
Abstract
Objective. To examine whether plasma adiponectin level is correlated with osteonecrosis of the femoral head (ONFH).
Methods. Blood adiponectin level in patients with nontraumatic ONFH (n = 120) was compared with a group of healthy subjects (n = 120). Patients with hip osteoarthritis (OA; n = 30) and traumatic ONFH (n = 45) were included as controls. Potential compounding factors, such as plasma low-density lipoprotein (LDL), high-density lipoprotein (HDL), apolipoprotein A1 (apo A1), apolipoprotein B (apo B), total cholesterol (TC), triglycerides (TG), and C-reactive protein (CRP) were also examined.
Results. Patients with nontraumatic ONFH had significantly lower plasma levels of adiponectin than the healthy controls (7.14 ± 3.53 vs 10.93 ± 3.41 μg/ml, respectively; p < 0.001). Adiponectin level was positively correlated with HDL (r = 0.282, p < 0.001) and age (r = 0.145, p = 0.01), yet negatively correlated with body mass index (r = −0.70, p < 0.001), TG (r = −0.55, p<0.001), LDL/HDL ratio (r = −0.173, p = 0.002), and CRP (r = −0.634, p < 0.001). No correlation was seen with LDL (r = −0.017, p = 0.762). A multiple logistic regression analysis revealed that adiponectin level is an independent predictor of the presence of nontraumatic ONFH (p < 0.001, OR 0.676, 95% CI 0.546 to 0.845).
Conclusion. Low adiponectin level is significantly associated with the presence of nontraumatic ONFH. This biomarker may be useful in assessing the potential presence of nontraumatic ONFH.
- ADIPONECTIN
- OSTEONECROSIS
- FEMORAL HEAD
- ISCHEMIC
- BIOMARKER
Abnormal lipid metabolism and bone marrow fat cell hypertrophy/proliferation play important roles in nontraumatic osteonecrosis of the femoral head (ONFH)1,2,3. Fat emboli and/or thrombi may further compromise circulation to the femoral head4. In addition, repair capacity and bone remodeling play important roles in the progression and severity of nontraumatic ONFH5.
Adiponectin is a collagen-like cytokine produced by adipose cells. Human plasma concentration of adiponectin ranges from 5 to 30 μg/ml6. Adiponectin possesses antiatherogenic and antiinflammatory properties and can influence lipid metabolism7. Several lines of evidence suggest adiponectin could be used to predict ischemic diseases. A recent study reported a significant association between plasma adiponectin level and atherosclerotic burden8. Low adiponectin level may increase the vulnerability of acute coronary syndrome through coronary plaque formation9. Low plasma adiponectin has also been associated with increased mortality after ischemic stroke10. Recent studies have also implicated adiponectin in the regulation of bone metabolism11. Oshima, et al reported that adiponectin could increase bone mass by suppressing osteoclastogenesis and activating osteoblastogenesis12. Shinoda, et al suggested distinct adiponectin actions on bone formation13.
Based on these actions of adiponectin, we speculated that low blood adiponectin levels could be associated with nontraumatic ONFH.
MATERIALS AND METHODS
Patients and controls
One hundred twenty consecutive patients (146 hips; 68 women, 52 men) with nontraumatic ONFH treated at 6 hospitals across China (2 in Henan Province, 1 each in Wuhan, Chengdu, Tianjin, and Shanghai) from March 2009 to June 2009 were investigated. The mean age was 52.5 years (range 18–70). The diagnosis of nontraumatic ONFH was established on the basis of the clinical history and a combination of radiography, computer tomography, or magnetic resonance imaging. The distribution of ARCO (Association Research Circulation Osseous) stages14 was stage I in 63 hips, stage II in 51 hips, stage III in 28 hips, and stage IV in the remaining 4 hips. Patients were divided into 3 groups for analysis: a corticosteroid-associated group (n = 52), a group with alcohol-abuse history (n = 38), and an idiopathic group (n = 30)15. The mean cumulative dose of the corticosteroids in the corticosteroid-associated group was 5847 mg prednisolone or equivalent. Accordingly, we further divided the corticosteroid-associated group into a high-dose (> 6000 mg prednisolone; n = 22) and a low-dose subgroup (≤ 6000 mg prednisolone; n = 30)15. A study suggested that alcohol intake > 400 ml/wk increases the relative risk for nontraumatic ONFH15. We therefore further divided the alcohol-abuse group into a low-consumption group (≤ 400 ml/wk; n = 14) and a high-consumption group (> 400 ml/wk; n = 24).
Forty-five consecutive patients with traumatic ONFH and 30 patients with hip OA treated at the participating hospitals during the same period were included as controls. Those with secondary hip OA after collapsed osteonecrosis were excluded. Exclusion criteria in these 2 control groups also included the use of corticosteroids and/or alcohol. A group of 120 randomly selected healthy volunteers with no history of corticosteroid use and/or alcohol abuse were included as a negative control. Age and sex of the healthy controls were matched to those in the nontraumatic ONFH group. Underlying diseases that may affect adiponectin level (such as diabetes mellitus and hypertension) were also excluded16. None of the subjects was taking any type of thiazolidinedione, an insulin-sensitizing agent known to increase plasma adiponectin17. All subjects were screened by means of a detailed questionnaire, a medical history, and a physical examination. This study was approved by the Institutional Human Experiment and Ethics Committee of Wuhan Union Hospital, and was performed in accord with the 1964 Declaration of Helsinki. Written informed consent was completed by all participants.
Laboratory tests
Venous blood samples were obtained just after overnight fasting. Blood cells were removed by centrifugation at 1000 × g at 20°C for 20 min. Plasma samples were stored at −70°C until ELISA for adiponectin, using an ELISA kit (Cusabio Biotech, Wuhan, China). Plasma low-density lipoprotein (LDL), high-density lipoprotein (HDL), apolipoprotein A1 (apo A1), apo B, total cholesterol (TC), triglycerides (TG), and C-reactive protein (CRP) were measured in the hospital laboratory.
Statistical analysis
Data are expressed as mean ± SD or median value (25th to 75th percentile range). For comparison between 2 groups, data were analyzed by independent t-test. For 3 or more groups, data were examined using ANOVA, followed by the least significant difference test. Logistic regression and fully adjusted multivariate analyses were used to analyze the relationship. P < 0.05 was considered statistically significant. All statistical analyses were performed using the SPSS 13.0 software (Statistical Package for the Social Science).
RESULTS
Characteristics of the subjects
The mean age (± SD) in the nontraumatic ONFH group was 52.5 (± 12.0) years. The corticosteroid-associated group consisted of 43 women and 9 men, 18 to 70 years of age (51.8 ± 12.6 yrs). Conditions intended for corticosteroid treatment included aplastic anemia (n = 9), systemic lupus erythematosus (n = 16), idiopathic thrombocytopenic purpura (n = 13), nephritic syndrome (n = 11), and uveitis (n = 3). The alcohol-abuse group consisted of 1 woman and 37 men, 31 to 70 years of age (55.7 ± 12.2 yrs). The idiopathic group consisted of 24 women and 6 men, 22 to 64 years of age (51.5 ± 10.0 yrs). The healthy group consisted of 68 women and 52 men, 26 to 70 years of age (51.2 ± 10.1 yrs). The traumatic ONFH group consisted of 20 women and 25 men, 34 to 70 years of age (52.6 ± 9.6 yrs): 12 of these patients had femoral head fracture, 29 had antecedent femoral neck fracture, and 4 had fracture dislocation of the hip. The OA group consisted of 19 women and 11 men, 34 to 69 years of age (54.3 ± 8.4 yrs).
Adiponectin levels
The nontraumatic ONFH and the healthy controls did not differ in sex, mean age, and body mass index (BMI; p = 1.000, p = 0.377, and p = 0.200, respectively; Table 1). The plasma adiponectin level in patients with nontraumatic ONFH was significantly lower than that in healthy controls (7.14 ± 3.53 vs 10.93 ± 3.41 μg/ml, p < 0.001). Patients with nontraumatic ONFH had significantly higher levels of TG, CRP, and apo B/apo A1 ratio, and lower HDL levels in comparison with the healthy controls. Adiponectin level in the nontraumatic ONFH group was significantly lower than that in the traumatic ONFH group (p < 0.001) and the hip OA group (p < 0.001; Figure 1). There was no significant difference between the traumatic ONFH and hip OA groups.
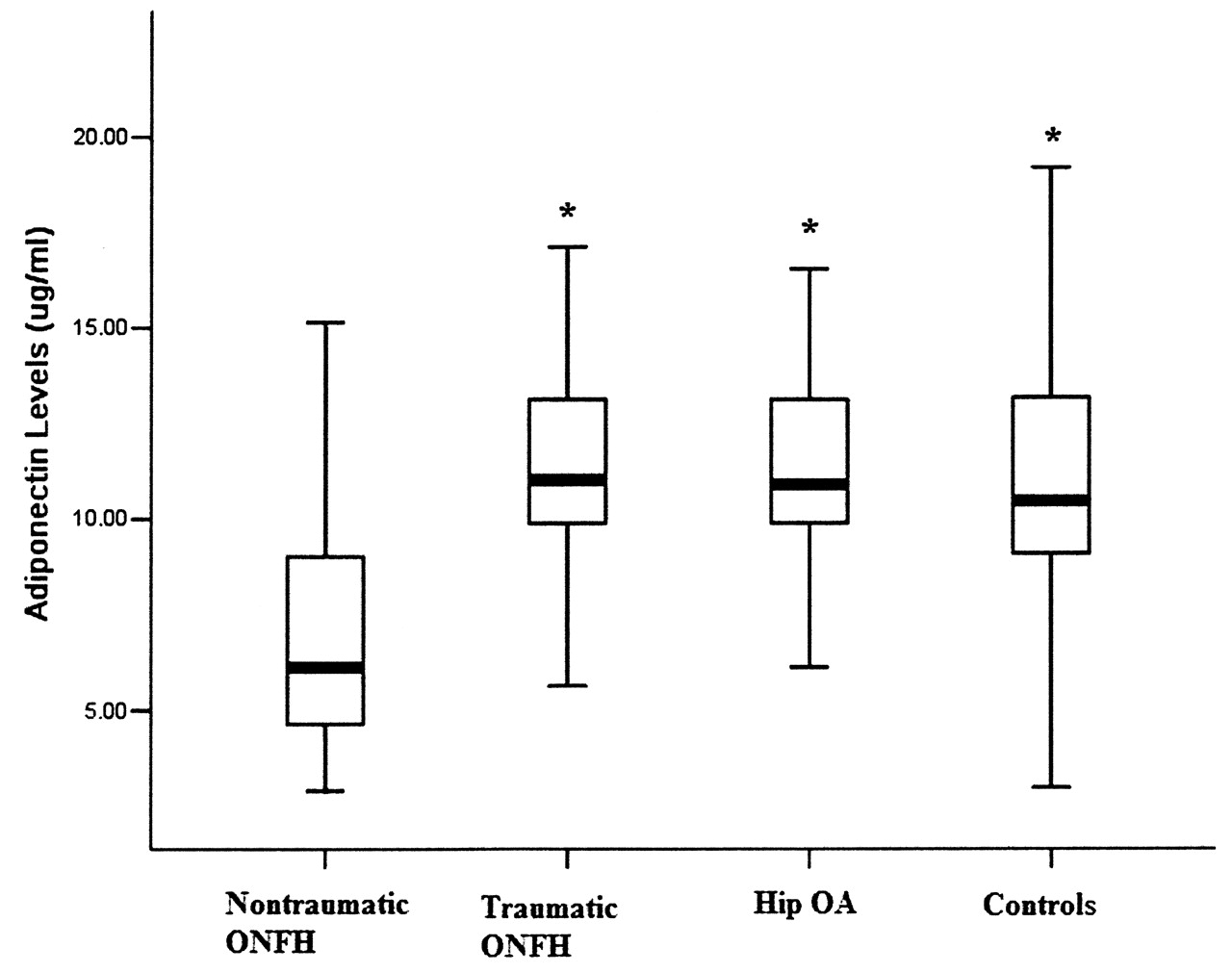
Plasma level of adiponectin in patients with nontraumatic osteonecrosis of the femoral head (ONFH; n = 120), traumatic ONFH (n = 45), and hip osteoarthritis (OA; n = 3), and healthy controls (n = 120). The adiponectin level in the nontraumatic group was significantly lower than in the traumatic group, the OA group, and the control group. *p < 0.001, but there was no significant difference among the latter 3 groups.
Baseline clinical characteristics and risk factors of patients with nontraumatic ONFH. Sex is listed as numbers of subjects, and the other factors are given as mean ± SD.
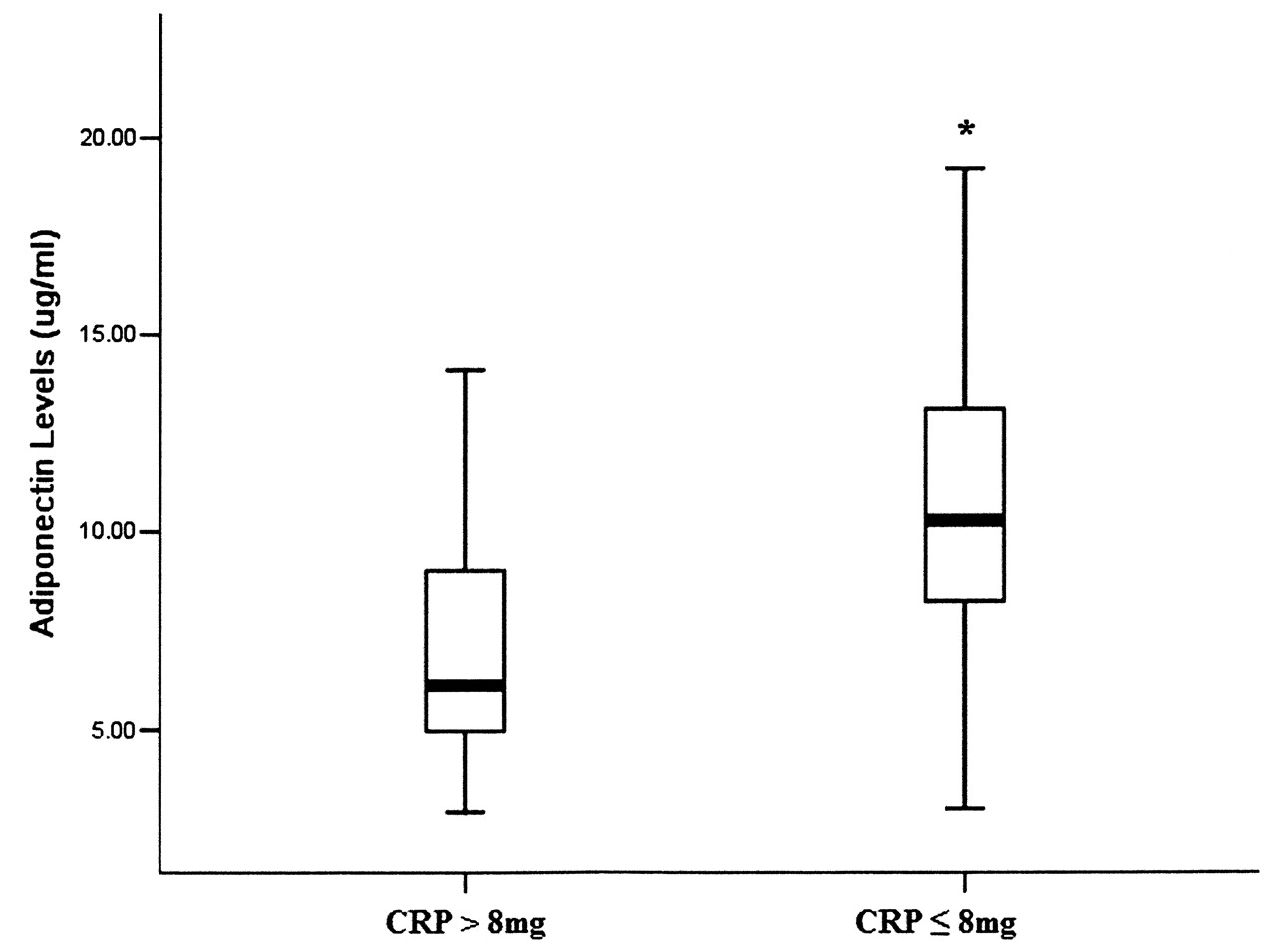
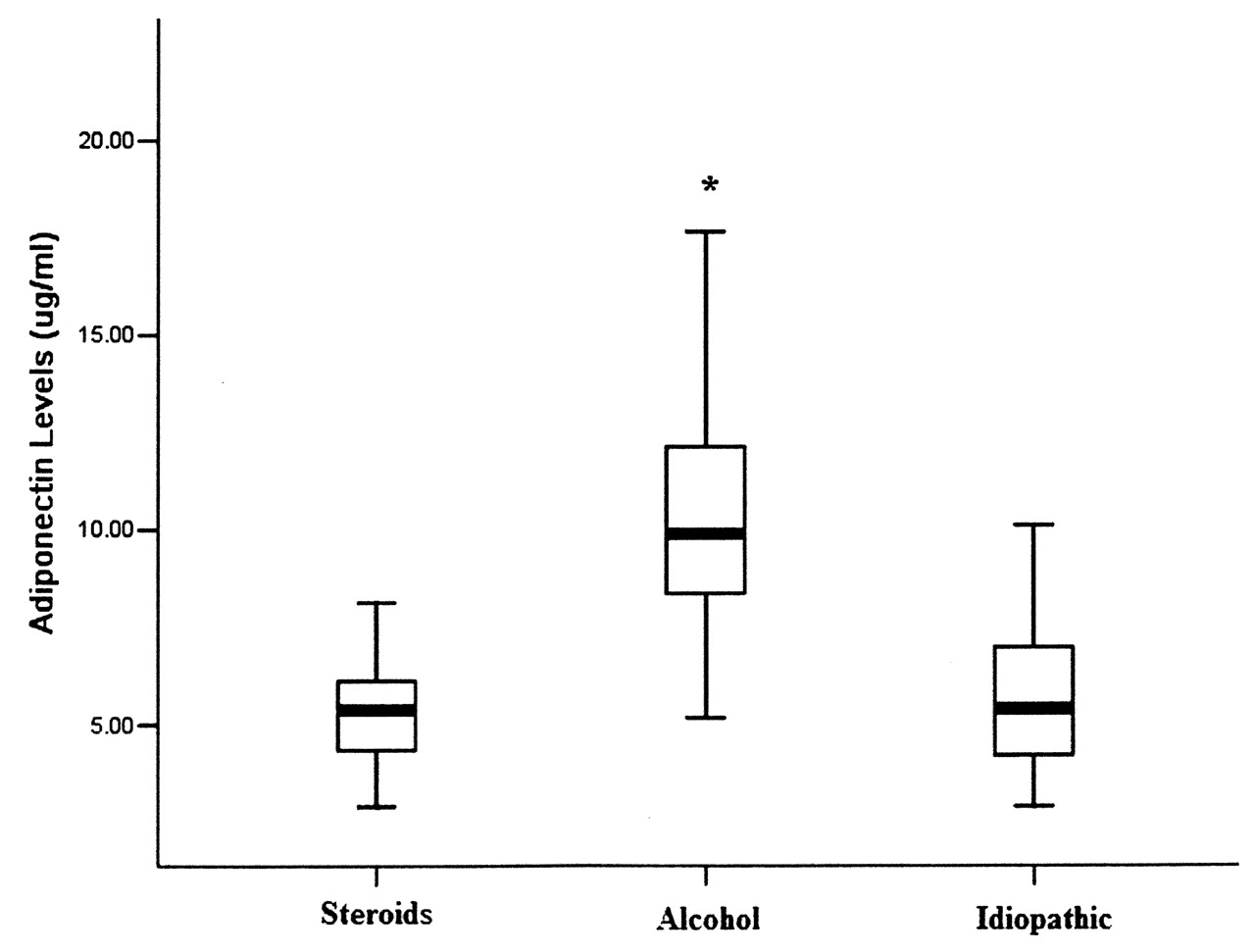
The adiponectin level in the alcohol-abuse group was significantly higher than in either the corticosteroid-associated group or the idiopathic group (Figure 2). The level was as high as in the control, traumatic ONFH, and OA groups (p = 0.715, p = 0.445, and p = 0.599, respectively). But there was no difference between low-dose and high-dose groups (9.32 ± 3.15 μg/ml for ≤ 400 ml/wk; 11.49 ± 4.09 μg/ml for > 400 ml/wk; p = 0.096). Corticosteroid dosage did not affect adiponectin levels (5.64 ± 1.48 μg/ml for ≤ 6000 mg; 5.22 ± 1.59 μg/ml for > 6000 mg; p = 0.340). The adiponectin level in the patients with nontraumatic ONFH who had elevated CRP (> 8 mg/l) was significantly lower than that in patients with normal CRP (7.30 ± 3.84 vs 10.47 ± 3.39 μg/ml; p < 0.001; Figure 3).

Median levels of adiponectin in 3 subgroups of patients with nontraumatic osteonecrosis of the femoral head (ONFH): a corticosteroid-associated group (n = 52); a group associated with alcohol abuse (n = 38); and an idiopathic group (n = 30). The level of adiponectin in the alcohol-associated group is significantly higher than in the other 2 groups. There is no significant difference between the corticosteroid-associated group and the idiopathic group. *p < 0.001.
{kind=link}
{kind=link}
{kind=link}
Median levels of adiponectin from the patients with elevated C-reactive protein (CRP; > 8 mg/l, n = 91) and normal CRP (n = 224). Level of adiponectin in patients with elevated CRP is significantly lower than in the normal CRP group. *p < 0.001.
Correlation between adiponectin and other nontraumatic ONFH risk factors
Plasma adiponectin level was positively correlated with HDL (r = 0.282, p < 0.001) and age (r = 0.145, p = 0.01), and negatively correlated with BMI (r = −0.70, p < 0.001), TG (r = −0.55, p < 0.001), LDL/HDL ratio (r = −0.173, p = 0.002), and CRP (r = −0.634, p < 0.001). Adiponectin was not correlated with LDL (r = 0.017, p = 0.762).
Low adiponectin was associated with the presence of nontraumatic ONFH
Simple logistic regression analysis showed that nontraumatic ONFH was associated with plasma adiponectin level (p < 0.001, OR 0.727, 95% CI 0.661 to 0.798), apo B/apo A1 ratio (p < 0.001, OR 1.274, 95% CI 1.218 to 1.333), LDL/HDL ratio (p = 0.012, OR 1.113, 95% CI 1.018 to 1.454), and CRP (p = 0.036, OR 1.336, 95% CI 1.005 to 1.701; Table 2). Multiple logistic regression analysis using a fully adjusted multivariate model revealed that nontraumatic ONFH was independently associated with plasma adiponectin (p < 0.001, OR 0.676, 95% CI 0.546 to 0.845), LDL/HDL ratio (p = 0.043, OR 1.108, 95% CI 1.009 to 1.507), and apo B/apo A1 ratio (p < 0.001, OR 1.269, 95% CI 1.209 to 1.333).
Logistic regression analysis for the presence of nontraumatic ONFH.
DISCUSSION
We demonstrated that patients with nontraumatic ONFH had signficantly lower plasma adiponectin levels in comparison to healthy controls as well as patients with traumatic ONFH or hip OA. More importantly, low plasma adiponectin was an independent predictor of the presence of nontraumatic ONFH. Plasma adiponectin was positively correlated with HDL levels and age and negatively correlated with BMI, TG, and CRP.
Adiponectin has been proposed as a biomarker for rheumatoid arthritis, obesity, type II diabetes, and certain ischemic diseases18,19,20,21,22. Several lines of evidence suggest adiponectin is neuroprotective. Efstathiou, et al showed an association between low plasma adiponectin with increased mortality after ischemic stroke10. Moreover, a study provided evidence that adiponectin has neuroprotective action through an endothelial nitric oxide synthase-dependent mechanism23.
Adiponectin plays a key role in inflammation and matrix degradation in the human joint24,25. The proinflammatory effects of adiponectin in human synovial fibroblasts appear to be selectively induced by interleukin 6 (IL-6) and matrix metalloproteinase-1 through the p38 5’-AMP-activated protein kinase (AMPK) pathway26. However, other studies have shown antiinflammatory properties of adiponectin27,28. Serelis, et al recognized an antiinflammatory role for adiponectin, and suggested that tumor necrosis factor-α is a key cytokine that regulates adiponectin level in patients with rheumatoid arthritis29. Adiponectin has been proposed as a biomarker and a site for therapeutic intervention in inflammatory joint diseases30. Our study revealed that low plasma adiponectin level is an independent predictor of nontraumatic ONFH.
More interestingly, the plasma adiponectin level of the alcohol-abuse group was significantly higher than that of the corticosteroid-associated group or the idiopathic group. It may be that moderate alcohol consumption increases adiponectin concentration, which is in line with some studies31,32. The mechanism of the difference is not clear, and there is no alcohol group of healthy controls for comparison. The forecast level of adiponectin in the nontraumatic ONFH group may be higher than that in the alcohol-abuse group. This needs to be confirmed in a more specialized study.
Several mechanisms may have contributed to the negative association between adiponectin and nontraumatic ONFH. First, adiponectin produces vasculoprotective effects through direct actions on endothelial cells, platelets, smooth muscle cells, and inflammatory cells, thus modulating initiation and progression of certain risk factors for ischemic necrosis of the femoral head (such as platelet-derived and endothelium-derived microparticles15, or thrombotic/fibrinolytic factors33, which might contribute to hypercoagulability and microthrombosis in patients with ONFH). Second, adiponectin may also improve lipid metabolism. Lipid transport from the central to peripheral tissues is enhanced by elevated serum LDL/HDL ratio, and resultant fat embolism compromises circulation within the bone marrow34. Several studies have associated nontraumatic ONFH, either drug-induced or idiopathic, with serum apo B/apo A1 ratio and LDL/HDL ratio35,36. Adiponectin inhibits the expression of the scavenger receptor class A-1 in macrophages, and therefore could significantly decrease uptake of oxidized LDL by macrophages37. Through activating AMPK, adiponectin stimulates phosphorylation of acetyl coenzyme-A carboxylase, fatty-acid oxidation, and glucose uptake. Adiponectin could also activate peroxisome proliferator-activated receptor-α, thereby also stimulating fatty-acid oxidation and decreasing tissue TG content38. In addition, adiponectin is present within normal bone marrow and can inhibit fat cell formation by marrow-derived stromal cells through a cyclooxygenase 2-dependent mechanism39. Finally, adiponectin could increase bone mass by suppressing osteoclastogenesis and activating osteoblastogenesis11,12.
Our study has several strengths and limitations. Our data support that adiponectin is an important biomarker of nontraumatic ONFH. However, since this was an association study, it did not establish a causal relationship between adiponectin and the presence of nontraumatic ONFH. In addition, we did not determine the cumulative corticosteroids dosage and alcohol consumption accurately. Levels were obtained by asking the patients. The clinical implications of our results still need to be determined.
We showed that adiponectin is significantly associated with nontraumatic ONFH. Low plasma adiponectin could potentially be used to predict events of nontraumatic ONFH.
Acknowledgment
The authors are grateful to the investigators and patients at the participating hospitals. Jing Li, Yan Li, Qingqing Chao, and Lan Gao also contributed to this study.
Footnotes
-
Supported by Excellence Future Inc., Beijing, China.
- Accepted for publication May 31, 2010.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.