
Abstract
Objective. Although osteoarthritis (OA) is generally assessed using standard radiographic images in clinical practice, biochemical markers can be used to detect the disease and determine its severity. Osteopontin (OPN) is an extracellular matrix glycoprotein that is a potential inflammatory cytokine. Presence of the thrombin-cleaved form of OPN is well correlated with various inflammatory diseases. We examined whether thrombin-cleaved OPN in synovial fluid (SF) and synovium could be associated with the severity of knee OA.
Methods. SF samples were obtained from 139 knees with OA. Thrombin-cleaved OPN product was determined using Western blotting. Levels of thrombin-cleaved and full-length OPN in SF were determined by ELISA. Synovium samples were analyzed by immunohistochemistry using an antibody specific to the thrombin-cleaved form.
Results. Western blotting showed the presence of thrombin-cleaved OPN in SF from patients with advanced OA. Concentrations of OPN full-length in OA knees were not statistically different from those in controls (p = 0.134). In contrast, levels of OPN N-half were significantly higher in OA knees than in controls (p = 0.042). Statistically significant correlation was found between thrombin-cleaved OPN and disease severity by Kellgren-Lawrence grade 1, 2, 3, and 4 (R = 0.274, p < 0.001). Immunohistochemistry of the synovium showed stronger reactivity in samples from subjects with advanced OA.
Conclusion. Local generation of thrombin-cleaved OPN was increased with greater OA severity.
- OSTEOARTHRITIS
- OSTEOPONTIN
- SYNOVIAL FLUID
- BIOMARKER
- THROMBIN
Although osteoarthritis (OA) is generally assessed using standard radiographic images in clinical practice1, biochemical markers can be used to detect the disease and determine its severity2. However, no marker has gained complete acceptance in clinical practice for monitoring progression of OA. The etiology of OA remains poorly understood, and several biochemical factors are involved in the pathogenesis. Levels of serum cartilage oligomeric matrix proteins seem to parallel the radiographic progression of OA3. We previously reported that synovial fluid (SF) levels of tenascin-C4, a matricellular protein, could be a biochemical marker of OA progression5.
Osteopontin (OPN), an extracellular matrix glycoprotein, is a potential inflammatory cytokine that modulates a variety of pathological conditions. OPN is a matricellular protein and is expressed in synovial tissue and cartilage from patients with rheumatoid arthritis (RA) and OA, suggesting a similar involvement in the pathogenesis of inflammatory arthritis as tenascin-C6,7,8,9. Expression of OPN was shown to be upregulated in OA cartilage and synovium. OPN could be involved in synovial cell attachment to chondrocytes or cartilage matrix, in addition to its involvement in destruction of cartilage matrix by the production of collagenases in articular chondrocytes7,9,10,11. Proteolytic modification of OPN by thrombin cleavage reveals cryptic binding sites for α9ß1 and α4ß1 integrins, preferentially expressed by neutrophils and by monocytes and lymphocytes, respectively12,13,14,15. The presence of the thrombin-cleaved form of OPN is well correlated with various inflammatory disease activities16. We measured SF levels of the N-terminal half of thrombin-cleaved osteopontin (OPN N-half) in RA directly, and demonstrated that OPN N-half levels were elevated in RA compared with OA17.
This cross-sectional study determined levels of OPN N-half and non-thrombin-cleaved osteopontin (OPN full-length) in SF from patients with OA. OPN N-half expression in synovium was also evaluated. We hypothesized that OPN N-half in SF and synovium may be associated with the severity of knee OA. To prove this hypothesis, we examined the SF and synovium levels of OPN N-half and evaluated a possible correlation between OPN N-half levels and radiographic grading of knee OA.
MATERIALS AND METHODS
Patients and samples
SF samples (n = 139) were obtained from 99 women and 40 men with primary OA of the knee at the time of surgery or before intraarticular injection of hyaluronic acid. All OA patients fulfilled the American College of Rheumatology clinical and radiological diagnostic criteria for OA18. Knee radiographs were evaluated according to the Kellgren and Lawrence (K-L) classification1 as follows: grade 1, doubtful narrowing of joint space and possible osteophytic lipping; grade 2, definite osteophytes and possible narrowing of joint space; grade 3, moderate multiple osteophytes, definite narrowing of joint space, some sclerosis, and possible deformity of bone contour; and grade 4, large osteophytes, marked narrowing of joint space, severe sclerosis, and definite deformity of bone contour. According to the K-L grading scale, 15 knees were K-L grade 1, 42 K-L grade 2, 41 K-L grade 3, and 41 K-L grade 4. Radiographic OA was considered present if K-L grade was more than 219. Knees with K-L grade 1 were defined as controls. All patients had serum C-reactive protein concentrations within the normal range for healthy adults. Subject characteristics are shown in Table 1. There was no difference between OA patients and controls in terms of age, sex, and body mass index (BMI). Synovium samples were obtained at the time of surgery in 38 patients with OA of the knee: 6 knees were K-L grade 2, 12 were K-L grade 3, and 20 were K-L grade 4.
Characteristics of the patients. Values are mean ± standard deviation except for sex.
All patients gave informed consent, and this study was approved by the local ethics committee.
Western blot analysis
Immunoblotting of SF was done to examine the presence of OPN N-half. From each SF sample, 0.15 ml was diluted twice with phosphate-buffered saline (PBS), added to 20 μl of DEAE Sepharose Fast Flow (GE Healthcare UK Ltd., Buckinghamshire, UK), mixed for 30 min at room temperature, washed 5 times with PBS, and then eluted with 1.0 ml of 0.7 M NaCl in PBS. The eluates were diluted twice with 2× sodium dodecyl sulfate (SDS) buffer (4% SDS, 20% glycerol, 125 mM Tris HCl, pH 6.8, 10% 2-mercaptoethanol), boiled, and applied on Western blotting with horseradish peroxidase-labeled anti-human OPN (O-17) rabbit IgG Fab’ (IBL, Gunma, Japan). Antibody (O-17) is raised against synthetic peptides corresponding to the internal sequence of mouse OPN (17LPVKVTDSGSSEEKLY32) and can bind both OPN full-length and OPN N-half20.
Enzyme-linked immunosorbent assay (ELISA)
SF was centrifuged at 15,000 g for 15 min, and the supernatants were stored at −80°C until analyzed. ELISA was applied to quantify the levels of OPN full-length and OPN N-half as described15. For the OPN N-half ELISA, Immuno Module Plates (Nalge Nunc, Rochester, NY, USA) were coated with anti-OPN N-half (34E3) mouse monoclonal antibody (in 0.1 M carbonate buffer, pH 9.5) at 4°C overnight, then blocked with 1% bovine serum albumin (BSA) in PBS containing 0.05% NaN3 at 4°C overnight. The mouse monoclonal antibody (34E3) specifically reacts to SLAYGLR and SVVYGLR, exposed by thrombin cleavage of mouse and human OPN, respectively. The OPN N-half ELISA system does not recognize full-length OPN and detects OPN after thrombin cleavage20. The specificity of the antibody (34E3) and ELISA was as described20. Sample and standard proteins were diluted with 1% BSA, 0.05% Tween 20 in PBS, added to each well, and incubated at 37°C for 1 h. After 7 washes with washing buffer (0.05% Tween 20 in phosphate buffer), 100 μl of horseradish peroxidase-labeled anti-human OPN (O-17) rabbit polyclonal antibody was added to each well and incubated 30 min at 4°C. After 9 washes with washing buffer, 100 μl tetramethyl benzidine buffer as a substrate was added to each well and incubated for 30 min at room temperature in the dark. Color development was stopped by addition of 100 μl stop solution (1 N H2SO4). The optical density of each sample was measured at 450 nm. To quantify the levels of non-thrombin-cleaved osteopontin (OPN full-length), a human osteopontin assay kit (IBL) was used with 2 antibodies (O-17 and 10A16). A mouse monoclonal antibody (10A16) is raised against synthetic peptides corresponding to the internal sequence of human OPN (155KSRSFQVSDEQYPDATDE172) and can bind to OPN full-length but not OPN N-half. The percentage of OPN N-half (% N-half) was then determined [OPN N-half divided by all OPN (OPN N-half plus OPN full-length)]17.
Immunohistochemistry
Expression of thrombin-cleaved OPN in synovium was determined by immunohistochemistry using the avidin-biotin complex method with anti-OPN N-half (34E3) mouse monoclonal antibody. Synovium samples were fixed in 10% buffered formalin, embedded in paraffin, and cut into 4-μm sections. After deparaffinization with xylene and rehydration through a series of graded ethanol solutions, the sections were pretreated in 10 mM citrate buffer, pH 6.0, in a microwave oven for 5 min for antigen retrieval. Sections were treated with superblock solution (Scytek Laboratories, Logan, UT, USA). After washing, sections were incubated in 0.3% H2O2 in methanol for 15 min to block endogenous peroxidase activity, blocked with 2% bovine serum albumin, and incubated with the primary antibody (34E3) overnight at 4°C. Sections were washed with PBS and reacted with the secondary antibody (biotinylated goat anti-mouse IgG antibody) for 1 h at room temperature. After washing, they were incubated with avidin-peroxidase complex for 30 min. Sections were then developed with diaminobenzidine tetrahydrochloride substrate solution and counterstained with hematoxylin. The results of immunoreactivity for synoviocytes and subintimal tissues were identified using the point system of Salter21, as follows. For synoviocytes, no staining = 0 point; staining of < 25% of synoviocytes = 1 point; staining of 25%–75% of synoviocytes = 2 points; and staining of > 75% of synoviocytes = 3 points. For subintimal tissues: no staining = 0 point; focal weak staining of subintimal tissues = 1 point; focal strong staining of subintimal tissues = 2 points; and extensive strong staining of subintimal connective tissue = 3 points.
Statistical analyses were performed using StatView for Windows version 5.0 (SAS Institute, Cary, NC, USA). The Mann-Whitney U-test was used to determine the differences between SF levels of OPN full-length, OPN N-half, and % N-half in OA patients and controls. Correlation analyses were performed for SF levels and disease severity using Spearman’s rank correlation test, and a multiple regression test was also used. Correlation between the immunohistochemical scores of synovium and disease severity were also estimated. P values < 0.05 were considered significant.
RESULTS
Expression of thrombin-cleaved OPN protein
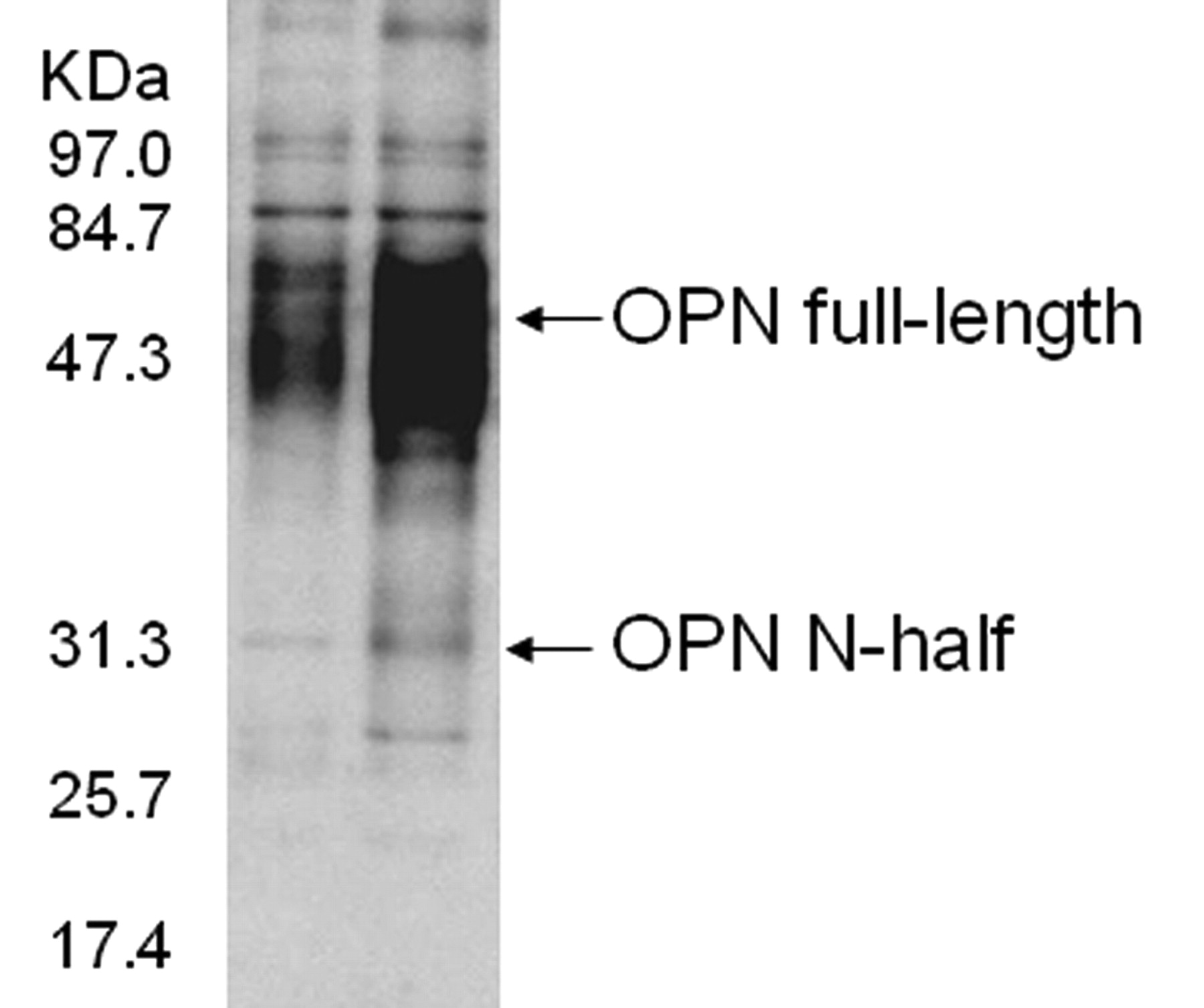
In SF from patients with OA, the antibody O-17 reacted with full-length and N-half OPN with molecular weights of 48 kDa and 30 kDa, respectively (Figure 1). These results showed that samples of OA SF contained full-length OPN, and that the level of N-half OPN was considerably elevated in patients with advanced OA (Figure 1, right lane), whereas a faint band was rarely detected in the early OA sample (Figure 1, left lane).

Representative Western blot analysis of synovial fluid. The antibody O-17 reacted considerably with bands around 48 kDa and 30 kDa in advanced OA (right lane). A faint band around 30 kDa was rarely detected in early OA (left lane).
ELISA
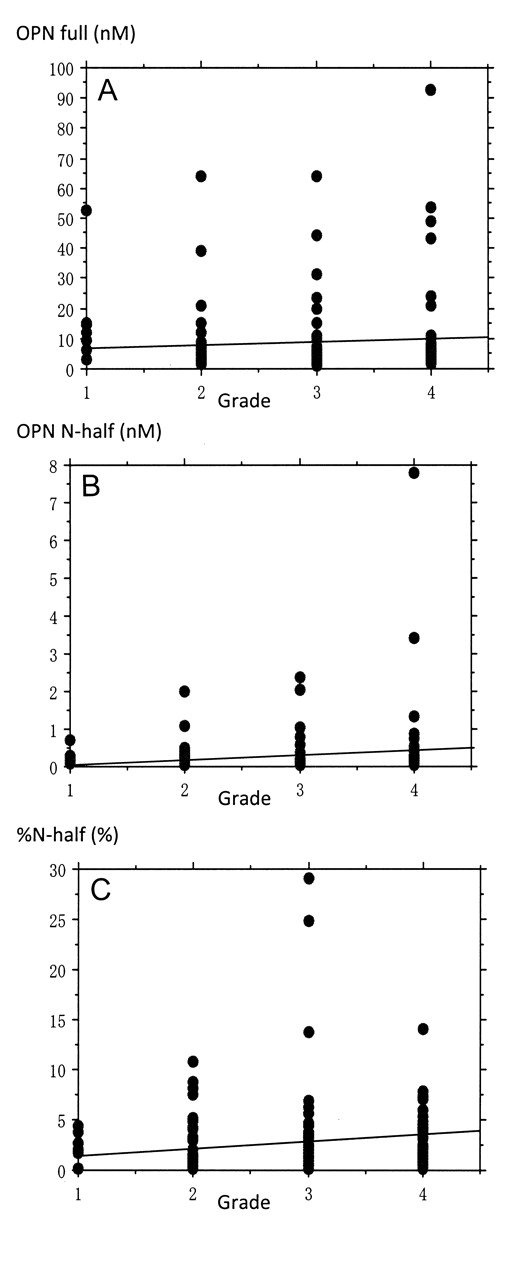
SF levels of OPN full-length, OPN N-half, and % N-half are shown in Figure 2. The levels of OPN full-length in OA knees were not statistically different from those in controls (p = 0.134; Figure 2A). In contrast, the levels of OPN N-half were significantly higher in OA knees than in controls (p = 0.042; Figure 2B). The % N-half increased significantly in OA knees compared to controls (p = 0.003; Figure 2C). In rank correlation tests, the SF levels of OPN full-length showed no difference (R = 0.111, p = 0.191; Figure 3A); however, the levels of OPN N-half and % N-half correlated with disease severity (R = 0.400, p < 0.001; Figure 3B, and R = 0.416, p < 0.001; Figure 3C, respectively). Apart from one clear outlier in K-L grade 4, showing extremely high concentration of OPN N-half (7.8 nM), OPN N-half levels correlated with disease severity (R = 0.282, p < 0.001). In addition, statistically significant correlation was found between OPN N-half and disease severity by K-L grade 1, 2, 3, and 4 (R = 0.274, p < 0.001). After adjusting the levels of OPN N-half as well as % N-half for sex and age, the correlation between % N-half and the radiographic grading levels remained statistically significant (R2 = 0.053, p = 0.015); however, the levels of OPN N-half showed no difference (R2 = 0.036, p = 0.089).

Levels of OPN full-length (A), OPN N-half (B), and % N-half (C) in synovial fluid from subjects with OA and controls. Lower and upper lines in the box represent 25th and 75th percentiles, and the median is shown. Bars show the range of 10th and 90th percentiles. *p = 0.134; **p = 0.042; ***p = 0.003.

Correlation of disease severity with synovial fluid levels of OPN full-length (A), OPN N-half (B), and % N-half (C).
Immunohistochemistry
Synovium samples showed positive labeling of OPN N-half in synovial lining cells and subintimal tissues in synovial samples from patients with OA (Figure 4). The mean scores of OPN N-half for synoviocytes were 0.67 ± 0.51 for grade 2 disease, 1.83 ± 0.71 for grade 3 disease, and 1.90 ± 0.72 for grade 4 disease. The mean scores for subintimal tissues for grade 2, 3, and 4 disease were 0.50 ± 0.55, 1.33 ± 0.49, and 1.35 ± 0.49, respectively. The scores of OPN N-half for synoviocytes and subintimal tissues correlated weakly with disease severity (R = 0.383, p = 0.020 and R = 0.358, p = 0.030, respectively).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Expression of OPN N-half in advanced OA synovium (A) and early OA synovium (B) (original magnification ×200).
DISCUSSION
We have demonstrated that SF concentrations of OPN N-half correlated with radiographic severity of OA. Elevated levels of OPN in the SF were possibly caused by either the release of OPN residing in the local tissues, including the synovium, articular cartilage, and bone, or the increase in its production, or both11,22. It is suggested that cell adhesion, migration, or inflammation could be involved in the release of OPN23. It is likely that the excessive production of cytokines and growth factors by the inflamed synovium and activated chondrocytes plays an important role in the pathophysiology of OA. Proinflammatory cytokines have been demonstrated to play a pivotal role in the development of the disease process. Tumor necrosis factor-α (TNF-α) and interleukin 1ß (IL-1ß) can stimulate their own production and induce chondrocytes and synovial cells to produce other cytokines and chemokines, including IL-6, IL-8, and matrix metalloprotease24,25,26. Previous studies have demonstrated that overexpression of OPN induces proinflammatory cytokines and chemokines, including IL-1ß, IL-6, IL-8, TNF-α, CXCL1, and CCL29,27. Sharif, et al28 reported that elevated levels of thrombin-cleaved OPN correlated with increased levels of multiple proinflammatory cytokines including TNF-α, IL-6, and IL-12p40, and chemokines IP-10 and eotaxin, whereas levels of OPN full-length did not correlate with levels of proinflammatory cytokines other than IL-6. Elevation of thrombin-cleaved OPN levels may play some role in a specific inflammatory response, including the pathogenesis of OA.
Our study demonstrated the immunohistochemical expression of OPN in the synovium and that synovium levels of OPN correlated with disease severity. Gao, et al11 reported OPN immunohistochemical staining in articular cartilage of knee OA, and the articular cartilage levels of OPN correlated with disease severity. Our study showed the SF levels of OPN N-half were correlated with disease severity, but the levels of OPN full-length were not. Two previous studies11,22 also showed that SF OPN levels significantly correlated with OA severity. The study by Honsawek, et al22 used the same commercial ELISA kit (IBL) that we used, and Gao, et al11 used another ELISA kit (Uscn Life Science & Technology Company, Wuhan, China). No description was given in either study of whether they used the kit for OPN full-length or OPN N-half. If the studies used the kit for OPN full-length, one possible reason for the difference in these results might be the molecular fragility of OPN. OPN can easily be cleaved into 2 fragments by thrombin, because the thrombin cleavage site is present in the OPN molecule.
In a previous study, we revealed that cartilage repair in tenascin-C knockout mice was significantly slower than that in WT mice and that the deficiency of tenascin-C progressed during cartilage degeneration29. In contrast, human SF levels of tenascin-C were shown to be elevated in OA in the advanced stage5. Matsui, et al30 demonstrated that OPN could be a critical intrinsic regulator of cartilage degradation and that OPN deficiency resulted in accelerated development of OA-like tenascin-C deficiency. These findings and our present results suggest remodeling of cartilage and synovium could play some role in the increased expression of OPN.
Limitations of this study include the cross-sectional design of the trial and lack of analysis of serum and urine levels of OPN N-half. We did not evaluate diurnal variations in SF levels of OPN. In addition, we could not obtain SF from a control group with completely healthy joints. The mean BMI in our study was low even in patients with K-L grade 4. We cannot directly generalize this finding to all ethnic groups. Therefore, our findings may not be applicable to heavy patients.
Our study showed that local generation of thrombin-cleaved OPN was increased with more severe OA, and our hypothesis was proved. Further investigations are needed regarding the relationship between SF and serum levels of OPN N-half as well as using some additional measures to evaluate severity of joint inflammation or symptoms.
Acknowledgment
The authors thank Dr. N. Kinoshita for contributing to the study design, and T. Iino for technical contributions.
- Accepted for publication September 1, 2010.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.