
Abstract
Objective. To determine the incidence and longitudinal trends of Wegener’s granulomatosis (WG) in the pediatric population of Southern Alberta over the last 15 years.
Results. Fifteen cases of childhood WG were confirmed. The average annual incidence was 2.75 cases/million/year, with a steep increase over the last 5 years to 6.39 cases/million/year.
Conclusion. In Southern Alberta the incidence of childhood WG during the past 15 years was comparable to the incidence reported in adults and it seems to be increasing. Further studies are required to determine if this is a regional or global phenomenon.
- WEGENER’S GRANULOMATOSIS
- CHILDREN
- INCIDENCE
Wegener’s granulomatosis (WG) is a systemic inflammatory disease that causes necrotizing vasculitis of small vessels. Classically, it affects the upper and lower respiratory tract as well as the kidneys. Detection of antineutrophil cytoplasmic antibodies (ANCA), in particular the cytoplasmatic form (c-ANCA), has been closely associated with WG1. The etiology of WG is unknown but staphylococcus infections and exposure to silica have been postulated as potential triggers2. The incidence of WG in the adult population has been well documented, with reported incidences ranging from 3 to 14 cases/million/year3–5. WG has been historically considered a disease of adults with very rare occurrence in the pediatric population6. Consequently, there have been no published reports on the incidence of WG in children except 1 from northern Sweden that included young adults (18–30 years of age), reporting an incidence of 0.5 cases/million per year7. The objectives of our study were to determine the incidence of childhood WG and to identify changing trends in the incidence of this disease over the last 15 years in a well defined pediatric population.
MATERIALS AND METHODS
Calculation of childhood WG incidence in Southern Alberta was based on the definition of Southern Alberta as the catchment area for the Alberta Children’s Hospital (ACH) in Calgary and validation of WG cases by a chart review of patients identified after searching all ACH inpatient and outpatient electronic databases from March 1993 onward.
The ACH is the sole tertiary-care pediatric referral center for 1.6 million inhabitants of Southern Alberta, Canada. Peripheral general hospitals provide limited pediatric care and all children requiring pediatric subspecialty attention are referred to the ACH or are managed by ACH physicians in outreach outpatient clinics. The catchment area served by the ACH during the study period was accurately defined by the regional health care administration system used in Alberta. Census-derived, regional, age-specific annual population statistics were obtained from Statistics Canad7a and the Alberta government7b.
ACH databases containing outpatient and inpatient diagnosis data were queried from March 1993 onward using International Classification of Diseases (ICD9) and ICD10 codes for Wegener’s granulomatosis, polyarteritis nodosa, Churg-Strauss, microscopic polyangiitis, and other necrotizing vasculopathies. The following free text search terms were also used: vasculitis, ANCA, antineutrophil, and Wegener. This search strategy identified all patients who had these diagnoses/terms mentioned in their inpatient or outpatient charts at any time since their presentation. Identifying patients who may have fulfilled criteria for WG but were never diagnosed or suspected as such was beyond the scope of our study.
Charts of identified patients were then reviewed for validation of WG diagnosis and data collection.
Inclusion criteria were (1) age at presentation younger than 18 years; (2) available documentation in the patient’s chart sufficient to satisfy the WG diagnostic criteria of the American College of Rheumatology8 or the European League Against Rheumatism/Paediatric Rheumatology European Society (EULAR/PReS)9; and (3) residence in the region for at least 5 years.
Exclusion criteria were insufficient documentation for validation of WG diagnosis, and patient/family refusal to be included in the study.
StatsDirect® 2.7.0 (StatsDirect Ltd., Altrincham, UK) software was used for statistical analysis; graphs were generated with SigmaPlot® 2.01. The average incidence of WG during the first 10 years of the study was compared to the incidence in the last 5 years using a chi-square analysis. Graphic representations of the absolute number of cases and the 3-year moving average of WG annual incidences among children in Southern Alberta were created.
Ethical approval was granted by the University of Calgary Research Ethics Board (E-21562).
RESULTS
Thirty-two patients were identified but only 15 met the inclusion criteria. Excluded patients were eventually diagnosed with the following diseases: 3 systemic lupus erythematosus, 1 Henoch-Schönlein purpura, 1 IgA nephropathy, 1 Kawasaki disease, and 1 juvenile dermatomyositis. Nine additional patients had various rashes that were suspected to represent vasculitis at presentation but eventually resolved without specific intervention and remained undiagnosed. The remaining patient of the excluded 17 had a diagnosis of suspected Wegener’s based on chest imaging studies demonstrating diffuse nodular lesions with granulomas on histology. However, the pulmonary lesions disappeared without specific treatment, ANCA levels were never elevated, and no other systemic involvement was demonstrated.
Demographic and clinical characteristics of included patients are summarized in Table 1. The average age at presentation was 12.7 years, with no significant gender difference.
Demographic and clinical characteristics of children diagnoses with Wegener’s granulomatosis in Southern Alberta in the last 15 years.
The overall average annual incidence of childhood WG in Southern Alberta over the last 15 years was 2.75 cases/million/year (95% CI 1.93–3.70). During the first 10 years of this period (1994–2003), the average incidence was only 0.93 cases/million/year (95% CI 0.41–1.70); however, during the past 5 years (2004–2008) it reached 6.39 cases/million/year (95% CI 4.37–9.03). A chi-square analysis comparing the average annual incidences in these 2 periods yielded a significant p value of 0.00402.
The absolute numbers of childhood WG cases are shown in Figure 1, while the 3-year moving average of WG annual incidences among children in Southern Alberta is illustrated in Figure 2.
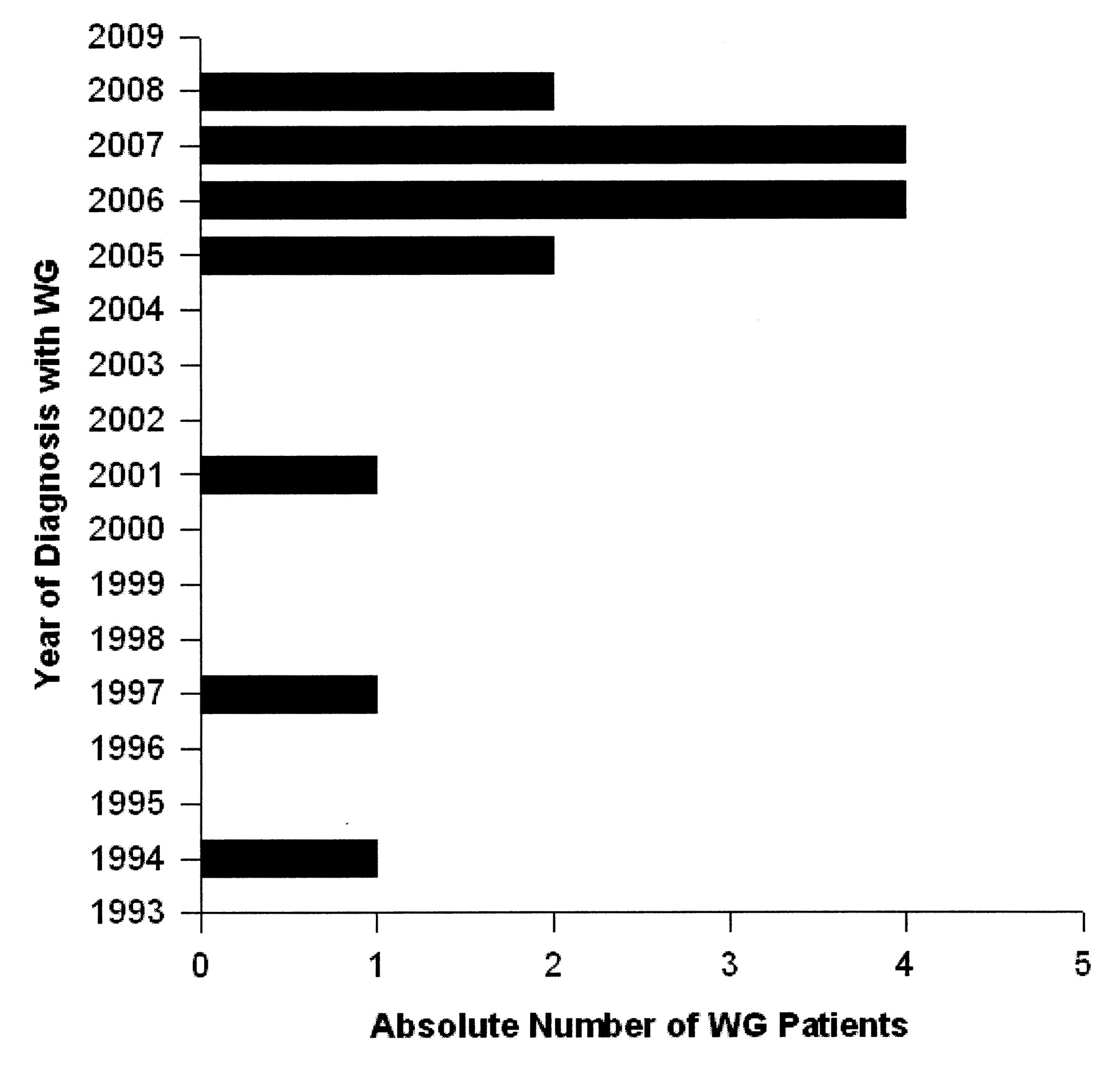
. Absolute numbers of childhood Wegener’s granulomatosis cases in Southern Alberta.

{kind=link}
{kind=link}
. The 3-year moving average of Wegener’s granulomatosis annual incidences among children in Southern Alberta.
DISCUSSION
This is a first population-based report on the incidence of childhood WG in Southern Alberta, demonstrating that the incidence of this disease there over the last 15 years was comparable to the incidence previously reported in adults3–5. In addition, a steep increase in the incidence of childhood WG in Southern Alberta, particularly during the last 5 years, was observed. Increasing incidence of WG among adults has been reported10,11. The results of this report support a similar observation in children.
We believe that these findings represent a real increase in incidence rather than improved recognition of childhood WG. Tests of serum levels of antineutrophil cytoplasmic antibodies (anti-PR3 and anti-MPO) have been readily available during the entire study period and we have not identified major changes in the diagnostic approach to suspected vasculitides during the study period at our center. Southern Alberta’s population increased significantly during the study period, with a disproportional advantage toward urban population growth. Previous reports found vasculitides in general to be more prevalent in urban areas12.
A thorough review of our cohort characteristics has not identified any previously published risk factors for WG such as exposure to infections or farming products2. Nevertheless, while searching for potential environmental factors associated with WG, we found that drinking water fluoridation was introduced in our region in 1991 after a plebiscite. This may be of interest, because the product used to increase fluoride levels of the water supply in our region is hydrofluorosilicate (H2SiF6), which dissociates thoroughly into free fluoride and silicate that can polymerize into stable colloidal silica at neutral pH13,14. Studies have suggested that exposure to silica may be a potential trigger for WG2,15.
Clearly, any correlation between exposure to silica in drinking water and WG is highly speculative; however, we believe it deserves further attention, particularly in view of the well documented regional variability in the prevalence of WG16.
We conclude that in Southern Alberta the average incidence of childhood WG is comparable to the reported incidence in adults, due mostly to a significant increase in the last 5 years. Retrospective and prospective surveillance studies from other regions in Canada and the rest of the world are required to clarify if our observation represents a regional or global phenomenon.
Footnotes
- Accepted for publication September 21, 2009.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 7a.
- 7b.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.