
Abstract
Objective. To investigate the relationship of psychological distress and associated factors with continuation of tumor necrosis factor (TNF) antagonist therapy in patients with rheumatoid arthritis (RA).
Methods. Patients about to start therapy with TNF antagonists (n = 166) were assessed for psychological distress using the Hospital Anxiety and Depression Scale (HADS). A core set of demographic and clinical variables, including comorbidities from medical records and cigarette smoking history by questionnaire, were recorded at baseline and regular intervals thereafter. Cox proportional hazards regression analysis was used to assess the likelihood of patients discontinuing therapy over a 36-month followup period.
Results. The number of years smoked was associated with anxiety (HADS-A; p for trend = 0.008) and general psychological distress (HADS-Total; p for trend = 0.03). In univariate analyses, earlier discontinuation was associated with these variables at baseline: anxiety (HADS-A), depression (HADS-D), abnormal mood (HADS-Total), smoking history (> 30 pack-yrs), years smoked (> 30 yrs), current smoking, high Disease Activity Score 28-joint count (DAS28), poor patient global assessment, and evidence of cardio/cerebrovascular disease (CVD). In multivariate analyses, the strongest predictors of discontinuation were HADS-Total, smoking history (> 30 pack-yrs), DAS28, and evidence of CVD at baseline.
Conclusion. Discontinuation of therapy with TNF antagonists is independently associated with psychological distress, heavy smoking, and CVD at baseline.
- RHEUMATOID ARTHRITIS
- DEPRESSION
- STRESS
- TUMOR NECROSIS FACTOR INHIBITORS
- TOBACCO
Anxiety and depression occur commonly in patients with rheumatoid arthritis (RA) and can influence perception of well-being and severity of symptoms1,2,3,4,5. Recently we demonstrated that in patients with RA treated with tumor necrosis factor-α (anti-TNF), those with persistent depression had a lower reduction in the 28-joint count Disease Activity Score (DAS28) at 3 months than those without depression6. Cigarette smoking is also associated with a worse anti-TNF response7,8,9, but the relationship with psychological stress has not been explored.
Studies on the association of depression6 and smoking8 with response to TNF antagonists did not address their influence on discontinuation of treatment. We investigated the relationship between smoking and psychological distress, and whether these and other factors are independently associated with discontinuation of anti-TNF therapy.
MATERIALS AND METHODS
Patients attended a hospital clinic at the Staffordshire Rheumatology Centre, UK, and satisfied the 1987 American College of Rheumatology criteria for RA10. All patients starting therapy with TNF antagonists since 2002 (n = 166) were recruited. Ethical approval was obtained from the North Staffordshire local research ethics committee, and all patients provided written informed consent.
Demographic and clinical variables were recorded at baseline and regular intervals thereafter. Evidence of comorbid conditions were obtained from the medical notes and review of patient medication. History of cardiovascular or cerebrovascular disease (CVD) included angina, ischemic heart disease, myocardial infarction, heart failure, or cerebrovascular accident, but excluded hypertension. Probable anxiety and depression at baseline was defined using the Hospital Anxiety and Depression Scale (HADS)11, cutoff score of ≥ 812. Combining the scores of the 2 scales was used to obtain a “total score” as a measure of general psychological distress13.
Smoking history was obtained from a patient-completed questionnaire and quantified in pack-years (py); 1 py was equivalent to 20 cigarettes per day for 1 year. Py were stratified into 4 categories (i.e., 0, 1–15, 16–30, > 30) to reflect smoking intensity.
Discontinuation of therapy was investigated only in patients who were previously anti-TNF- or other biologic-naive, and was not assessed in those starting a second anti-TNF agent. The major reasons for discontinuation were adverse events or inefficacy (as defined by British Society for Rheumatology guidelines)14. All patients were followed up at 3 months, 12 months, and 12-monthly intervals thereafter. Of 166 patients recruited, 4 were excluded from the analysis because of incomplete or missing questionnaires.
Statistical analysis
The relationship between anxiety, depression, and smoking history was assessed using contingency tables, and multivariate logistic regression analysis. The relationship between baseline variables and discontinuation of therapy was investigated using Cox proportional hazard regression analyses.
Predictors of discontinuation were initially determined using univariate analyses. Variables with an unadjusted p value < 0.2 were carried forward for multivariate analysis. Kaplan-Meier curves were plotted to illustrate the proportion of patients remaining on therapy during the course of our study. All data were analyzed using the Number Cruncher statistical software package for Windows (NCSS, Kaysville, UT, USA).
RESULTS
Characteristics of patients with RA
Patients had a median age of 57.0 years, disease duration of 13 years, and 70% were women. Rheumatoid factor was present in 69.3% and erosions in 88.6%. Anxiety and/or depression was found in 48% of patients. Of 166 patients recruited, 76 were treated with infliximab, 62 with etanercept, and 28 with adalimumab.
Association of smoking with anxiety and depression
Current smokers at baseline were more likely to be anxious or depressed than patients who had never smoked (Table 1). Measures of psychological distress were more closely associated with the length of time smoked than py.
Relationship between smoking and Hospital Anxiety and Depression Scale (HADS) scores at start of anti-tumor necrosis factor therapy. Data analyzed using Mantel-Haenszel chi-square test for trend.
Predictors of discontinuation of therapy
Nearly 50% of patients (79/162) discontinued therapy during the 36-month followup period. Of these, 42/79 stopped due to inefficacy and 31/79 due to adverse events. The mean duration of therapy before discontinuation was 16.9 months.
In univariate Cox regression analyses of discontinuation for any reason, significant associations were seen with all measures of mood disorder, current smoking, py > 30, and smoking for > 30 years (Table 2). Associations were also found with the DAS28 total score, patient global assessment (PGA), erythrocyte sedimentation rate, and CVD. Similar associations were seen in patients stopping due to inefficacy alone (Table 2).
Univariate analysis of baseline predictors of anti-TNF discontinuation.
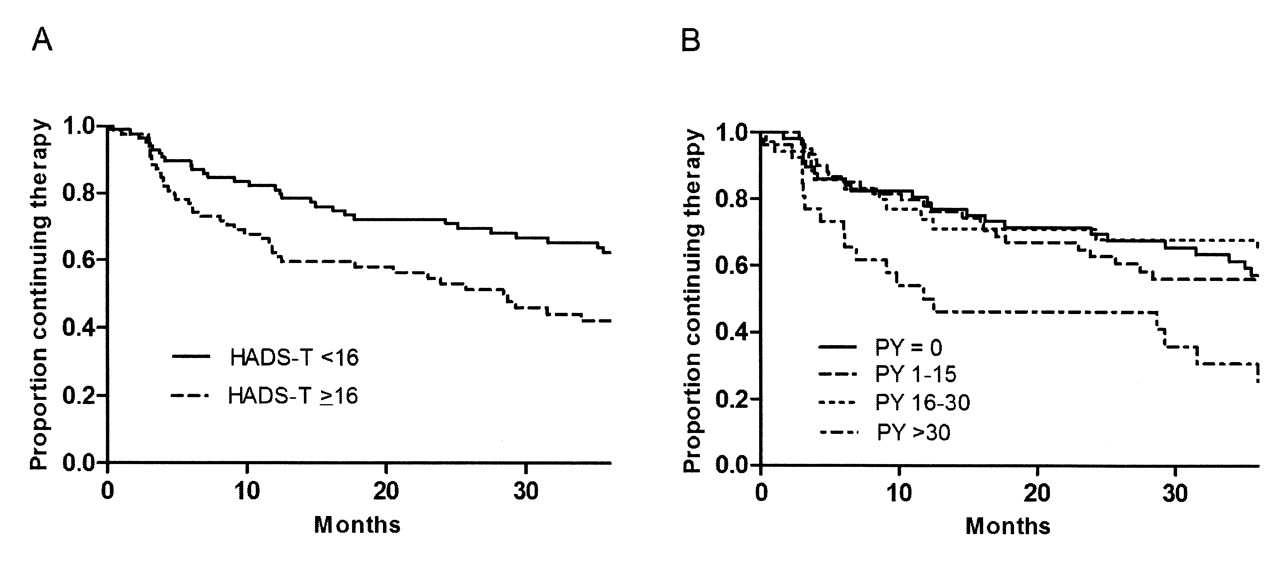
Kaplan-Meier curves showed that 50% of patients with psychological distress (HADS-T ≥ 16) had discontinued by 30 months, compared with about 35% of unaffected patients (Figure 1A). In patients with py > 30, 50% had discontinued treatment by 12 months compared with 20%–25% in those with py ≤ 30 (Figure 1B).

{kind=link}
Kaplan-Meier curves to illustrate the proportion of patients remaining on anti-TNF therapy in relation to (A) HADS-Total (HADS-T) and (B) cigarette pack-year (PY) category.
In multivariate analyses, the overall “best” model (hazard ratio) for discontinuation due to any reason included HADS-Total ≥ 16 (HR 1.68, 95% CI 1.06–2.67), DAS28 (HR 1.32 per unit, 95% CI 1.01–1.72), py > 30 (HR 2.90, 95% CI 1.70–4.95), and previous evidence of CVD (HR 2.45, 95% CI 1.30–4.62) as independent variables. The variables most strongly associated with stopping due to inefficacy were HADS-Total ≥ 16 (HR 2.23, 95% CI 1.18–4.22), py > 30 (HR 3.24, 95% CI 1.58–6.63), and CVD (HR 2.59, 95% CI 1.05–6.42).
DISCUSSION
Psychologically distressed patients (particularly depressed ones) were more than twice as likely to be current smokers at the start of anti-TNF therapy. Despite this relationship, psychological distress and py (> 30) were independently associated with discontinuation of anti-TNF therapy, as were a raised DAS28 and evidence of CVD at baseline. Discontinuation of anti-TNF treatment is clearly a complex, multidimensional endpoint that may be influenced by biological, emotional, and sociological factors15. It is possible that conditions linked to psychological distress (such as fibromyalgia) may have an influence on these findings, but patients were not assessed for fibromyalgia in our study.
Although CVD showed an association with ever having smoked (p = 0.03), it did not explain the association between py (> 30) and anti-TNF discontinuation, since both were highly significant in the multivariate analyses. Similarly, it is unlikely that association between psychological distress and anti-TNF discontinuation could be explained by the presence of CVD since the association between HADS-T and CVD was not significant (data not shown), while both were significant in the multivariate analyses.
It is interesting that the association of discontinuation with baseline DAS28 could be explained mainly by the PGA. The PGA is more likely to vary subjectively to external factors such as psychological distress. However, the correlation between PGA and HADS-T was weak (r = 0.27), and they were found to be independently associated with earlier discontinuation. This suggests that they are measuring different aspects of disease effect.
Our study reinforces the message that limiting smoking may be beneficial for continuation on anti-TNF therapies. It also suggests that preexisting psychological distress has a significant effect upon continuation of anti-TNF medication. Thus, in patients being considered for anti-TNF therapy, it would be useful to assess their psychological status. It may be that intervention with mood-enhancing therapies will subsequently be shown to improve the proportion of patients responding to and tolerating anti-TNF therapy.
Acknowledgment
We thank Michelle Kirwan (research nurse) and Janet Turner (research assistant) for their help with data collection and entry.
Footnotes
-
Funding by the Haywood Rheumatism Research and Development Foundation.
- Accepted for publication May 5, 2010.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.