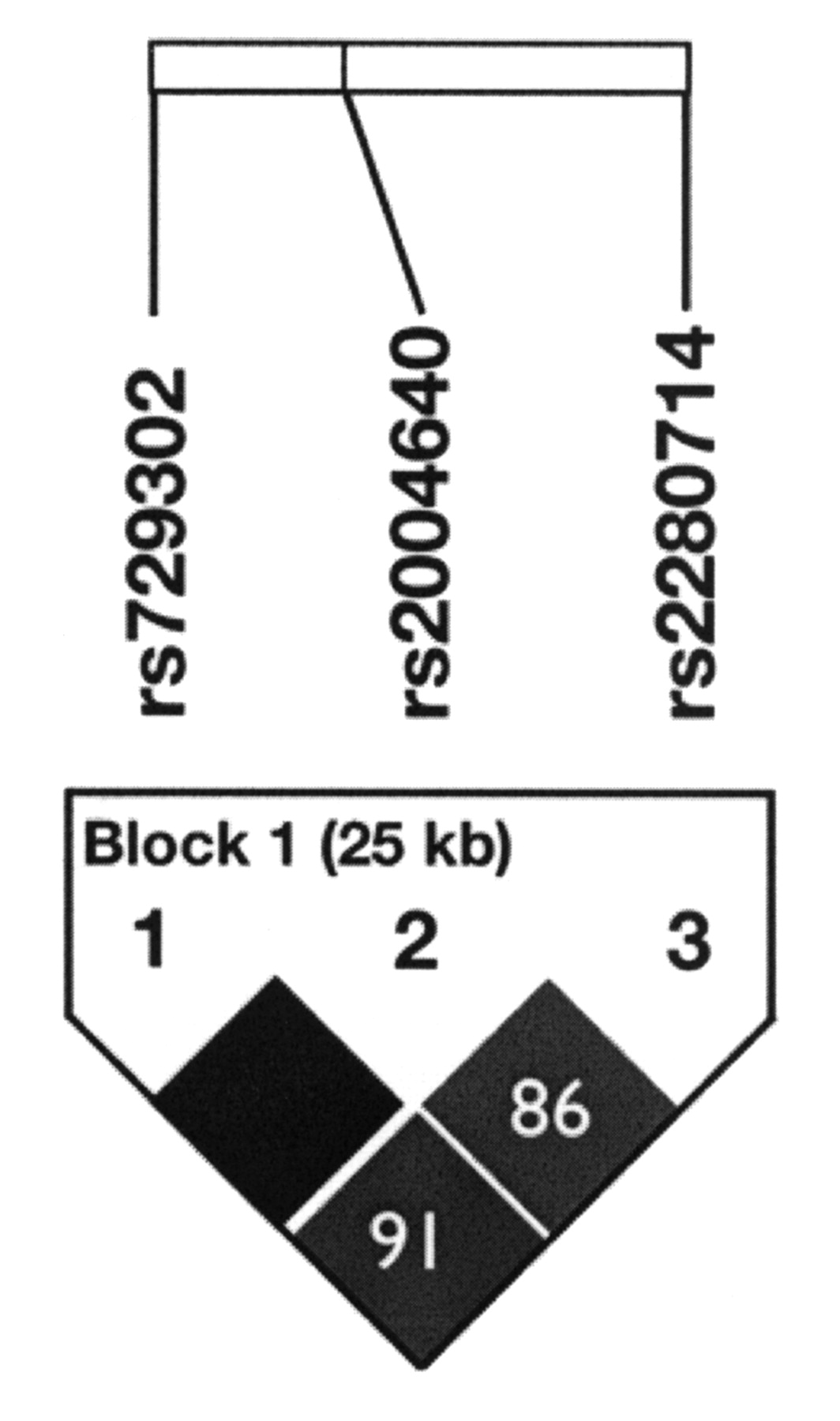
However, the rs2004640 SNP was found to be associated with MAS susceptibility (Table 4). Patients with the rs2004640 T allele had a high risk of developing MAS compared to those without this allele even after the Bonferroni correction (pc = 0.003, OR 4.12, 95% CI 1.84, 9.16). Moreover, all the patients with the TT genotype at rs2004640 finally developed MAS (Table 4, Figure 1). Patients carrying the TT genotype at rs2004640 had an early onset of MAS (a mean of 12.1 mo after onset of JIA). Additionally, the ATT haplotype of the IRF5 gene (rs729302-rs2004640-rs2280714) showed a statistically significant association with susceptibility to MAS (p < 0.001, OR 4.61, 95% CI 1.73, 12.3; Table 5). A haplotype block showed the correlation between the SNP genotyped (Figure 2).

Kaplan-Meier analysis of survival without macrophage activation syndrome and rs2004640 genotypes. JIA: juvenile idiopathic arthritis.
{kind=link}
{kind=link}
Haplotype blocks of interferon regulatory factor 5 gene polymorphisms.
Association of polymorphisms in the IRF5 gene with susceptibility to macrophage activation syndrome (MAS) in patients with systemic juvenile idiopathic arthritis (JIA).
Comparison of IRF5 haplotypes in patients with systemic juvenile idiopathic arthritis (JIA) with or without MAS. The order of SNP (single-nucleotide polymorphisms) in the haplotype is rs729302-rs2004640-rs2280714.
DISCUSSION
In the clinical setting, MAS apparently develops under the influence of systemic inflammatory responses of systemic JIA together with environmental factor(s), supposedly viral infection5. Susceptibility to these environmental factors may be subject to genetic influences. The combined presence of fairly frequent polymorphisms in multiple genes involved in the regulation of innate and adaptive immunity may be one of the major determinants in the initiation of rheumatic diseases19. To develop innate and adaptive immune responses, the activation of a TLR signaling pathway is essential. The transcription factor IRF5 is generally involved downstream of the TLR signaling pathway for induction genes for proinflammatory cytokines such as IL-6, IL-12, and TNF-α11,20. As mentioned, proinflammatory cytokines such as IFN-γ and TNF-α are responsible for the clinical and laboratory abnormalities seen in MAS4,5. Thus, we examined the association of polymorphisms in the IRF5 gene with susceptibility to MAS in patients with systemic JIA.
Our investigation revealed that the rs2004640 T allele and the ATT haplotype in the IRF5 gene were associated with MAS developing in patients with systemic JIA. All the patients with the TT genotype at rs2004640 had MAS, and they had an early onset of MAS compared to those with non-TT genotypes (Figure 1). While the ATT haplotype of the IRF5 gene was associated with susceptibility to MAS in patients with systemic JIA in our study, it was also reported that this is the common haplotype conferring increased risk of SLE12. The T alleles of both rs2004640 and rs2280714 were associated with higher levels of IRF5 messenger RNA expression12. Further, the other IRF5 haplotype was associated with high serum IFN-α activity in patients with SLE21. Although we did not address the association between proinflammatory cytokine activity and genotype/haplotype in the IRF5 gene, there may be the potential role of IRF5-associated immune response in the pathogenesis of MAS. Further research is needed to determine the influence of gene polymorphisms in the IRF5 gene on proinflammatory cytokine activities.
Although several drugs, such as tolmetin and tocilizumab, and viral infections were considered the triggering causes of MAS in our cohort, the triggers were not determined in most cases. All patients with MAS recovered from their severe complication. We could not find any association between IRF5 genotypes/haplotypes and the characteristics of clinical symptoms and severity of MAS in this study, presumably because of a small study population. We need a larger cohort to determine this association.
There are some limitations to our study. The incidence of MAS (40.7%) was significantly higher than generally seen (about 10%)4,5. Our hospital is one of the pediatric rheumatology centers in Japan and we have treated many patients with severe systemic JIA. The incidence of MAS is so high partly because of the characteristics of our hospital. In addition, there are ethnic differences in the incidence by the sub-types of JIA. Specifically, systemic JIA accounts for about 20% of JIA in Japan but for only about 10% in Europe and the United States22. Therefore there may also be ethnic differences in susceptibility to MAS.
A second issue is that we could not carry out a validation study. Although the genetic association study should be validated, the incidence of MAS complicating systemic JIA is too low to validate this association in a single institution. Therefore it is important for the association between the IRF5 genotype/haplotype and MAS susceptibility to be confirmed by other groups.
We found a strong association between polymorphisms in the IRF5 gene and susceptibility to MAS in patients with systemic JIA. This finding suggests a potentially important role of the IRF5-associated immune response in the pathogenesis of MAS.
Acknowledgment
We are grateful to T. Kaneko and S. Morita for advice on statistics. We also thank R. Tanoshima for secretarial assistance.
Footnotes
-
Supported by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (No. 16790583).
- Accepted for publication November 16, 2010.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.